
Abstract
The nation faces a persistent issue of delayed access to hospice care. Even though hospice enrollment is considered to be one of the most difficult medical decisions, physician clinics and hospitals lack tools for helping patients/families faced with making decisions about enrollment. Health-care literature lacks discussion of development of decision-making aids in the context of hospice decisions for minority ethnic groups, even though those groups have decisional needs that may differ from those of non-Hispanic whites. To fill the gap, we developed a video of a Latino hospice patient with footages showing how the patient was being taken care of by her family with support from a hospice disciplinary team. A primary objective of this article is to describe how focus groups, existing decision aids, and individual interviews were used to develop and improve a Spanish-language hospice educational video targeting Latino subgroups with linguistic, cultural, and educational barriers. These steps may provide guidelines for developing and revising health-related videos targeting other minority ethnic groups.
Introduction
Hospice represents the most comprehensive set of services that focus on comfort in the end of life, typically the last 6 months of life. 1 –3 However, the reality for the majority of hospice patients is that referral to hospice care occurs so close to the day of death that it is unlikely to provide much assistance or comfort to them. 4 –7 One of the reasons for delayed use of hospice is inadequate knowledge of hospice, which is a particular concern for the Latino community. 8 –12 Latinos, particularly those with low education and limited English proficiency, 13,14 are most likely to have not heard of hospice and to have a misunderstanding of hospice. 9,11
Although more timely hospice enrollment may be possible when information about hospice is provided earlier in the illness course, clinics and hospitals serving Latino patients including undocumented Latino immigrants are often faced with language barriers and limited knowledge of cultural factors and beliefs related to hospice decisions. 1,15 –17 Research with Latinos and clinicians serving Latinos suggests that medical mistrust and cultural barriers to discussion of hospice and death exist. 18 –24 Such research warns that misconceptions about hospice cannot be dispelled simply with Spanish fliers or pamphlets; it is recommended that one-on-one discussion is the best way to deliver hospice information and that such discussion can be successfully achieved with a volunteer coming from the Latino community because of the trust that will be accorded these community residents. 20 –22
Existing materials, including videos, for Spanish speakers for end-of-life care decision-making hardly meet such recommendations. For example, even when the narrative accompanying the video is in Spanish, the ethnicity of the patients and family members in the video is Caucasian. 25 In the videos 26 –28 where patients and family are Latinos, a narrator explains hospice services and concepts, with the patient and family simply as background images.
Video Development Project
In 2012, we received funding to develop a short Spanish-language video to educate Latino families with terminally ill relatives about hospice. Given the location of our university near Hollywood and in a community with a large Latino population, we benefited from an abundance of talented Latino students and affordable filming equipment through professors from the Department of Cinema and Television Arts. Completion of the project took 3 full years. The primary aim of the project was to design and develop a culturally credible video with emphasis on authentic testimony. The video was to be short as we intended it to be used in physician clinics and hospitals, rather than as community outreach material. This article’s main objective is to report the steps we took to produce the video.
The process of developing and enhancing the video was completed in 3 phases. Table 1 summarizes data collection efforts through literature review, focus groups, and interviews for developing and assessing the video. Phase 1 developed the first video; Phase 2 enhanced it based on focus group feedback; Phase 3 produced the final video based on evaluation of its acceptability among Latino caregivers, physicians and hospitals.
Data Collection Methodology for Developing and Assessing the Hospice Decision Aid Video.
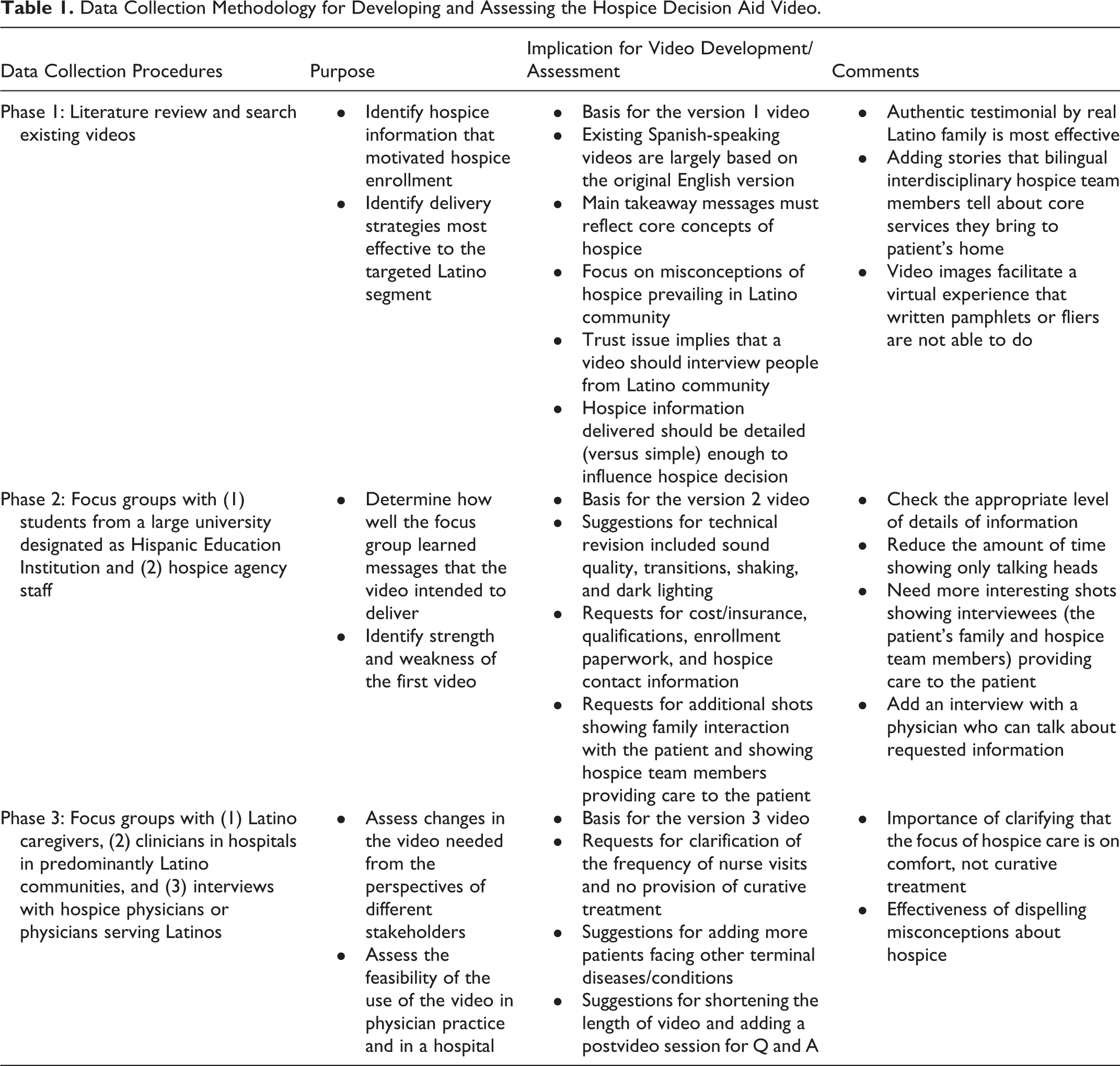
Phase 1
Through literature review of published studies, printed resources, and videos, phase 1 was to (1) determine video content and shooting strategies and (2) develop an initial video (version 1).
Literature review
Existing studies identified hospice information that was most influential in the hospice enrollment decision—hospice is “comfort-focused care, a 24-hour help by phone, and nurse and home health aide available.” 29,30 Research for decision aid tools in general suggests that information be detailed to affect decision-making. Video is generally better for getting detailed information across, especially to individuals with low education. 24 A well-designed video will be better than printed materials to dispel Latinos’ most common misunderstandings of hospice: (1) that hospice care is available only at a hospital or institution, not at home; (2) that hospice is only for imminent death; (3) that hospice means all treatment is stopped; (4) that once hospice takes over, the role of the family or the primary care physician in the management of the patient’s care ceases to exist. 18 –23
Analysis of existing Spanish-language videos 25 –28 suggests that a video depicting a real patient is the best and that such video with narrative proved to be more effective than verbal description alone. 25 Our video was designed to help viewers gain an appreciation of core hospice concepts by hearing from and observing the experiences of family members who have been the primary caregivers for hospice patients.
Producing version 1 video
Based on literature review and analysis of existing videos, we decided to make a video featuring a real patient with Alzheimer and the patient’s family members. We decided that end-stage Alzheimer was the best choice among many hospice diagnoses, since it places a high burden on caregivers and therefore provides a good illustration of a core hospice concept—supporting not only the patient but also caregivers. In addition to the patient and family, we decided to include interviews with many bilingual interdisciplinary hospice team members to illustrate another core concept of hospice care—the interdisciplinary team.
Through our alumni network, we contacted and made a contractual agreement with a local hospice agency in the summer of 2012. The agency agreed that a bilingual nurse working at the hospice would assist us in recruiting a Latino family who has a family member with Alzheimer receiving hospice care and would be willing to share their experience with hospice. In return, we agreed that we would allow the agency to use and distribute the video on digital versatile disc to the physicians in contractual relationships with the hospice agency.
Recruiting a Latino family meeting, our criteria turned out to be extremely difficult. After repeated failures, our hospice nurse finally turned to the coordinator of the Latino program of the Orange County Alzheimer’s Association, who helped recruit 1 family. The patient’s husband was a primary caregiver of a 68-year-old Mexican American woman at the end stage of Alzheimer. The functional assessment staging showed that she was at stage 7-F—she was bedbound, experiencing difficulty in eating and swallowing safely, and lacking the ability to communicate.
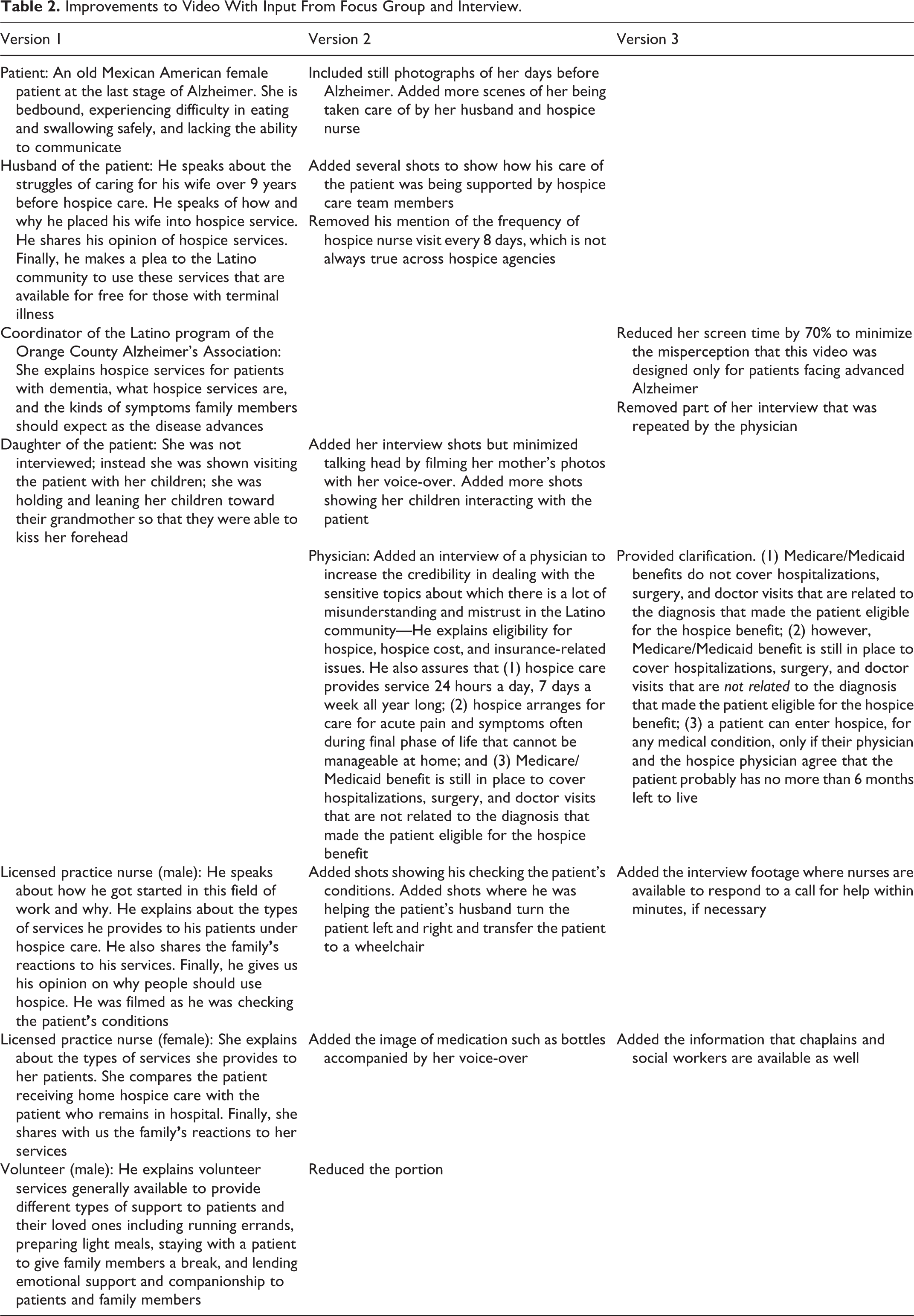
Table 2 presents verbal descriptions of version 1 of the video, along with versions 2 and 3. The video contains interviews with the hospice patient’s husband, daughter, and grandchildren, 2 hospice nurses, a hospice volunteer, and the Alzheimer program coordinator. They all speak Spanish, including the Caucasian hospice volunteer. In our video, the emphasis was on showing core hospice concepts rather than telling. For example, while standard hospice educational material tells that a hospice patient can have quality of life with family members around, our video shows the patient’s daughter and grandchildren coming to visit and kiss her forehead. In another example, her husband was lifting the electric bed while the husband’s voice is heard talking about the types of equipment hospice provides. While concepts were shown, detailed information was narrated by the family members and hospice care team members.
Improvements to Video With Input From Focus Group and Interview.
Phase 2
The purpose of phase 2 was to refine the version 1 video. Phase 2 involved (1) conducting focus groups to assess the video’s effectiveness and obtain suggestions for video improvement and (2) developing version 2.
Focus groups
In the spring/summer of 2013, we conducted 3 focus groups with 47 students from a large university serving a community with a large Latino population in southern California and 1 focus group with 12 local hospice staff members we recruited from the hospice agency that helped recruit the hospice patient family for the video. The students and the hospice agency staff members were selected for convenient sampling for quick feedback. The students had taken gerontology courses in which hospice was discussed as part of postacute care services. Nearly a third of the students identified themselves as a Latino/a.
Responses to the open-ended question about video improvement were placed into 3 categories: (1) technical issues such as screen shaking or dark lighting, (2) requests for more powerful shots that can facilitate virtual experience and engagement, and (3) requests for additional information directly related to hospice enrollment such as information about eligibility, enrollment procedure, or cost/insurance. We saw requests for practical information about eligibility, how to enroll, or cost/insurance as indirect evidence that the video was powerful enough to make viewers think of the next action beyond just learning about hospice.
Answers to the open-ended question about strength of the video largely suggested that the video was developed as we intended. A majority of participants mentioned “authentic,” “real,” or “realistic” words. Hospice staff used “culturally appropriate,” “culturally credible,” and “culturally acceptable” expressions. The most often mentioned expressions were “informative,” “detailed information,” “learned,” and “helpful information.”
Developing version 2 video
The biggest improvement in video 2 was to shoot a physician who is bilingual and regularly sees and refers terminally ill Latino patients to hospice. The decision to interview a physician was made because a physician is a credible authority suitable for sensitive topics about which there is a lot of misunderstanding and mistrust in the Latino community. 19,23,31 In the video, the physician explained basic cost- and health insurance-related issues and assured the availability of services such as short-term acute care of pain/symptoms in the inpatient setting that cannot be manageable at home, help available 24 hours by phone, and a doctor visit at home.
Phase 3
In 2014, we began testing the acceptability of the refined version 2 video among the targeted Latino segments and in its intended locations, including physician clinics and hospitals. Specifically, phase 3 involved conducting 1 focus group with Latino caregivers and interviews of clinical experts (1) to assess the effectiveness of the video and the feasibility of integrating the video into physician clinic practice and the process of hospital discharge and (2) to further enhance the video. This article focuses on changes in the video that the participants recommended.
Focus group with Latino caregivers
We recruited 12 Latino caregivers from the largest charity organization in southern California. Eligibility criteria were being Latino/a and the experience of currently providing care to ill relatives or having taken care of them. All the participants were of Mexican origin, and a local grocery store gift card of US$30 was used as an incentive. As expected, a majority of the participants belonged to the bottom tier of health literacy, scoring a range of 12 to 20 on Short Assessment of Health Literacy for Spanish Adults (SAHLSA-50) used widely in the field. 32 –35 Hospice knowledge test 10 administered before watching the video found that 9 of the 12 participants believed that hospice was only available at a hospital, consistent with the findings of previous studies. 10,11 Nearly all the participants mentioned that their communities had little knowledge about hospice and that this video would increase awareness of hospice availability. Two participants even asked questions about local hospice programs they could contact.
E-mail interviews with physicians
In addition to Latino caregivers, we sent e-mails to 12 physicians. They included 2 hospice physicians with whom the authors were acquainted and 10 physicians who volunteered to work in clinics in the charity organization from which we recruited Latino caregivers. Despite low response rate (3 responses), their comments were both encouraging and critical for revision of video content. Most important to the accuracy of the video, 1 physician serving as a hospice medical director expressed concerns that some information described by the physician speaker was misleading. Two statements in particular were pointed out—“You can enter hospice at any time and for any reason” and “Medicare will continue to pay for whatever doctor visits and hospitalizations the patient needs.” We realized that this happened when the physician speaker spoke too briefly. Outside of this request for revision, the physicians’ responses were positive, which was encouraging to us because it is well documented that for an intervention to succeed, physician buy-in is the most important but the most difficult element. 31
Focus group with hospital discharge personnel
In 2015, we conducted a focus group with 7 people from 4 hospitals in southern California—palliative care nurses, a case manager, a nurse practitioner, and a hospital administrator planning a hospital-based hospice program. As to the usability of the video in a hospital setting, 1 participant of Latino background mentioned the benefit of the video by relating her experience: “A very knowledgeable physician currently leads the palliative care conversation but there is a disadvantage of language barrier. When you get a translator, you don’t even know what kind of translation they are having. Even if you use a relative, if the relative is not comfortable about talking about hospice or if the relative is not ready for hospice, the message is sent totally wrong.” Another participant was concerned that the video’s seemingly exclusive focus on Alzheimer may not fit in a hospital setting, as patients referred by hospital personnel are far more likely to have diseases other than Alzheimer.
Participants from a hospital with a well-established palliative care consultation program suggested that the video could be used as part of palliative care consult. The suggested best timing of the video presentation was when they meet the family. They also mentioned that adding a postvideo session for questions and answers may be more effective than the video alone. On the other hand, participants from a hospital with no palliative care program expressed concerns about where and when to introduce the video.
Developing version 3
The final video production included (1) reshooting of the bilingual physician to address concerns about potentially misleading information and (2) the reduction of the portion featuring the coordinator of the Latino program of the Orange County Alzheimer’s Association.
Discussion
This article describes how we produced a hospice educational video targeting Spanish-speaking Latinos with terminally ill family members. Specifically, we describe how focus groups, existing decision aids, and individual interviews were used to develop and improve a Spanish language hospice educational video targeting Latino subgroups with linguistic, cultural, and educational barriers. These steps may provide guidelines for developing and revising health-related videos targeting other minority ethnic groups.
We envisioned that the video can help clinicians in clinics and hospitals to assist each Latino family with a terminally ill member who needs individual assistance negotiating hospice decisions and hospice care. For example, the video would greatly help clinics and hospitals that serve a large number of undocumented Latino immigrants with advanced cancer. 17 We ensured that (1) the video contains detailed information on hospice services that were empirically evidenced as most influential for hospice enrollment and (2) this detailed information be delivered in a culturally credible way to Latinos with cultural barriers of low educational background and limited English proficiency. Featuring a Spanish-speaking family member with a real patient and a bilingual hospice interdisciplinary team gave credibility to the video. Furthermore, incorporating knowledge from research conducted with the Latino community and gained from community participants helped to improve the cultural credibility of the video.
Throughout our development and enhancement efforts, we made no compromise with 1 criterion—less than 10 minutes of video length. The length is critical for the use of the video in a busy clinic and hospital. Keeping the video less than 10 minutes was especially hard because we tried to make the video as informative as possible. The detailed hospice information in the video was delivered through not only the Latino family’s personal testimonial but also bilingual interdisciplinary hospice team members’ stories about hospice. The following representative quotes from the study participants suggest that the video is well balanced: “It was very informational and to the point and yet it managed to tug at the heart strings.” “It was quick and informative. Sometimes informational videos go on and on. I think it ended at a good point.” “It was not filmed in a glossy, Hollywood way with sunsets and tear-provoking music. That appeals to me and it makes me trust it more.”
Testing the video with the sample of the intended stakeholder groups—Latino caregivers, physicians serving Latinos, and discharge planners in a hospital—gave further opportunities to enhance not only the acceptability but also the accuracy of the video. Their feedback confirms that the video successfully provides a virtual experience of being a caregiver for a hospice patient by enabling viewers to watch the services of hospice being delivered to a real hospice patient. This virtual experience in turn helps the viewers learn the core concepts of hospice with little effort. Positive feedback from focus groups suggested that the virtual experience is powerful when the video delivers personal stories, particularly when the stories come from people to whom Latinos can relate.
Despite our best efforts, there is still room for improvement in our video. First, we could not test our video using real Latino family members of terminally ill patients, although we developed the content of our video based on previous studies of family caregivers of decedent hospice patients. Second, we could not afford to incorporate all of the feedback that would have made our video better. One example of such feedback is as follows: “Show a scene of the husband caring for his wife without voice-over of talking head. Need to see the care in action in an intimate way—can be very brief, gives a break from constant talking and time for the viewer to reflect.” Third, the nationality of the patient and family in the video is of Mexican origin. Given there is a wide variation in nationality among Latinos, the usability of our video could be limited to Latinos of Mexican origin.
In summary, the goal of this article was to inform researchers who wish to develop educational materials targeting other racial/ethnic groups in the context of end-of-life care decision-making. We conclude with an emphasis that every effort should be made to ensure that such material is personally and culturally credible. Without such credibility, no matter how useful the information in the educational material is, it would not affect end-of-life care decisions, since end-of-life care decisions by different racial/ethnic groups are greatly influenced by their own end-of-life beliefs, concerns, and traditions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by NIH Grant # 1P20MD003938.