
Abstract
As the baby boomer generation ages, the need for palliative care services will be paramount and yet training for palliative care physicians is currently inadequate to meet the current palliative care needs. Nonspecialty-trained physicians will need to supplement the gap between supply and demand. Yet, no uniform guidelines exist for the training of internal medicine residents in palliative care. To our knowledge, no systematic study has been performed to evaluate how internal medicine residencies currently integrate palliative care into their training. In this study, we surveyed 338 Accreditation Council for Graduate Medical Education–accredited internal medicine program directors. We queried how palliative care was integrated into their training programs. The vast majority of respondents felt that palliative care training was “very important” (87.5%) and 75.9% of respondents offered some kind of palliative care rotation, often with a multidisciplinary approach. Moving forward, we are hopeful that the data provided from our survey will act as a launching point for more formal investigations into palliative care education for internal medicine residents. Concurrently, policy makers should aid in palliative care instruction by formalizing required palliative care training for internal medicine residents.
Introduction
It is estimated that by 2050, greater than 66 million Americans will be older than 65 years, many of whom will have multiple chronic diseases. 1,2 Accordingly, the need for palliative care services, for both symptom management and guidance with complex medical decision-making, will be forced into the forefront.
Unfortunately, we do not currently have enough palliative care physicians to meet the current need. Based on 2008 levels of hospice and palliative medicine trained physicians, there was a shortfall of approximately 4487 hospice and 10 810 palliative care physician full-time equivalents to match the need. 3 Lupu conservatively estimated that a minimum of 269 physicians would need to be trained annually to keep pace with those retiring. As of 2013, only 178 palliative care fellows were being trained annually, far too few to keep up with the projected need. 4
Accordingly, nonspecialty-trained physicians and nonphysician practitioners will need to provide the majority of palliative care in the future. It is imperative that residency programs impart palliative care training to their residents in an effort to fill the expected dearth of expertise.
Currently, the Accreditation Council for Graduate Medical Education (ACGME) program requirements for graduate medical education in internal medicine only dictates that residents have the opportunity to experience palliative medicine, without required exposure. 5 The National Consensus Conference on Medical Education for Care Near the End of Life (EOL) has proposed 9 educational domains: pain assessment and management, nonpain symptoms assessment and management, ethics, physician–patient communication, EOL communication, psychosocial care, death and dying, personal awareness, and EOL clinical experiences. 6 In a survey of 29 specialties that dealt with EOL care, Weissman and Block found that geriatrics, internal medicine, and neurology had the highest EOL emphasis but that the training was far from uniform in content. 6
To our knowledge, how internal medicine residencies incorporate palliative care training into their programs has not been looked at systematically on a national level. This has been previously attempted in the pediatric literature. In 2007, Baker et al looked at palliative care and EOL education in pediatric residencies. Surveying 246 directors, they found 41.8% of the pediatric residency programs received direct palliative care education, with the majority occurring during hospital rotations. Sadly, only 38% of the directors surveyed indicated that their graduating residents were competent in pediatric palliative care. 7
The goal of our article is to evaluate the prevalence and use of palliative care training in ACGME-accredited internal medicine programs. Given the authors’ affiliation at the time of the survey, a secondary goal from this study is to assess if the palliative care training at Harbor-UCLA is on par with national standards.
Methods
We sent out a Web-based survey (http://www.surveymonkey.com/) to the ACGME-accredited internal medicine residencies’ program directors based on available contact information on the ACGME’s (http://www.acgme.org/) and American Medical Association’s Web sites (http://freida.ama-assn.org/). There are approximately 400 ACGME-accredited internal medicine programs, for which we were able to generate 350 contact e-mails. Twelve of the e-mails were not accurate, resulting in the invitations being bounced back. Respondents were asked via e-mail to participate in the survey, which was completely voluntary. It was estimated that the survey would take no more than 5 minutes of the respondent’s time. No compensation was provided for participating in our survey. The survey was open to participants from February 2015 to June 2015. The study was given an institutional review board waiver by the John F. Wolf, MD, Human Subjects Committee (reference #039983), as it was determined not to be a human subject research as defined by the Department of Health and Human Services and/or FDA regulations. The survey questions are listed in the Appendix.
The majority of the data collected from the survey was nominal in nature and was analyzed by the percentage of respondents with that response. Relationships between whether an internal medicine training program had palliative care and the size of the residency training class was analyzed using a chi-square analysis. Similarly, the correlation of whether a program had palliative care and whether it was affiliated with an academic center was also analyzed using a chi-square analysis. Statistical analysis was performed with IBM SPSS statistical software (version 23).
Results
A total of 84 (24.8%) responses were obtained out of 338 accurate e-mails. Using a 3-point Likert scale ranging from “not important at all” to “very important,” the majority of respondents indicated that they felt palliative care was a “very important” part of their residents’ training (70/80 respondents, 87.5%).
Of the responses, 63/83 (75.9%) reported that they offer a rotation in palliative care. The typical length of a palliative care rotation was between 1 and 3 weeks’ duration (38/63, 60.32%). Over half of the programs (37/63, 59.7%) included outpatient palliative care exposure as part of their curriculum, predominately through hospice (n = 28, 75.7%) and clinic (n = 28, 75.7%) settings. The relationship between offering palliative care and the size of the residency program (less than 20 residents per class vs greater than 20 residents per class) was not statistically significant (χ12 = 3.471, P = .104). Nor was there a significant correlation between affiliation with a university hospital (academic-based program vs community-based program) and whether palliative care training was offered (χ12 = 2.137, P = .212).
Of the programs with palliative care rotations, the majority of responding programs had a full-time palliative care faculty member on staff (55/63, 87%). Residents were exposed to an interdisciplinary palliative care team (59/63, 95%), typically consisting of a physician (58/63, 98.3%), nurse practitioner (49/63, 83%), and social worker (46/63, 78%).
Nearly half of the residency programs had required lectures as part of their curriculum (30/63, 48%). The distribution of lecture topics is listed in Table 1.
Lecture Topics Given During Internal Medicine Palliative Care Rotations.a
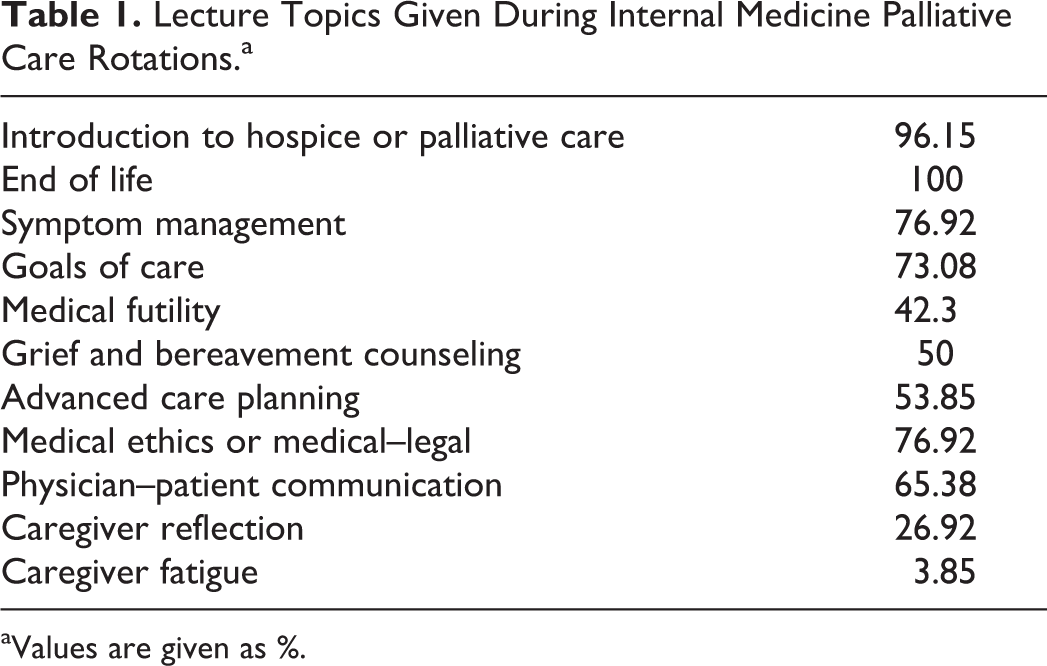
aValues are given as %.
Outside of a palliative care rotation, more than half (34/60, 57%) stated that their palliative care service was “very involved” with the internal medicine ward teams, based on a 3-point Likert scale from “not involved at all” to “very involved.”
Discussion
From our survey results, it is clear that ACGME-accredited internal medicine program directors in our response sample believe palliative care exposure and training is a “very important” aspect of an internal medicine resident’s training. Interestingly, while 87.5% believed it was “very important,” only 75.9% of survey respondents offered palliative care exposure. This may be due to limited resources or competing curriculum opportunities that every residency program director must decide. Greater than three-fourths of the survey respondents offered some aspect of palliative care training to their residents, a statistic that to our knowledge has not been previously evaluated. Unfortunately, the allotted time for a focused palliative care rotation was often only 1 to 3 weeks, with varying experiences offered.
It is unclear from our survey if exposure to palliative care training came from a mandatory rotation or an elective rotation. Based on individual responses, palliative care exposure may also be embedded into other rotations, such as geriatrics, or through scheduled grand rounds/morning reports throughout the year. We believe that both didactic and clinical exposure to palliative care are important components in the training of internal medicine residents.
The percentage of fellowship trained or palliative care boarded faculty at each site was not elucidated in our survey, which may affect the quality of palliative care education. Alternatively, we are aware that some institutions use nurse practitioners to manage their palliative care services. Encouragingly, the topics that the internal medicine residents were exposed to during this time correlated well with the National Consensus Conference on Medical Education for Care Near the End of Life summary recommendations. 6 These included an introduction to hospice or palliative care, EOL, symptom management, goals of care, and physician–patient communication (Table 1).
Regarding our study secondary aim, it appears Harbor-UCLA is grossly on par with the study’s respondents with the kinds of palliative care exposure provided to their residents, including both lecture topics and integration into a multidisciplinary team. As an emphasis is placed on an interdisciplinary approach to medical care, palliative care should be looked to as a model. In our survey, greater than 95% of respondents utilized some aspect of an interdisciplinary team during their palliative care rotation.
This survey had several weaknesses. The survey response rate was not as robust as we had hoped and is unlikely powered to generalize to other internal medicine programs. The low response rate also carries a risk for nonresponse bias. The response rate may have stemmed from the survey being entirely voluntary and only offered through e-mail. One can assume that internal medicine residency directors have significant amounts of e-mails to attend to daily, and distinguishing the survey’s e-mail from others may have been difficult. Nonetheless, the response rate was on par with the previously mentioned survey of pediatric residency program directors looking at palliative care education (22.4%). 7
In an effort-limit response bias, we looked at the residencies who responded to our survey versus all ACGME-accredited programs nationally. Comparing our respondents’ program characteristics to national data, respondent’s internal medicine programs had smaller residency classes (31% greater than 20 residents per class vs 42% nationally). Additionally, our survey respondents were more affiliated with community hospital internal medicine programs compared to the national data (23% respondent university affiliation vs 34.5% nationally). 4 Looking at regional distribution of residency programs, our survey responders were more likely to be from the Northwest (42% vs 32% nationally) and less likely to be from the South (20% vs 29% nationally). Percentage of survey responders from the Midwest and West appear to be within 2 percentage points of the national distribution. 8
It should be noted that our survey was chosen for ease of use and has not been validated against other cohorts, including internal medicine residencies who chose not to respond to our survey. Lastly, with regard to the question of whether palliative care was viewed as important, there may be a social acceptability bias driving the favorable responses seen in our survey.
While it is possible that the internal medicine programs that did not respond to our survey differ from the viewpoints of our respondents, palliative care exposure and integration should nonetheless be emphasized in internal medicine postgraduate education to ensure graduates are on par with the evolving US health-care environment. Palliative care provides a model for high-quality, patient-centered care that is cost-efficient and will need to be integrated into accountable care organizations. 9,10
Moving forward, we are hopeful that the data provided from our survey will act as a launching point for more formal investigations into palliative care education for internal medicine residents. Specifically, given the preponderance of program directors in our survey who feel that palliative care is very important, formal guidelines should be implemented in the next ACGME internal medicine program requirements draft revision. Similar calls have been voiced by American Academy of Hospice and Palliative Medicine (AAHPM) previously. 11 Individual internal medicine residency programs would be able to use ACGME’s revised guidelines to create mentorship programs and curriculum changes, ideally based upon AAHPM’s position paper for successfully developing academic palliative care programs. Formal curriculum changes have already been attempted on an individual institutional level but have yet to be adopted on a national scale. 12 The increased prevalence of palliative care in the hospital setting is already occurring, thus we need to expose our future physicians to palliative care in their training in order for them to competently transition into their future careers. 13
Conclusion
As internal medicine programs try to adapt to changing demographics and patient care needs, increased palliative care training is paramount. The vast majority of internal medicine program directors in our study recognized that importance. Future policy makers should aid in palliative care instruction by formalizing required palliative care training.
Footnotes
Appendix
Authors’ Note
Neither AE nor SN have any competing financial interests. AE and SN had full access to all of the data in this study and take complete responsibility for the integrity of the data and the accuracy of the data analysis. If interested, please contact AE for access to anonymous response data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.