
Abstract
Aim:
Anger is a common reaction to cancer diagnosis which may impact patients’ perceptions of their prognosis and goals of care. This study tested the hypothesis that men with prostate cancer who are anger prone are pessimistic regarding their cancer prognosis.
Methods:
Two hundred and twelve men with a history of prostate cancer completed measures of personality traits, their prostate cancer prognosis, and their perception of their doctor’s assessment of their prognosis. Anger proneness was operationally defined by the presence of high levels (ie, above the medians) of neuroticism and disagreeableness.
Results:
One in 4 men with prostate cancer disagreed with their doctor about prognosis. Anger-prone participants endorsed more pessimistic perceptions of prognosis (P = .041). This significant association was maintained after accounting for potential confounders.
Conclusion:
Greater attention paid to patient anger regulation style and pessimistic perceptions will improve discussions about prognosis and goals of care among men with prostate cancer. Given recent calls for wider distress screening and earlier palliative care intervention in cancer settings, providers have an unprecedented opportunity to assess and respond to anger in the clinical setting. Communication could be improved through empathic statements that convey realistic optimism when appropriate, a commitment to the patient–provider relationship and a willingness to explore and address patient needs.
Although clinically relevant levels of anger are witnessed in up to 20% of patients with cancer, 1,2 the emotion is understudied compared to depression and anxiety, and men with prostate cancer have reported receiving inadequate help for their anger. 3 -5 Anger is a natural response to situations that are threatening, uncontrollable, or perceived to be unfair, 6 but individuals also differ in their proneness to anger. While anger may be viewed as an irrational response and patients who express anger may be labeled as difficult, anger also serves important functions for empowering individuals to confront loss and adversity. However, when poorly regulated, anger and other forms of distress present significant barriers to medical decision-making because distressed patients may adopt a negative problem orientation toward their illness that leaves them doubtful, rejecting or dismissive of treatment recommendations. 7 -13 Moreover, patient’s anger may be perceived as a threatening emotion to many providers and may disrupt communication, especially when discussing difficult topics such as prognosis and goals of care. 14,15 Given calls for distress screening in oncology 16 and for earlier provision of palliative care in populations with cancer, 17 palliative care clinicians will spend increasing time with anger-prone patients who previously would not have received palliative care.
Kübler-Ross et al 18 was among the first palliative care leaders to note the primacy of anger in response to terminal illness. Following a sense of shock and denial, Kübler-Ross et al noted that many patients experienced intense anger. Anger may shape the patients’ thought process and lead to misunderstandings and hostile communications. Angry patients may blame providers and adopt beliefs that providers are incompetent or are withholding information. In order to effectively engage angry patients in goals of care discussions, providers must consider how anger shapes the patient’s understanding of their prognosis. 19 Although many individuals become angry in response to specific situational stressors such as cancer, individuals also differ in their overall tendency to become angry across situations. 20 Momentary anger is referred to as state anger, and the overall tendency to become angry is referred to as trait anger or anger proneness. Kübler-Ross focused (implicitly) on a type of self-limiting state anger that resolves with acceptance and support. Jackson and colleagues 21 have noted that a degree of momentary anger may be indicative that prognostic information is being integrated and processed by the patient. To the best of our knowledge, trait anger has been rarely discussed in the palliative care literature. Trait anger may be chronically problematic if patients repeatedly respond with anger and hostility across the duration of their cancer trajectory. If anger and its determinants are not well understood, providers may inadvertently frustrate and invalidate patient experiences. 18
The Five Factor Model of personality defines anger regulation style as the combination of personality traits of neuroticism, the tendency to experience negative emotional states, disagreeableness, and the tendency to be uncooperative, distrusting, and cold 22 (see Figure 1). Individuals demonstrate relatively stable styles of anger regulation. 22 -24 Highly disagreeable individuals tend to be dissatisfied with life events in general, 25 and in the context of patient–provider communication, patient disagreeableness has been linked to reduced trust and satisfaction with providers. 26 Compared to individuals with other anger regulation styles such as easy going (agreeable and low neuroticism), timid (agreeable and neurotic), and cold (disagreeable and low neuroticism), anger-prone individuals (disagreeable and neurotic) are more likely to exhibit aggressive outbursts, hostile cognitions, biased perception of threat, cynical distrust of others, 27 -29 and, we hypothesize, relatively pessimistic view of their cancer prognosis. This is an important hypothesis to test because anger-prone patients who lack trust in their medical providers may be less likely to receive adequate information about their disease and prognosis. Consequently, they may experience poorer outcomes. 30 -34
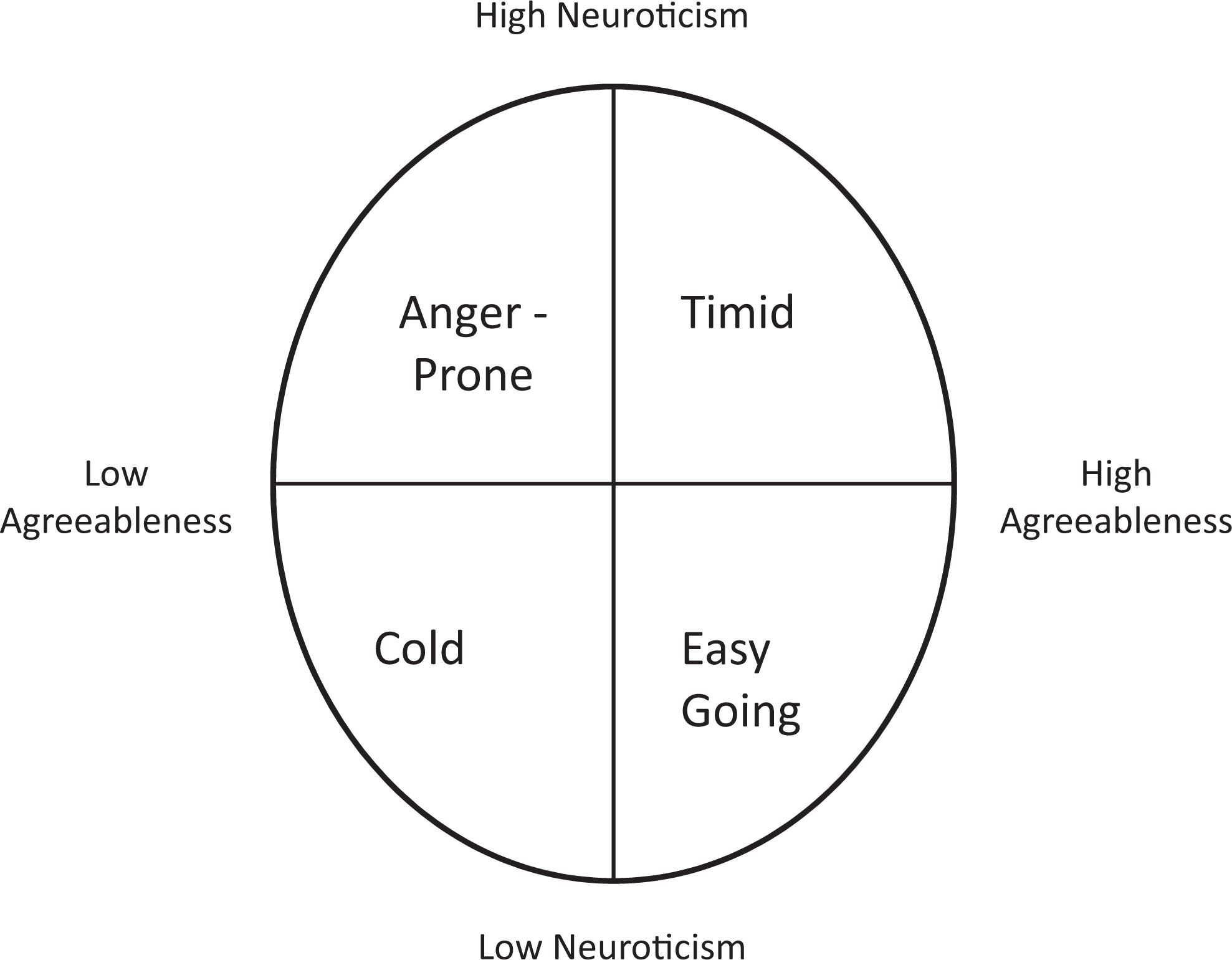
Five Factor Model anger regulation-style circumplex.
The current study investigated the associations between anger proneness and optimistic/pessimistic beliefs about prognosis in 212 men diagnosed with prostate cancer. We hypothesized that men who are anger prone (disagreeable and neurotic) would underestimate their projected 5-year survival relative to their estimate of their doctor’s assessment of prognosis.
Method
Participants and Procedure
The study was reviewed and approved by the University of Rochester Institutional Review Board. Participants (N = 212 men with prostate cancer) were recruited via the NIH ResearchMatch (researchmatch.org) recruitment tool from July 2011 to April 2012. Participants were solicited through e-mail to complete a cross-sectional online survey on medical decision-making at the James P. Wilmot Cancer Institute of University of Rochester. The ResearchMatch tool provides access to a database of approximately 85 000 individuals who may be interested in participating in research. Volunteers register to the database and provide background information to determine their interest and eligibility for various research studies. Registered researchers can then access the database to contact participants. Potential participants could also reach the study through links posted on health Web sites, listservs, and various search engines. The research Web site included an online consent form and provided contact information for the study personnel. Participants were eligible to register for a US$100 raffle to compensate them for their participation in the study. If participants were not interested in the study, they would not respond to the e-mail or access the Web site, and so refusal rates could not be determined. Data were screened for invalid responses including inappropriate responses to validity check items, rapid response rates, and repeat responses.
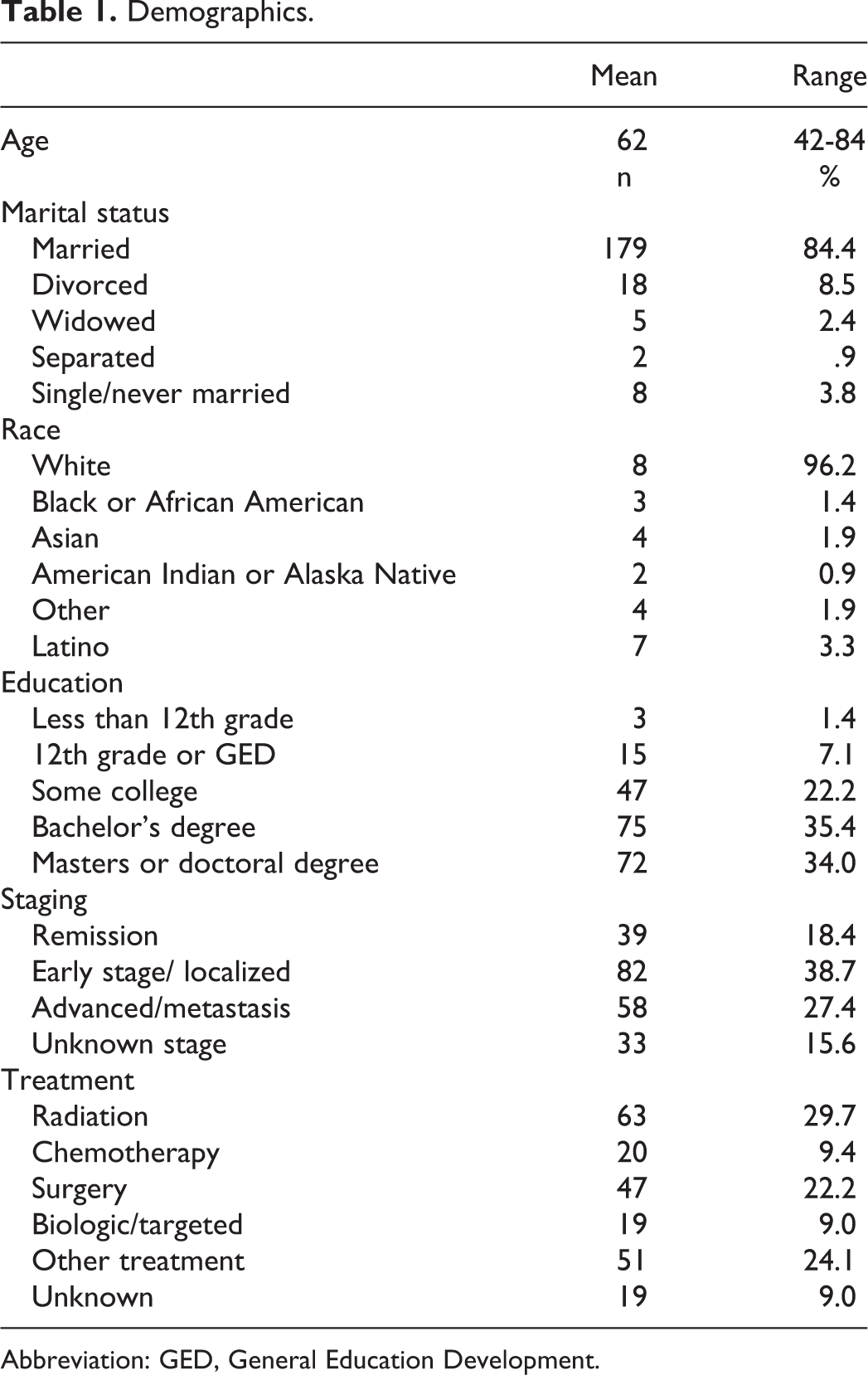
Table 1 presents demographic information of study participants. On average, participants were 62 years old; most (66.5%) were between 54 and 70 years of age. Age ranged from 42 to 84 years old. The majority (84.4%) of participants were married and identified as caucasian (96.2%; an additional 1.9% identified as Asian, 1.4% identified as black or African American, 0.9% identified as Native American/Native Alaskan, and 1.9% identified as other). Few (3.3%) identified as Latino. Many reported having a bachelor’s degree (69.3%) and private insurance (64.6%) or Medicare (31.1%). The median time since prostate cancer diagnosis was 1.5 years (interquartile range = 0.7-3.5 years), with 42.0% having been diagnosed within the past year and 18.4% having been diagnosed at least 5 years ago. With regard to staging, 38.7% reported localized disease, 27.4% reported metastatic disease, 18.4% reported disease in remission, and 15.6% reported unknown staging. Participants received a range of treatments for prostate cancer including radiation (29.7%), surgery (22.2%), chemotherapy (9.4%), biologic/targeted therapies (9.0%), other therapies (24.1%), and no treatment (22.2%). Due to the online nature of the study, medical records were not available to confirm diagnoses or treatments. Prior work suggests that self-reported medical data are reliable and valid among men with prostate cancer. 35,36
Demographics.
Abbreviation: GED, General Education Development.
Measures
Demographic background
Participants reported demographics described earlier.
Personality traits
To assess neuroticism and agreeableness, participants completed the Mini International Personality Item Pool (IPIP), a 20-item scale validated as a Five Factor Model personality trait measure. 37 The Mini-IPIP was adapted from the 50-item IPIP, 38 which has been used to study neuroticism and agreeableness in relation to anger, 23,24 perceived discrepancies in social situations, 39 and health-related behavior. 40 Participants answered 4 questions each for neuroticism and agreeableness. Items on the Mini-IPIP offered participants a Likert-type scale from which to select 1 to 5, described as “very inaccurate,” “moderately inaccurate,” “neutral,” “moderately accurate,” and “very accurate,” respectively. The sum of each 4-item subscale represented neuroticism and agreeableness total scores in analyses. Internal consistency was good for the neuroticism (α = .77) and agreeableness (α = .70) scales. For sensitivity analyses, anger management styles (see Figure 1) were operationalized using median splits such that Easy Going was defined as a neuroticism score below the median and agreeableness above the median. Timid was defined as both scores above the median. Cold was defined as both scores below the median. Anger prone was defined as a neuroticism score above the median and an agreeableness score below the median.
Prognostic discrepancy
Prognostic discrepancy was assessed by asking participants the following questions, “Patients in this study have many different types of cancer with varying chances for a cure. What do you believe are the chances that you will live for five years or more?” and “Sometimes people have different views. If you had to guess, what do you believe your doctor thinks the chances are you will live for five years or more?” Participants responded to both questions using the following scale (0 = 0%, 1 = 1%-25%, 2 = 26%-74%, 3 = 75%-99%, 4 = 100%). 41 This method of assessing prognostic discrepancy has been used previously in studies assessing patient–physician communication 41 and patient perceptions of prognosis. 42 The order of 2 questions was counterbalanced. Discrepancies were identified by subtracting the patient belief score from the provider belief score such that lower values indicated more pessimistic beliefs on part of the patients.
Analysis
All analyses were conducted in SPSS version 19. 43 Descriptive statistics and bivariate associations were tested to assess for potential confounders such as age, disease staging, and time since diagnosis. The primary study hypothesis was tested following guidelines of Aiken and West 44 and within the process utility for SPSS. 45 Prior to using the process utility, neuroticism and agreeableness were standardized. As such the unstandardized regression coefficients reflect differences in prognostic discrepancy based on a 1 standard deviation change in the dependent variable. Within this framework, a significant interaction term is considered evidence of moderation. Interactions are then probed by assessing associations between the independent variable (ie, neuroticism) and the dependent variable (ie, prognostic discrepancy), with the moderator (ie, agreeableness) at both 1 standard deviation above and 1 standard deviation below the mean. An adjusted analysis was conducted to evaluate the interaction after accounting for disease staging, age, marital status, and education that theoretically could influence patient expectations and understanding of their illness. Finally, sensitivity analyses were conducted to determine whether a categorical approach using median splits (see heading 2.2.2) could identify how anger-prone participants differ from participants with other anger regulation styles. Similar approaches to operationalizing personality styles have been used previously. 46,47
Results
The majority of patients expected a 75% or greater chance of living 5 years and perceived that their doctors had similar expectations (see Table 2). Nonetheless, there were significant discrepancies. Specifically, 22 (10.4%) participants viewed themselves as more pessimistic than their doctors about their prognosis and 29 (13.7%) viewed themselves as more optimistic. A 1-way analysis of variance with post hoc Tukey Tests indicated that participants with advanced disease were more optimistic than they believed their doctors to be when compared to participants with early-stage disease (P = .023) and unknown stage (P = .046). Bivariate correlations indicated that when considered separately, neuroticism and agreeableness were not related to pessimistic/optimistic perceptions of prognosis, r = .05, P = .619, r = .04, P = .725, respectively. A small but significant correlation was observed between neuroticism and agreeableness (r = −.21, P = .002).
Patient Demographics and Reported Expectations of Prognosis.

Moderation analyses were used to test the hypothesis that neuroticism and agreeableness interact to predict discrepancies between patient and doctor belief of prognosis. Results indicated a significant interaction (B = .080, standard error [SE] = .039, P = .041, R2 Change = .021) such that the association between neuroticism and prognostic discrepancy was significant among individuals low (−1 SD) in agreeableness (B = −.135, SE = .059, P = .024) but not among individuals with high (+1 SD) levels of agreeableness (B = .026, SE = .028, P = .659). As can be seen in Figure 2, anger-prone individuals (ie, those reporting high levels of neuroticism and low levels of agreeableness) were more likely to view themselves as more pessimistic than their doctor. After adjusting for advanced disease, age, marital status, and education, the interaction term remained significant (B = .083, SE = .038, P = .032; See Table 3). Participants with advanced disease status were more optimistic than they believed their doctors to be (B = .30, SE = .09, P = .003). Following the examples of Fang and colleagues 46 and Weiss and colleagues, 47 we investigated the predictive utility of a categorical classification by identifying anger-prone individuals with neuroticism scores above the median and agreeableness scores below the median.
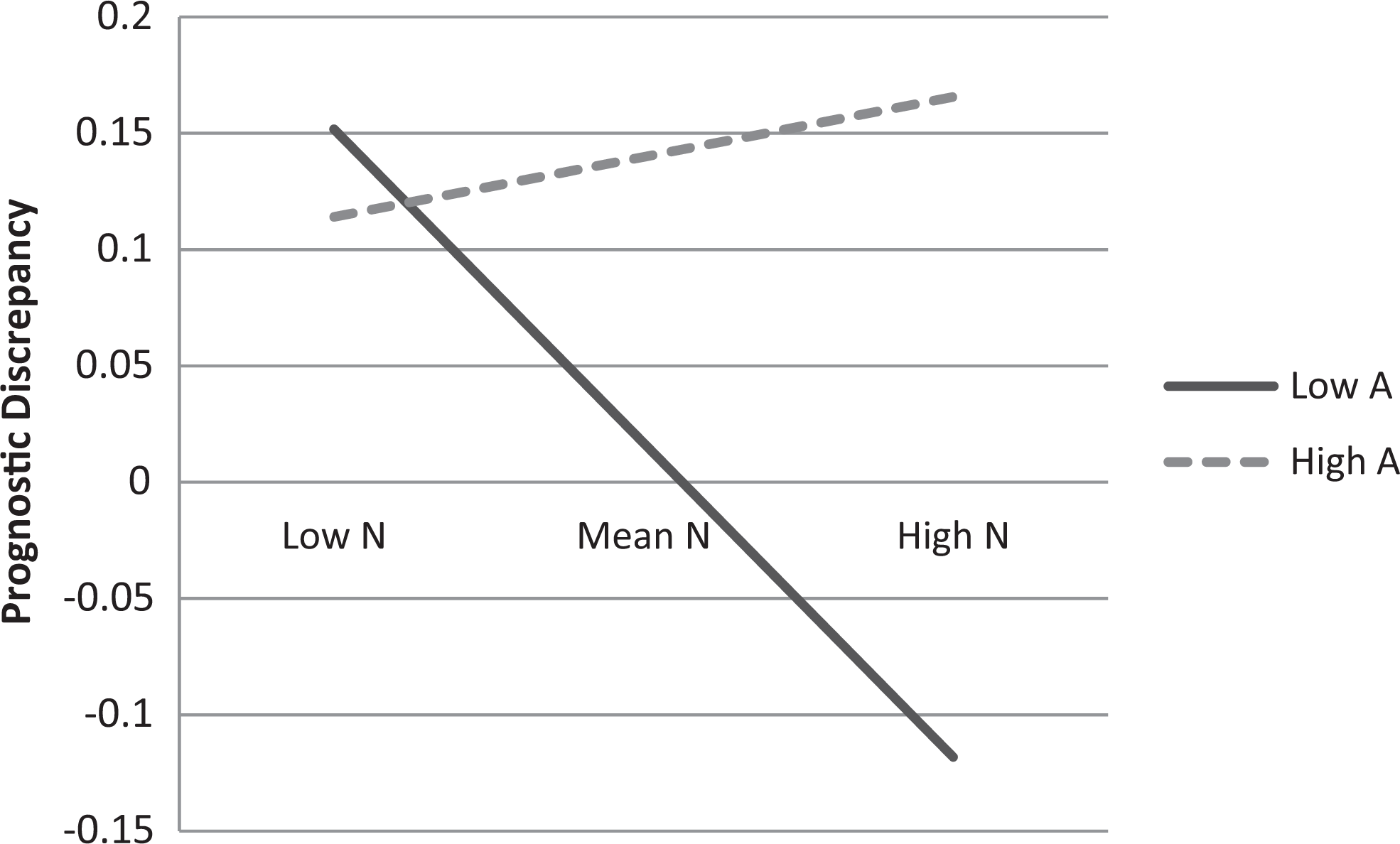
Interaction plot of neuroticism and agreeableness predicting prognostic discrepancies. N = Neuroticism, A = Agreeableness, Low = 1 standard deviation below the mean, High = 1 standard deviation above the mean. Prognostic discrepancy values are depicted.
Neuroticism and Agreeable Interact to Predict Prognostic Discrepancy.
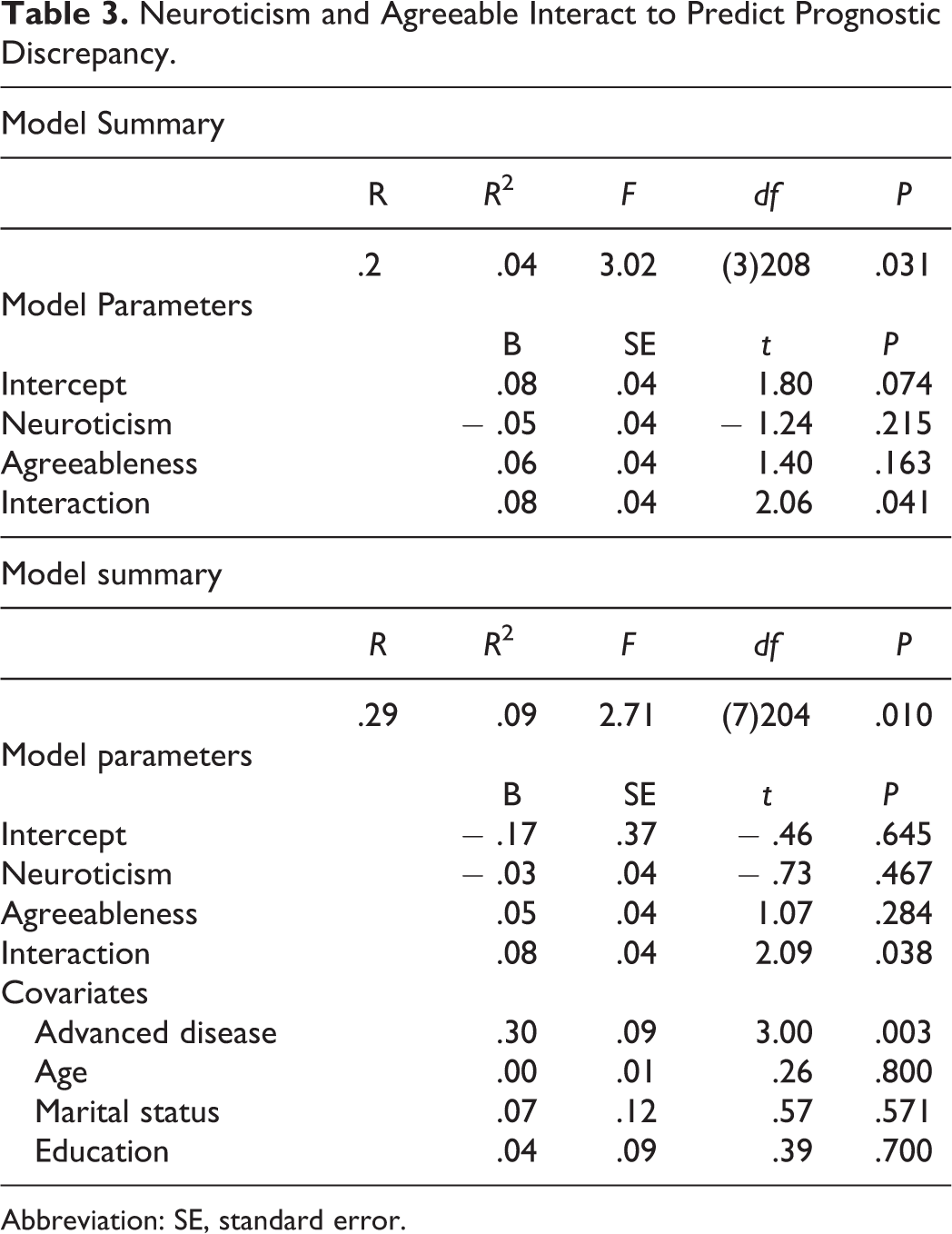
Abbreviation: SE, standard error.
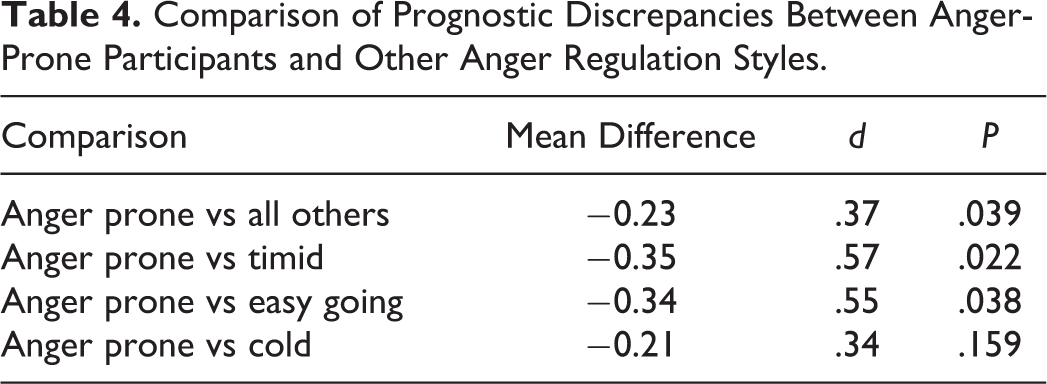
Table 4 presents mean differences and effect sizes for comparisons between anger-prone and other participants. The 43 (20.2%) participants with the anger-prone style reported more pessimistic beliefs regarding their prognosis (Mean = −.12, SD = .59) compared to the rest of the sample (Mean = .11, SD = .64), t(210) = −2.08, P = .039, d = .37). In a comparison of all anger regulation styles, the 43 anger-prone men reported more pessimistic beliefs regarding their prognosis compared to the 31 timid men (Mean = .23, SD = .64), t(72) = −2.34, P = .022, d = .57, and 37 easy going men, (Mean =.22, SD = .82), t(76) = −2.11, P = .038, d = .55, but not the 32 cold men (M = .09, SD = .69), t(73) = −1.41, P = .159, d = .34. A 1-sample t test comparing 3 groups (timid, easy going, and cold) showed that these participants were significantly inclined toward more optimistic beliefs relative to a discrepancy of zero, t(99) = 2.47, P = .015. This suggests that men with other anger management styles may lean more toward an optimistic outlook of their prognosis.
Comparison of Prognostic Discrepancies Between Anger-Prone Participants and Other Anger Regulation Styles.
Discussion
Findings suggest the importance of anger in shaping patient understanding of their illness. In this sample, 24.1% of participants stated that they and their doctor had discrepant views toward 5-year prognosis. Ten percent of the participants perceived their prognosis more pessimistically than their doctor’s assessment of prognosis. As hypothesized, men with an anger-prone style have a greater tendency toward more pessimistic views of 5-year prognosis compared to other men with prostate cancer, including those with timid traits who are also characterized by high neuroticism. These analyses are clinically significant to the extent that underweighted/underestimated prognosis has implications for treatment responsiveness and quality of life. Over the short term, patient may base their decisions regarding testing and treatments on their perception that their prognosis is worse than that estimated by their physician and may pursue more invasive testing and intervention. 9 Over the long term, pessimistic beliefs about the curability of cancers have been linked to higher mortality over 15 years follow-up. 48
Results of this study extend prior work on the association of neuroticism with the impact of cancer-related distress. Individuals with elevated neuroticism are more prone to depression and to general distress, including worry, anxiety, and pessimistic attitudes, 49,50 and this could manifest as higher levels of worry regarding their prostate cancer care. 51,52 While agreeable traits (eg., sympathetic, kind, cooperative) may enable distress-prone men to overcome worries and trust their provider’s assessment of prognosis, disagreeable traits (eg., cynical, selfish, quarrelsome) may undermine trust, compromise communication, and lead to overly pessimistic views of cancer prognosis. These findings also extend prior work on agreeableness and patient reports of satisfaction with care and physician competence. 26,53,54 While agreeable patients tend to report greater trust and satisfaction with their providers overall, disagreeable patients may require a greater emphasis on support and warmth from their providers to establish trust. 26 Patients and their spouses may be shocked by a diagnosis of prostate cancer, 55 and, therefore, it is possible that anger-prone patients may be too overwhelmed with the cognitive, emotional, and somatic experience of anger to effectively listen to their providers during stressful conversations.
Providers should explore patient uncertainties with empathy, assertive communication, and verbalize their willingness to address concerns and frustrations. 33,56 Providers can also assess for the presence of anger and a negative problem orientation related to cancer prognosis in the context of distress screening or goals of care planning. 7 Misunderstandings may be mitigated if providers ask patients about information needs and personal preferences, provide medical information, and assess patient understanding of the information. 41
The current study suggests that anger proneness is important in men with prostate cancer and may have implications for discussions of prognosis and care planning. The distinction between momentary anger and anger proneness is important to highlight in the context of how providers can optimally respond to anger-prone patients in treatment-related discussions. Given the multifactorial origins of anger in populations with cancer, it may be most useful to providers to first help them identify which kind of anger expression their patients are displaying and adjust their response style accordingly. State anger refers to anger expression from an acute, anger-provoking stressor and typically resolves with the removal of the stressor. Communication coaching may be useful for helping providers understand the origins and adaptive expression of anger and to elicit and empathically respond to patient anger. 15,56
Responding to anger proneness, or trait anger, often calls for more advanced skills as these patients are consistently hostile. For example, although many patients may experience some justifiable anger in response to a provider error, anger-prone patients may display levels and intensities of emotion that are disproportionate to the situation and significantly greater than other patients. Anger-prone patients may displace their anger onto people who are not responsible for errors. Their anger may be unrelated to the actions of the provider but instead related to aspects of the diagnosis or treatment. It is not uncommon for anger to serve adaptive functions, such as restoring a man’s sense of perceived control in the midst of uncertainty. 19
Much of the empirical literature on intervening with anger-prone individuals has explored anger management programming. The persistent anger of patients referred to these programs presents a challenge even to seasoned clinicians. 57 Although more research is needed, some lessons from anger management may be applicable to palliative care clinicians. Providers should be cognizant of their own attributions and emotions when working with anger-prone patients. 15 Here the goal is to stay present with the patient without avoiding the experience of emotional distress elicited by the patient. Providers may learn to be willing to hear out the angry patient and not take the anger personally, as it occurs across contexts. Providers may also find work more rewarding if they cultivate compassion by considering the adverse developmental experiences that may have shaped chronic anger and the suffering it maintains. Kübler-Ross et al 18 shared the anecdote of a nurse who wished to die as the same angry rebel as she had lived and argued that the patient should be accepted and permitted to die according to her wishes. These strategies may help the provider accept the patient holistically and could limit escalation of conflict.
Behaviorally, providers should look for ways to strengthen the working alliance between themselves and their patients. 57 This includes developing a mutual agreement on treatment goals, which may be an area of strength for palliative care clinicians who routinely facilitate goals of care discussions. Finally, when anger and other difficult emotions are intractable, palliative care clinicians may find that a team-based approach to consultation may help them share the emotional load and maintain effective patient boundaries. 58 By exploring patient anger, providers can identify underlying concerns, address them with compassion, and share information related to the disease and its treatment. Even still, many anger-prone patients will be immediately dismissive of empathic remarks. The stressful nature of palliative care may trigger emotional reactions among clinicians. 59,60 Patient’s expression of anger is commonly an emotionally triggering event for clinicians, and clinicians are encouraged to seek consultation and practice self-care as they routinely face these challenging encounters. 61
Results of this study should be qualified in the context of its strengths and limitations. The study included a large sample of men with a history of prostate cancer. The evaluations are well validated and have been used previously in research. The study is limited by its cross-sectional nature, and associations should not be interpreted as causal. Data are patient reported, and discrepancies in prognosis are based on the perceptions of participants. Patient data including staging should be corroborated with medical chart reviews in the future. In addition, participants may have had multiple providers, and follow-up studies should assess if discrepancies are more likely to occur with specific providers (eg. oncologists, urologists, primary care physicians). Although our findings suggest that anger-prone individuals believe they are more pessimistic than their doctors, another interpretation is that patients who are timid or easy going tend to be relatively optimistic. Undue optimism may be cause for clinical concern if it reduces engagement in health-promoting behaviors 62 or contributes to overly positive predictions of treatment response. 63 Another important limitation is the lack of racial diversity in the current sample. It is possible that the magnitude of prognostic discrepancies may differ in marginalized samples that face barriers to satisfactory health care. For example, the sociohistorically engendered mistrust of the health-care system among African Americans could contribute to greater discrepancies, and replication of these findings should be pursued in more diverse samples. 64 More research is needed to determine how these discrepancies may occur in with other common malignancies such as lung cancer and breast cancer.
Conclusion
In conclusion, this study demonstrated a significant association between anger regulation style and pessimistic beliefs about prognosis among men with prostate cancer. Previous research has linked prognostic pessimism to poorer long-term outcomes for men with prostate cancer. Palliative care professionals and other providers should be attentive to patient expressions of anger and tailor their communication styles to help patients resolve their unmet needs.
Footnotes
Authors’ Note
We are grateful to Mark Grichanik, M.A. for his feedback on Big-5 personality traits.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Rochester Medical Center Department of Psychiatry Leonard F. Salzman Research Award, T32MH018911 from the National Institute of Mental Health, and U54GM104940 from the National Institute of General Medical Sciences. Dr. Gerhart and Dr. O’Mahony receive support from the Prince Charitable Trusts, and the Coleman Foundation.