
Abstract
Background:
Utilization of hospice has increased significantly over the past 2 decades, but there has been no recent assessment of US physicians’ opinions regarding and practices of referring patients to hospice.
Methods:
We surveyed 2016 US physicians from various specialties. Respondents agreed or disagreed with 2 statements: “For most patients, hospice provides better care at the end of life than they would otherwise receive without hospice” and “Many patients who enter hospice end up missing out on medical interventions from which they would have benefited.” Physicians were also asked, “In the past 12 months, approximately how many patients and/or their surrogates have you encouraged to consider entering hospice?”
Results:
Ninety-eight percent of physicians agreed that hospice provides better care at the end of life than the patient would receive without hospice. Only 11% of physicians agreed that patients who enter hospice miss out on medical interventions from which they would have benefitted. Ninety-two percent encouraged at least 1 patient to consider hospice in the previous 12 months. Oncologists were the most ambivalent about whether patients who enter hospice miss out on beneficial interventions, but they also referred more patients to hospice than physicians from other specialties.
Conclusion:
US physicians overwhelmingly believe hospice is the best form of care for most patients at the end of life. Compared to a study published in 1998, the median oncologist reports referring fewer patients to hospice, but the median general internist reports referring more.
Introduction
Two decades ago, Iwashyna and Christakis 1 conducted the only representative national study to date of US physicians’ opinions and practices regarding hospice care. In that, 89% of internists indicated that “hospice is an appropriate mode of care for most terminally ill patients,” and 84% had referred at least 1 patient to hospice in the previous year.
Around the time that study was fielded, the American Medical Association published a report titled, “Good Care of the Dying Patient,” 2 lamenting that, “In the current system of care, many dying persons suffer needlessly, burden their families, and die isolated from family and community” and calling for widespread expansion of hospice and palliative medicine. In the ensuing years, a new clinical subspecialty has been established, and the number of patients dying in hospice has increased markedly. 3 -5
We used data from a recent representative national survey to provide an updated assessment of US physicians’ practice of referring to hospice and the extent to which they believe hospice is not just an appropriate option but the better option for most patients at the end of life.
Methods
Study methods and characteristics of respondents have been published previously. 6 In 2010, we surveyed a representative sample of 2016 practicing US internists and family physicians, including an oversample of 768 physicians in subspecialties that care for disproportionate numbers of patients at the end of life (hospice and palliative care, geriatrics, oncology specialties, and pulmonary/critical care). The sample was generated from the American Medical Association Physician Masterfile, a database intended to include all practicing US physicians. Physicians received up to 3 separate mailings, with a US$20 cash incentive in the first and an offering of US$30 for participation in the third. All data were double keyed, cross-compared, and corrected against the original questionnaires. The study was approved by the University of Chicago institutional review board. All analyses included case weights to account for oversampling and modest differences in response rates by sampling strata. The method of case weighting—widely used in population-based research—enabled us to adjust for sample stratification and variable response rates in order to generate national estimates for the population of US physicians.
Respondents agreed or disagreed with 2 statements: “For most patients, hospice provides better care at the end of life than they would otherwise receive without hospice” and “Many patients who enter hospice end up missing out on medical interventions from which they would have benefited.” They were also asked, “In the past 12 months, approximately how many patients and/or their surrogates have you encouraged to consider entering hospice?” After excluding hospice physicians (n = 40), we analyzed data from 1116 respondents.
Results
Overall, 98% of physicians agreed (79% strongly) that for most patients hospice provides better care at the end of life than the patient would receive without hospice. Only 11% of physicians agreed (60% disagreed strongly) that many patients who enter hospice end up missing out on medical interventions from which they would have otherwise benefitted. Ninety-two percent had encouraged at least 1 patient or surrogate to consider hospice in the previous 12 months (median = 6; mean, standard deviation [SD] = 12.2, 0.7).
As seen in Table 1, male sex and younger age were modestly associated with strongly agreeing that hospice provides better care at the end of life, and men reported referring 3 more patients, on average, to hospice. Asian physicians were somewhat less likely to endorse hospice on both opinion measures. Oncologists appeared the most ambivalent about whether patients who enter hospice miss out on beneficial interventions (50% strongly disagreed, compared to 56%-67% of other specialties; P = .024 for oncologists vs other), but they also referred more patients to hospice (mean 27, median 20) than physicians in any other specialty.
Physician Attitudes Regarding Number of Referrals to Hospice by Physician Sex, Age, Race/Ethnicity, and Specialty.a
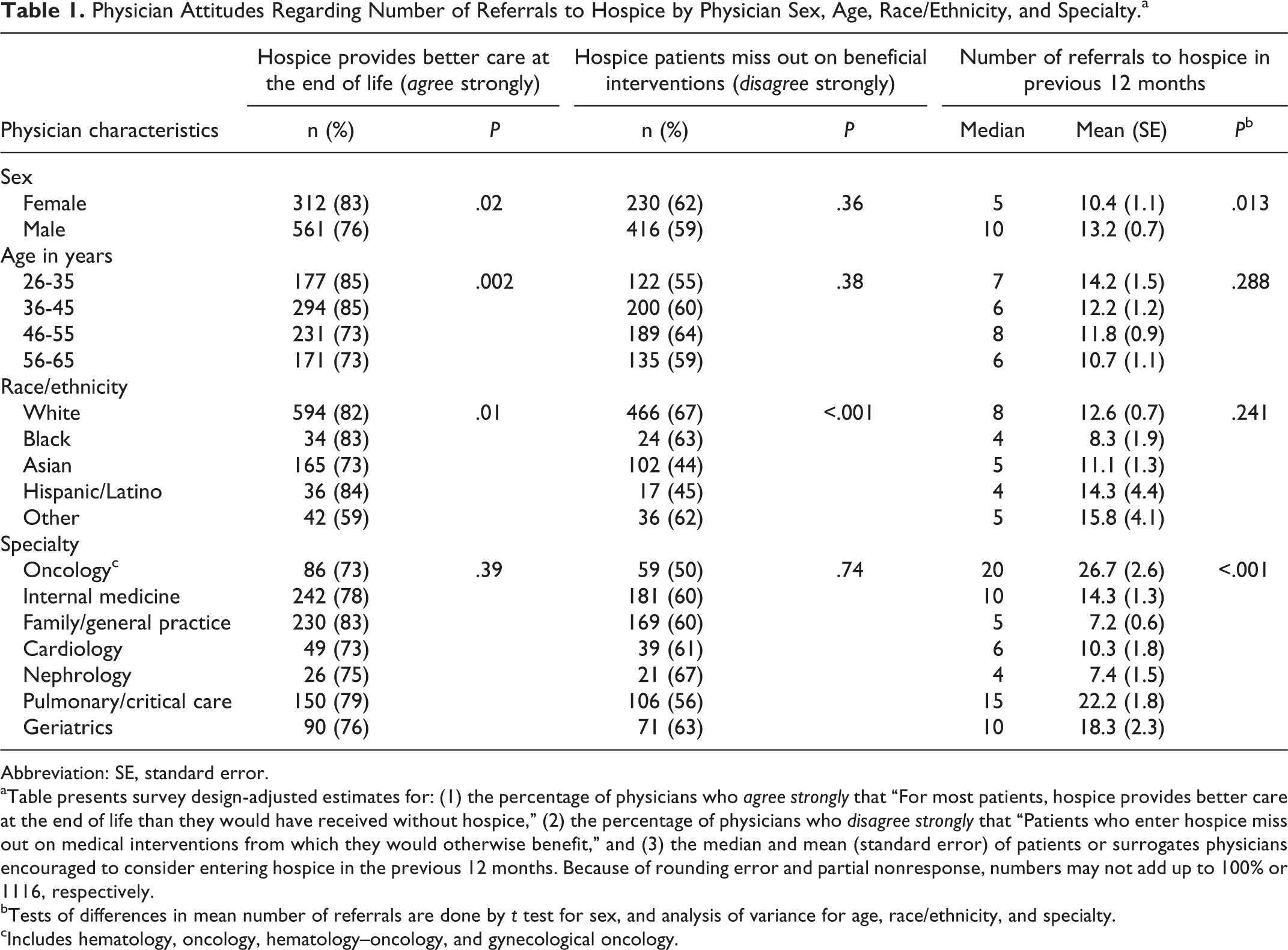
Abbreviation: SE, standard error.
aTable presents survey design-adjusted estimates for: (1) the percentage of physicians who agree strongly that “For most patients, hospice provides better care at the end of life than they would have received without hospice,” (2) the percentage of physicians who disagree strongly that “Patients who enter hospice miss out on medical interventions from which they would otherwise benefit,” and (3) the median and mean (standard error) of patients or surrogates physicians encouraged to consider entering hospice in the previous 12 months. Because of rounding error and partial nonresponse, numbers may not add up to 100% or 1116, respectively.
bTests of differences in mean number of referrals are done by t test for sex, and analysis of variance for age, race/ethnicity, and specialty.
cIncludes hematology, oncology, hematology–oncology, and gynecological oncology.
Conclusion
Though limited by the possibility of recall and other response biases, this study demonstrates that US physicians now overwhelmingly agree that hospice is the better form of care for most patients at the end of life. Compared to the study published in 1998, 1 the median general internist now reports referring twice as many patients (10 vs 5) to hospice each year, whereas the median oncologist appears to be referring roughly half as many (20 vs 38). Although the latter finding may raise worry about overly aggressive treatment of advanced cancer, 7 the former finding suggests that general internists and other primary care physicians may be more empowered than ever to refer patients diagnosed with advanced cancer directly to hospice, rather than deferring to oncologists about such referrals. Either way, that younger physicians are most enthusiastic suggests that hospice will increasingly become physicians’ preferred structure for caring for most patients at the end of life.
Footnotes
Acknowledgments
The authors thank Kenneth Rasinski and Annikea Miller for their assistance with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the John Templeton Foundation.