
Abstract
Background:
Advance care planning (ACP) is an instrumental mechanism aimed at preserving patient autonomy. Numerous interventions have been proposed to facilitate the implementation of ACP; however, rates of completed advance directives (ADs) are universally low. Patient electronic portal messaging is a newer tool in patient–provider communication which has not been studied as a method to promote ACP. In this study, we hypothesized that the use of ACP-specific patient electronic messages would increase rates of AD completion in patients aged 65 years and older in an academic primary care practice.
Methods:
All primary care patients, aged 65+, who had previously enrolled in a patient electronic messaging system, within an academic primary care practice, were included for randomization. Two hundred patients were randomized to receive an electronic message. The primary outcome was the proportion of patients in each group who completed an AD, 3 months after intervention. Secondary outcomes included clinical utility of the completed ADs and proportion of patients who viewed their electronic messages.
Results:
The intervention group completed an AD 5.5% of the time when compared to 2% in the control group (odds ratio 3.2 [1.6-6.3]). Up to 74.5% of patients opened their electronic messages.
Conclusion:
Among primary care patients aged 65 years and older, use of AD-specific electronic messaging statistically significantly increased the rate of AD completion, but the absolute number of completed AD remained relatively low. These data suggest that this valuable communication tool holds opportunities for further improvement. Older, frailer adults were more likely to complete an AD, and prompted directives were more likely to include a written expression of the individual’s health-care values and preference.
Background
Advance care planning (ACP) is a dynamic, iterative process for patients to communicate their preferences for medical care should they ever lose the capacity to express their wishes or the ability to make medical decisions. 1 Although the efficacy of ACP has been debated in the past, numerous studies have shown that the process promotes patient autonomy and enhances communication between providers, patients, and their families. 2 –4 Now, over 20 years since the Patient Self-Determination Act, ACP is emerging as a reportable quality metric in some areas and has been endorsed by the National Quality Forum. 5 Documentation of ACP within the electronic health record (EHR) can take many forms including the designation of code status, health-care proxy, discussions between a patient and a provider, or most commonly via an advance directive (AD).
Despite the aforementioned drivers of ACP, AD completion rates remain universally low, at approximately 30% among patients aged 18 years and older, in the United States. 6 Numerous barriers to successful completion of an AD have been identified, and wide-ranging solutions have been proposed including physician training sessions, computer-generated reminders for providers, appointments targeted toward ACP, interactive patient education seminars, and prolongation of the health maintenance examination visit. 4,7,8 Many of these interventions have been temporarily successful in improving AD completion but can be difficult to sustain long term due to financial and time constraints. 9 –11 Few studies have taken into account the changing technological landscape within medicine, specifically, electronic patient messaging, as a means of reaching a wider patient population in a cost-effective manner. 12
Secure patient electronic messaging (PEM) is rapidly being adopted by many medical institutions. Patient electronic messaging is typically a feature of the institution’s EHR, which allows patients to interface with their medical record, check test results, and securely send and receive electronic messages from care providers. The Markle Survey on Health in a Networked Life identified that 9% of patients in the United States were enrolled in a PEM system in 2010. 13 This survey was published only 1 year after the initiation of the Health Information Technology for Economic and Clinical Health Act in 2009, which has since increased EHR adoption by as much as 7% and likely spurred increases in PEM in the process. 14 Currently, multiple medical centers throughout the United States actively employ patient portals, including the Veterans Administration, Kaiser Permanente, Cleveland Clinic, MD Anderson Cancer Center, Vanderbilt, Northwestern Medicine, and Mayo Clinic. 15 –18
Since the emergence of PEM, multiple groups have studied its effect on various patient populations. In multiple studies, patients older than 65+ years of age constituted approximately 15% to 25% of active PEM users. 19,20 There are several recent studies and systematic reviews that have shown overall positive results with respect to patient satisfaction, improved patient–provider communication, and better self-management of chronic conditions through the use of a messaging system. 19,21 –23 Given the widespread use of portal technology in chronic disease management, experts in this field have called for trials examining their utility in promotion of ACP. 12
The primary aim of this study was to measure the impact of a personalized ACP electronic message on AD completion in the primary care setting. We hypothesized that a nonintrusive motivational electronic message linked to appropriate resources would improve AD completion rates among senior adults.
Methods
Setting
Mayo Clinic’s Division of Primary Care Internal Medicine (PCIM) Clinic in Rochester, Minnesota, located in Olmsted County, provides primary care to over 35 000 patients. At the time of this intervention, the division was composed of 48 internists, 96 resident physicians, and 29 advance practice providers. This division provides primary care to the local community, to Mayo Clinic employees, and their dependents. Most patient visits occur on the downtown campus. Olmsted County has a population of over 150 000 people, with 13.6% of the population comprised of those aged 65 and older. 5
The Mayo Clinic Patient Online Services system is a secure EHR and PEM system that has been offered without cost to all patients since 2009. Registration is patient initiated and not mandatory in order to receive care at the institution. Registration allows patients secure access to physician notes, laboratory test results, imaging studies, and appointment details. In addition, there is a messaging system that allows patients and their providers to communicate electronically. As of 2015, there are over 700 000 patients enrolled, with an adoption rate of approximately 45%.
Study Design
We conducted a randomized controlled intervention within the Division of Primary Care Internal Medicine. The study was conducted from May 2015 through July 2015.
Participants
Patients empaneled to a PCIM provider were evaluated for inclusion. Patients were included if they were aged 65 or older, did not have an AD on file within their EHR, and had access to the Mayo Clinic Patient Online Services system.
Outcomes
The primary outcome was the completion and return of an advance care plan within 3 months of receiving a personalized message prompt. The secondary outcomes included clinical utility of the completed AD based on (1) presence or absence of a health-care proxy, (2) designation of code status, and (3) personal description of health-care wishes and values.
The AMALGA Hospital Information System IT platform was used to obtain baseline patient data for all patients participating in the study. Baseline data included demographic information, Johns Hopkins Adjusted Clinical Group medical complexity tier, and Elder Risk Assessment (ERA) 24 score. The Johns Hopkins Adjusted Clinical Group (ACG) model is a proprietary model that characterizes patient morbidity. Higher medical tier is associated with higher morbidity. 24 The ERA index is a risk model that has been validated to identify elderly patients at risk of nursing home placement and mortality within 2 years. 25 Patients are assigned points based on numerous factors, including age, race, and presence of specific chronic medical conditions. High ERA scores are associated with high risk of mortality and morbidity.
Sample Size
It was determined that in order to detect a 10% difference with 90% power, assuming a 5% AD completion rate in the usual care group, the study would require 200 patients in each arm. Thus, 200 patients were individually, electronically randomized to the intervention arm, and the remainder of the population comprised the control arm, which received usual care.
Intervention
Patients randomized to the intervention arm received a personalized PEM explaining the ACP process and encouraging them to complete an AD. The electronic message also included a link to an ACP workbook that guided the individual and their loved ones through each step of the ACP process. This workbook included a Minnesota-specific AD form with instructions on how to return the completed document to the patient’s primary care provider. Eight weeks after the initial message was sent out, a reminder message was delivered to those individuals who had not yet returned an advance care plan. Final outcomes data were collected at 12 weeks. This quality improvement intervention was reviewed and deemed exempt by the Mayo Clinic institutional review board.
Statistical Analysis
Data were summarized using mean ± standard deviation for continuous variables and frequency counts and percentages for categorical variables. The percentage of patients who completed an AD was compared between study groups (electronic message intervention vs usual care) using the χ 2 test. To assess other characteristics potentially associated with the completion of an AD, a series of logistic regression analyses were performed. Separate analyses were performed for each of the patient characteristics listed in Table 1. For these analyses, completion of AD was the dependent variable, and the explanatory variables included the characteristic of interest and study group (electronic message vs control). The 2-way interaction between the given characteristic and study group was included in an initial analysis to assess whether the effect of electronic message was dependent on the given characteristic. In addition, to assess each characteristic individually, 2 preplanned multivariable analyses were performed. Age, sex, and study group as well as a multivariable model included the Johns Hopkins ACG medical tier, and the other model included ERA score.
Baseline Characteristics.
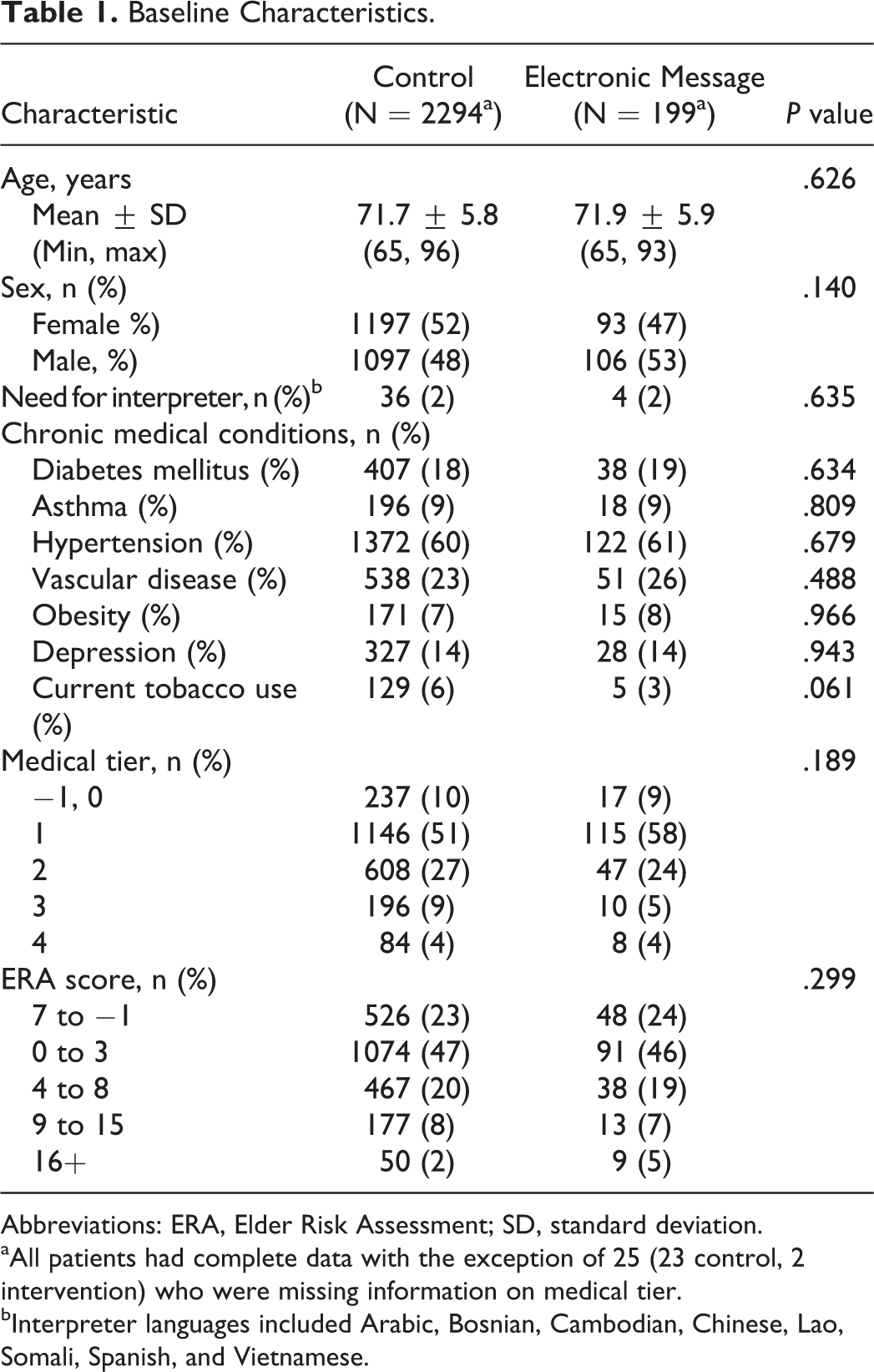
Abbreviations: ERA, Elder Risk Assessment; SD, standard deviation.
aAll patients had complete data with the exception of 25 (23 control, 2 intervention) who were missing information on medical tier.
bInterpreter languages included Arabic, Bosnian, Cambodian, Chinese, Lao, Somali, Spanish, and Vietnamese.
In analyses restricted to patients in the electronic message group, exploratory analyses were performed using the 2-sample t test or χ
2
test to compare characteristics between those who opened the electronic message versus not. In all cases, 2-tailed P values of ≤.05 were considered statistically significant. Data related to this study may be obtained by e-mailing the corresponding author at
Results
Baseline Characteristics
A total of 2526 patients within the Division of PCIM, aged 65 and older, with access to the secure PEM system and without an AD on file, were included for randomization. Two hundred patients were individually randomized to the intervention group. The remaining 2326 patients comprised the control group. Of these, 32 patients left the practice during the time of our study and were not included in the final statistical analysis. Clinical characteristics and demographics were balanced between the group randomized to receive the motivational message and those in the control group (Table 1.)
Primary Outcome: AD Completion and Return
Among the intervention group, 11 (5.5%) completed and returned an AD during the study period compared to 46 (2%) in the usual care group (odds ratio [OR] 3.2, confidence interval = [1.6-6.3]). Additional factors associated with completion of an AD included higher medical complexity (P = .017) and older age (OR per 5 year age increase 1.5, P < .001)
Secondary Outcomes
Of the 200 patients randomized to receive the intervention, 149 (74.5%) opened their electronic message.
Among the returned ADs, those directives completed by individuals receiving the personalized message and ACP workbook were more likely to include a personal expression of their health values (P < .02; Table 2)
Comparison of Advance Directive Content.
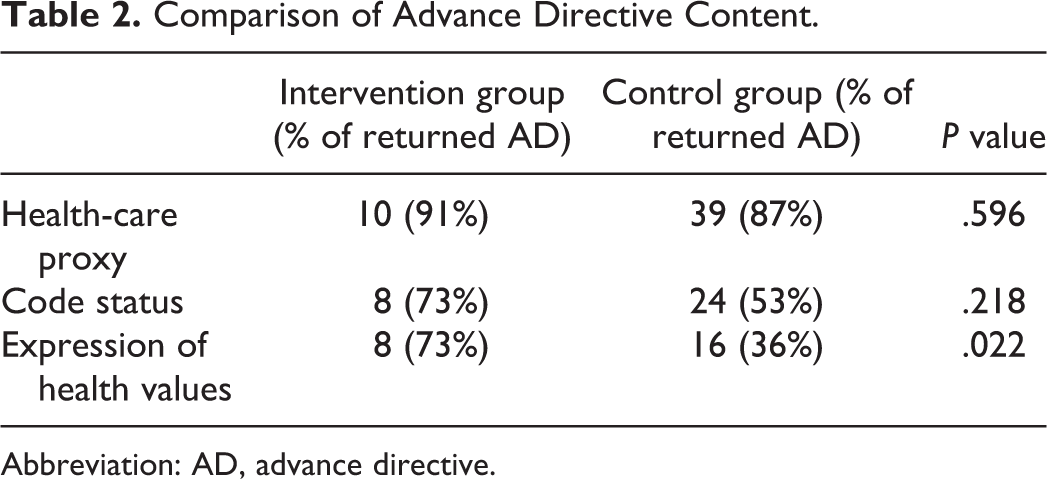
Abbreviation: AD, advance directive.
Discussion
This study revealed that individuals receiving personalized, electronic motivational prompts and electronic resources were statistically significantly more likely to complete and return an AD document when compared to usual care. Additionally, the content of the ADs that were completed as a result of this minimally intrusive intervention was both comprehensive and clinically useful. Although the absolute number of completed AD remained low (11 of 199), the trend toward a positive association between PEM and AD completion is important to recognize. To the best of our knowledge, this project reports the only randomized trial utilizing electronic messaging as a motivational tool for ACP. This demonstrates both the feasibility and the utility of electronic messaging systems in facilitating ACP in some primary care patients.
Motivational portal messaging has established utility as a low touch, inexpensive intervention that has increased patients’ willingness to participate in various aspects of health care from diabetes management to medication reconciliation. 26,27 Utilization of health messaging allows patients to consider important health data, medical recommendations, and view patient education during their own time in the privacy of their own home. This modality also allows patients to share information with loved ones and decision makers who may not be able to attend office visits.
Other authors have successfully utilized nonelectronic messaging to prompt ACP. These interventions include ACP counseling offered via face-to-face visits with primary care providers or telephonic-based visits. 28 –30 Our group demonstrated that mailing ACP materials prior to a health maintenance visit also increased rates of AD completion. 31 Several state-wide initiatives to improve ACP utilizing trained volunteers have also proven feasible. 32,33 However, each of these ACP enhancement modalities requires substantial time and resource utilization for both the institution and the patient and requires ACP to occur during a time frame that is convenient for the health-care institution but not necessarily convenient or acceptable for the patient. Few studies have employed electronic tools to aid in ACP. One study investigated the use of electronic reminders to physicians, urging providers to discuss ACP with their patients. 34 Other authors have studied electronic decision aids to facilitate ACP conversations. 35 However, these modalities are dependent on an office visit which are challenging to sustain in this era of increasing nonvisit care and limited face-to-face visits. Additionally, existing limitations in primary care access for older adults minimizes the feasibility of dedicated ACP visits. 13
We view PEM as a feasible and emerging vehicle for delivering important ACP tools and a means of normalizing discussions about this sensitive topic. This modality also allows providers to tailor PEM to target specific, at-risk populations within their practices. For example, materials may be translated to reach non–English-speaking patients who historically have lower rates of ACP. 36 Additionally, inclusion of video technology may allow providers to better reach lower rates of health-care literacy. 37 Messages may also be sent at multiple time points, allowing for evolution of material as a patient’s understanding of ACP grows. This may be crucial to success because the process of ACP has been conceptually likened to the behavior change model. 1 Thus, use of PEM would allow for facile communication of the right information at the right time.
For health-care institutions with electronic messaging capabilities already in place, this intervention is both cost efficient and sustainable once automated. These results are generalizable regardless of the PEM system in place. A relatively simple, text-based message was utilized in this study, which can be performed by most messaging platforms.
This study is not without limitations. First, the authors recognize that ACP needs to vary at different points in an individual’s life. At times, planning may require intensive face-to-face communication between the individual, his or her loved ones, and their health-care team. While our intervention does not replace this valuable longitudinal communication between the patient and their health-care team, it does represent a starting point for ACP and normalizes dialogue regarding the topic. Second, patients targeted in this study must have access to a computer and have registered for electronic messaging. This confers selection bias for individuals with greater socioeconomic security and higher degrees of health literacy. This intervention also poses a problem with those who are not literate in English, although translation of culturally sensitive ACP materials is feasible. Third, the possibility exists that patients could have been exposed to other measures designed to increase ACP awareness which were in effect at the same time as the study; however, our randomization process minimized the impact of confounding factors.
In this era of burgeoning use of health information technology, PEM represents an inexpensive and feasible adjunct to many of the measures currently in place throughout health-care institutions. We have demonstrated that motivational electronic messaging allows patients to participate in ACP and complete an advance care directive on their own terms independent of office visits. Further studies of electronic ACP dialogue are needed to determine patient acceptability and satisfaction with the use of this technology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.