
Abstract
Objective:
To describe the current landscape of palliative care (PC) in nursing homes (NHs) in New York State (NYS).
Measurements:
A statewide survey was completed by 149 respondents who named 61 different NHs as their workplace. Questions were related to presence, type, and composition of PC programs; perceptions of PC; barriers to implementing PC; and qualifying medical conditions.
Results:
Hospice is less available than palliative or comfort care programs, with three-fourths of NYS NH responded providing a PC program. In general, medical directors and physicians were more similar in perspective about the role/impact of PC compared to nursing and others. There was general agreement about the positive impact and role of PC in the NH. Funding and staffing were recognized as barriers to implementing PC.
Conclusion:
There is growing penetration of PC programs in NH facilities in NYS, with good perception of the appropriate utilization of PC programs. Financial reimbursement and staffing are barriers to providing PC in the NH and need to be addressed by the health-care system.
Introduction
Many long-term care nursing home (NH) residents have chronic medical conditions and/or acute life-threatening illnesses which can benefit from a “palliative care” (PC) approach to reduce symptoms and improve quality of life. 1 The National Consensus Project Guidelines for Quality Palliative Care was designed to direct the structure and development of PC services in US NHs. 2 Palliative care focuses on providing patients with relief from the symptoms, pain, and stress of a serious illness—whatever the diagnosis. Palliative care is provided by a team of doctors, nurses, social workers, and others who provide an extra layer of support. It is appropriate at any age and at any stage of serious illness and can be provided along with curative treatment. 3 The benefits of PC through symptom management, care coordination, and identifying achievable health goals can provide valuable benefits to a vulnerable NH population. 4
Palliative care is similar to hospice as a team-based approach to symptom management; unlike hospice, it does not require forgoing curative treatment and can be given concurrently while receiving subacute rehabilitation Medicare part A benefits. 5 The hospice Medicare part A benefit requires 6 months or less life expectancy for patients to forgo curative or life-sustaining treatment for their terminal diagnosis. 5 Although hospice has clearly defined benefits and services, the services provided in PC and “comfort care” can vary widely.
Clinical experience and research have demonstrated that written advance directives are not sufficient to assure that those who have serious, progressive, advanced chronic illnesses will have their preferences for medical treatment honored. 6 In response, medical orders such as the Physician Order for Life-Sustaining Treatment (POLST) form were created. The POLST form is a medical order for the specific medical treatments a patient would want or not want and is designed for individuals with a serious illness or advanced frailty near the end of life. 7 In New York State (NYS), the Medical Orders for Life-Sustaining Treatment (MOLST) form is used. Under NYS law, the MOLST is the only authorized form in NYS for documenting both nonhospital Do Not Resuscitate (DNR) and Do Not Intubate (DNI) orders and is also valid in the hospital setting. The signed MOLST form should be transported with patients as they travel to or transition across health-care settings. The medical orders on the form do not need to be reissued by the patient’s new health-care provider. However, the medical orders should be reviewed and may be revised by the physician when the patient transitions to a different health-care setting and when the patient’s preferences and/or medical conditions change. The NYS Department of Health updated the MOLST form in June 2010 to improve usability and to align the form with the Family Health Care Decisions Act that went into effect on June 1, 2010. 8
Hospice care in the NH setting has been associated with better pain treatment and fewer hospitalizations in the last month of life for those with hospice compared to residents without hospice. 9 –11 Additionally, studies suggest that quality of care is improved for NH residents who receive PC. 10,12 –15
A study showed an increasing trend between 2003 and 2007 of NH residents being transferred to hospitals at the end of life and dying in hospitals. 16 Anecdotal evidence suggests that NH may transfer patients to the hospital to avoid incurring the cost of providing intensive on-site care and because they lack resources, training, and support to serve dying residents. 16 These burdensome transitions are commonly associated with markers of poor quality in end-of-life care. 16 –18
The National Consensus Project Guidelines for Quality Palliative Care aimed to encourage and guide the structure and development of existing and new PC services in US NHs. 2 Since then, the field has evolved dynamically. Prior studies assessed PC use in NHs as reported by nursing staff. 19,20 Our study took a snapshot of the current state of PC landscape in NYS NHs. This study contributes to the literature in that it (1) surveyed multiple clinical disciplines in addition to nursing, (2) evaluated staff perception of PC and clinical conditions qualifying for PC, and (3) assessed broader issues including comfort care and hospice care.
Methods
This was a prospective survey and descriptive study of NH PC in NYS. The survey consisted of 15 questions and was created by the authors of this study. The survey was conducted from May 18, 2015, to August 3, 2015, and was adapted with permission from a prior survey of PC in the NH. 20 The survey included several domains: personal and institutional demographics, description of PC in the institution, and perception of PC. We asked questions about the presence of hospice care, PC, and comfort care in the facilities. For those who had a palliative program, the survey inquired about the duration and composition of the program. Our survey did not define the meaning of comfort care programs as they likely vary by facility and our goal was to evaluate formal PC programs specifically.
The survey collected data about respondent’s clinical role and duration of time they worked in the NH. We assessed the use of MOLST forms and funding for PC programs. The survey included perception questions about the role of PC, using an ordinal scale of 1 to 5 for responses of “strongly disagree, disagree, neither disagree or agree, agree, and strongly agree.” We included open-ended questions about “experiences with PC or thoughts about PC.” See Appendix A for surveys.
This survey was conducted online using Surveymonkey.com and was anonymous with voluntary participation. Participants were invited to participate via e-mail and had the option to be entered into a lottery to win 1 of 13 US$50 Amazon.com gift cards. The invitation e-mail was sent to physicians and medical directors of NHs in NYS through the list serves of several regional physician organizations (New York Medical Directors Association, Metropolitan Area American Geriatrics Society, and New York American College of Physicians). To improve response rates, the invitation e-mails were sent several times over the study period and the invitation asked participants to share with colleagues and staff.
Data were extracted from the online database, and an ordinal scale was applied for responses such that a score of 0 reflected strong disagreement and a score of 5 reflected strong agreement. As this was a descriptive study, associations between the demographic variables and the other questions on the questionnaire were evaluated to uncover possible significant trends, which might serve as topics for future research. Comparisons between groups with respect to the distribution of scores were performed via Kruskal-Wallis tests. Association between categorical variables was assessed via χ2 tests. Data were analyzed using SAS 9.3 (SAS Institute, Cary, North Carolina). Results were considered significant when P < .05.
Institutional review board’s review was not required because the study met criteria for exemption from such review because it is a quality improvement survey about institutional practices and policies and not human subjects research.
Results
We received 149 completed surveys. Sixty-one NHs were named in the survey. There are an estimated 650 NH in NYS, resulting in approximately a 9.3% response rate (Table 1).
Primary Role of Respondents in the NH.
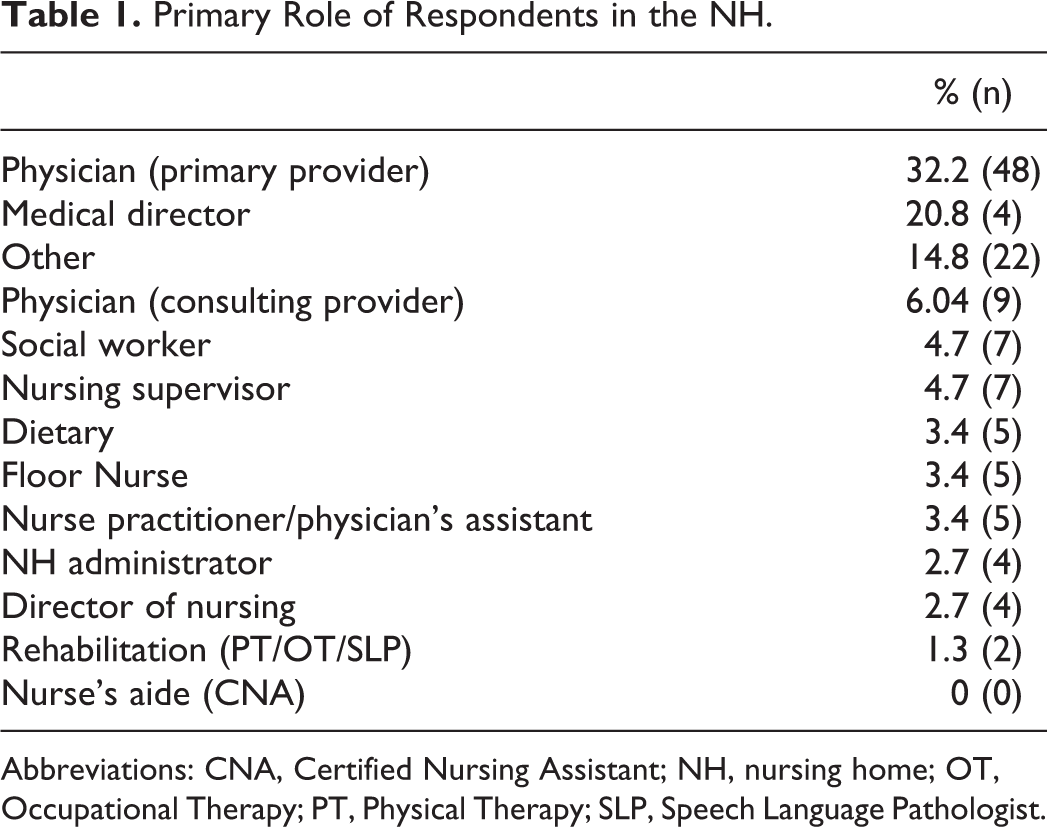
Abbreviations: CNA, Certified Nursing Assistant; NH, nursing home; OT, Occupational Therapy; PT, Physical Therapy; SLP, Speech Language Pathologist.
Respondent and Institutional Characteristics
Respondents included disciplines from dietary, nursing, midlevel providers, physicians, medical directors, social work, rehabilitation, and NH administrators. The largest group of respondents were physicians (including fellows trainees) as primary providers (32.2%) and medical directors (20.8%). Over 58% of respondents have worked in their current NH for at least 3 years, and 29.5% have worked there for 11 or more years. Respondents represented larger size facilities: 40% represented NHs with 100 to 200 beds and 44% represented facilities with over 200 total beds.
Presence and Type of Programs
In the NHs surveyed, there was less presence of hospice care (71.3%), compared to comfort care (79%) or PC (75.7%) programs. Of note, 16.9% of facilities have a mechanical ventilator unit. Of the 149 respondents, 60 (40%) reported information about the duration of PC program. Of these, 16.7% had a program for <1 year, 33% had a program for 3 to 5 years, and 47% had a program for 6 years or longer. Use of the MOLST form varied, with 96 (64.4%) respondents reporting using the MOLST. Of the 61 respondents who reported how long they’ve used the form, over half (55.7%) have used it for 3 years or more, whereas 21.2% have used it for under 1 year.
Team Composition of PC Programs
In facilities with formal PC programs, we asked who was included in the PC team and found variability in team composition. Physicians were most frequently included, while bereavement counselors were the least often part of the team (Table 2). This survey did not inquire specifically about who provides the PC in NHs, such as existing NH employees versus contracting with outside providers.
Composition of Palliative Care Programs Listed in Decreasing Order of Frequency Each Discipline Is Included in the Team.
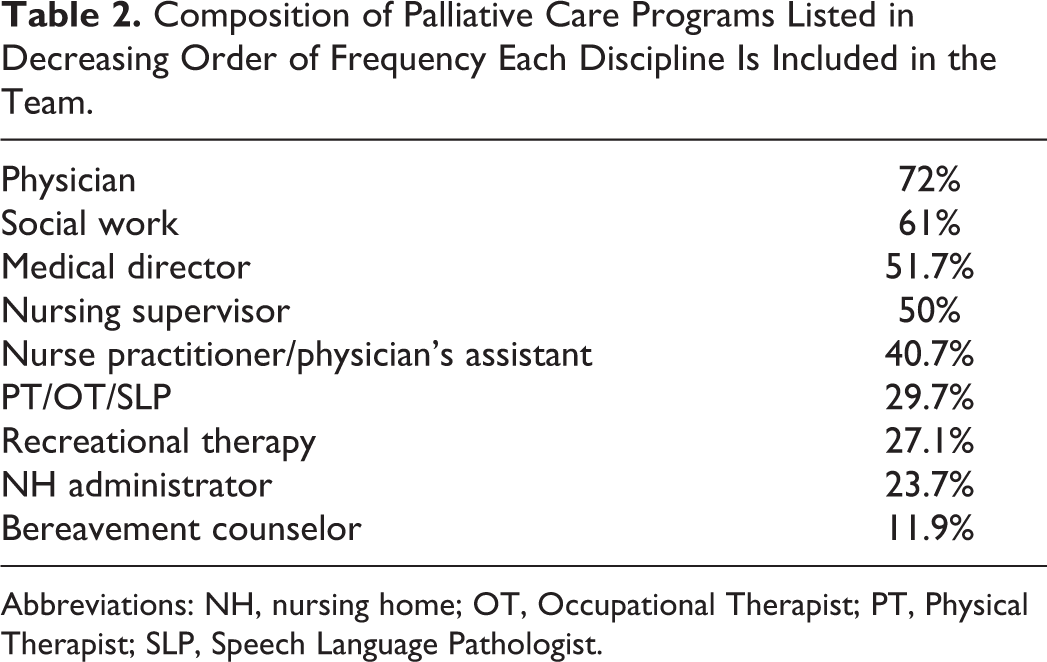
Abbreviations: NH, nursing home; OT, Occupational Therapist; PT, Physical Therapist; SLP, Speech Language Pathologist.
Perceptions About PC
There was general agreement about the positive impact and role of PC in the NH environment, with most respondents answering “correctly” about most of the questions. The “correct” answers were determined by asking local PC experts for what they consider the correct or most appropriate answer to the questions (Table 3).
Perceptions About Palliative Care in the NH.a
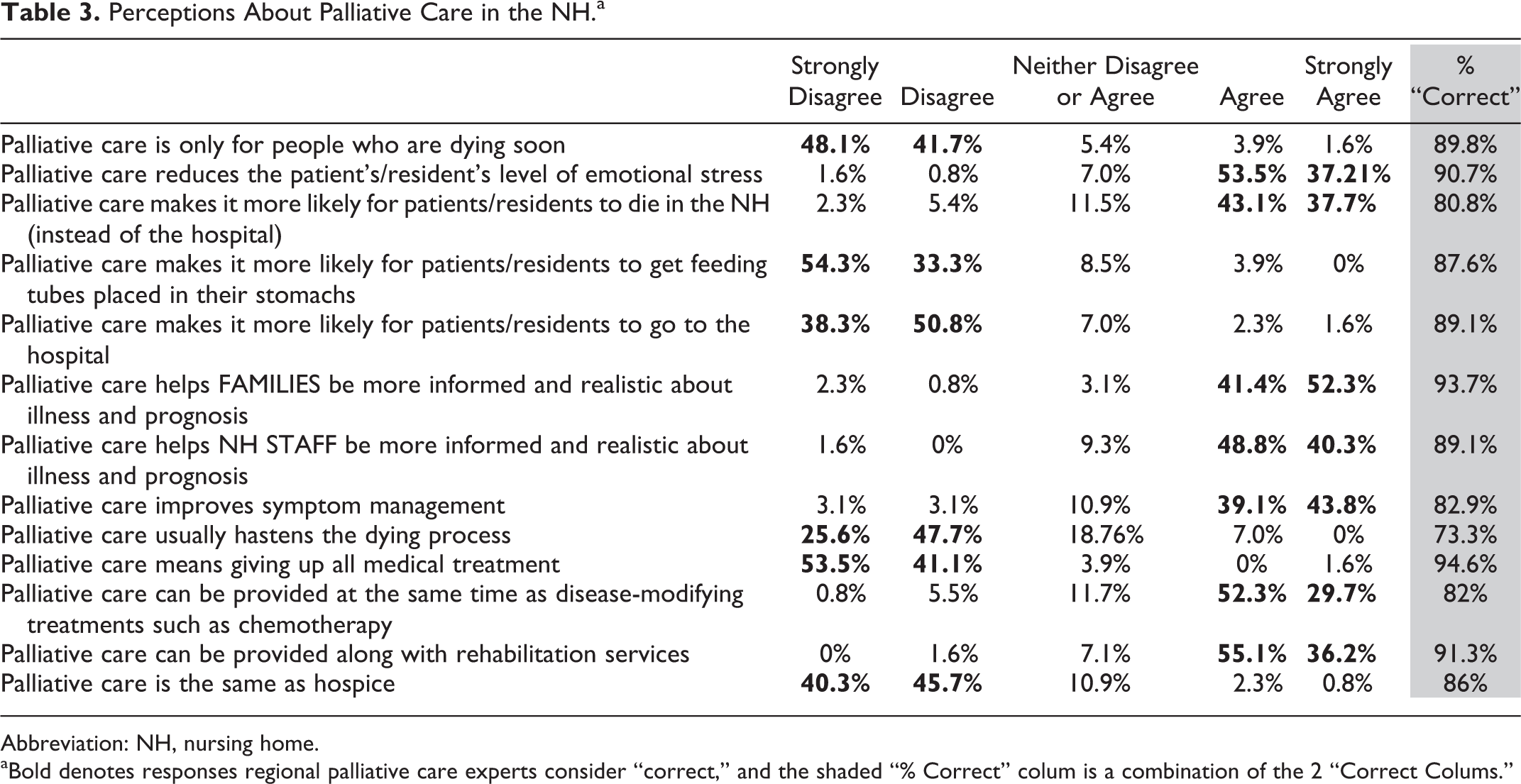
Abbreviation: NH, nursing home.
aBold denotes responses regional palliative care experts consider “correct,” and the shaded “% Correct” colum is a combination of the 2 “Correct Colums.”
We assessed whether the duration or maturity of the PC program impacted respondents’ perception about PC. Perception about PC was not impacted by duration of existence of PC program within the NH, with the exception of 1 question. The distribution of scores for “Palliative care is only for people who are dying soon” differed depending on the length of time the facility was reported to have a palliative program (P = .01). For example, 100% of programs that had a program for over 6 years disagreed or strongly disagreed with this statement, compared to 94% of respondents from programs present for 0 to 5 years and 84% of respondents with no program or who were unaware of any PC program.
Barriers to Implementing PC
Funding challenges for PC in NHs
Only 7.9% of respondents “strongly disagreed” that it is difficult/challenging to fund PC in NHs, whereas 49.1% either “agreed” or “strongly agreed” with that statement. Very few programs have outside funding: 4 have private grants and 3 have government grants. Twenty-seven respondents say the providers do their own billing as consultants.
Staffing challenges
A total of 56.6% reported it is difficult/challenging to find PC-trained physicians to work in NHs and 54.9% reported it is difficult/challenging to find PC-trained nonphysician staff to work in NHs.
Resident Conditions That Qualify for PC Services
The survey assessed what types of patient conditions should qualify for palliative services in an NH facility (Table 4).
Respondents’ Belief That Certain Conditions Should Qualify for Palliative Care in the NH.a
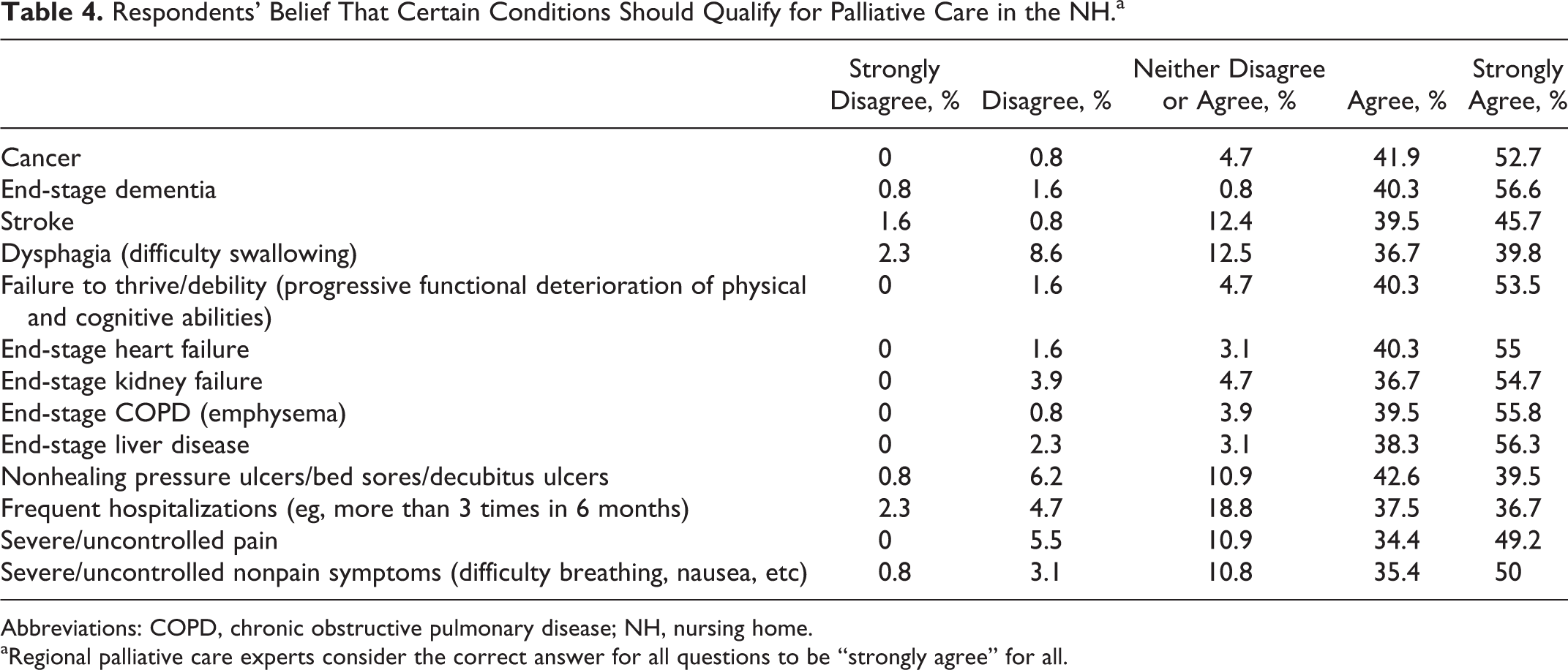
Abbreviations: COPD, chronic obstructive pulmonary disease; NH, nursing home.
aRegional palliative care experts consider the correct answer for all questions to be “strongly agree” for all.
Interdisciplinary Variations in Staff Perceptions About PC
Does PC make it more likely for patients/residents to die in the NH instead of the hospital? We assessed differences in the distribution of responses by discipline and observed a statistically significant difference such that medical directors and physicians had higher median scores compared to nursing (P = .04). Nursing agreed or strongly agreed with the statement 42% of the time, while medical directors and physicians agreed or strongly agreed 88.9% of the time.
Can PC be provided at the same time as disease-modifying treatments such as chemotherapy? We found interdiscipline variations: 86% of physicians replied “agree or strong agree,” medical directors 78%, nursing 67%, and others 78% (P = .02). Similarly, the percentage who “agree or strongly agree” that PC can be provided along with rehabilitation services varied: medical director 97%, physician 91%, nursing 91%, and others 83% (P = .04).
Does PC mean giving up all medical treatment? There were statistically significant differences in the distribution of responses across disciplines (P = .01) such that the percentage of respondents who replied “disagree or strongly disagree” were as follows: medical director 100%, physician 97%, nursing 83%, and others 89%.
Qualitative Reflections on PC
Respondents were asked to comment on “any experiences with PC or thoughts about PC that you would like to share.” Responses were in 3 broad categories: palliative as a positive experience, reflections on hospice, and current barriers to PC in the NH (Table 5).
Qualitative Reflections on Palliative Care.
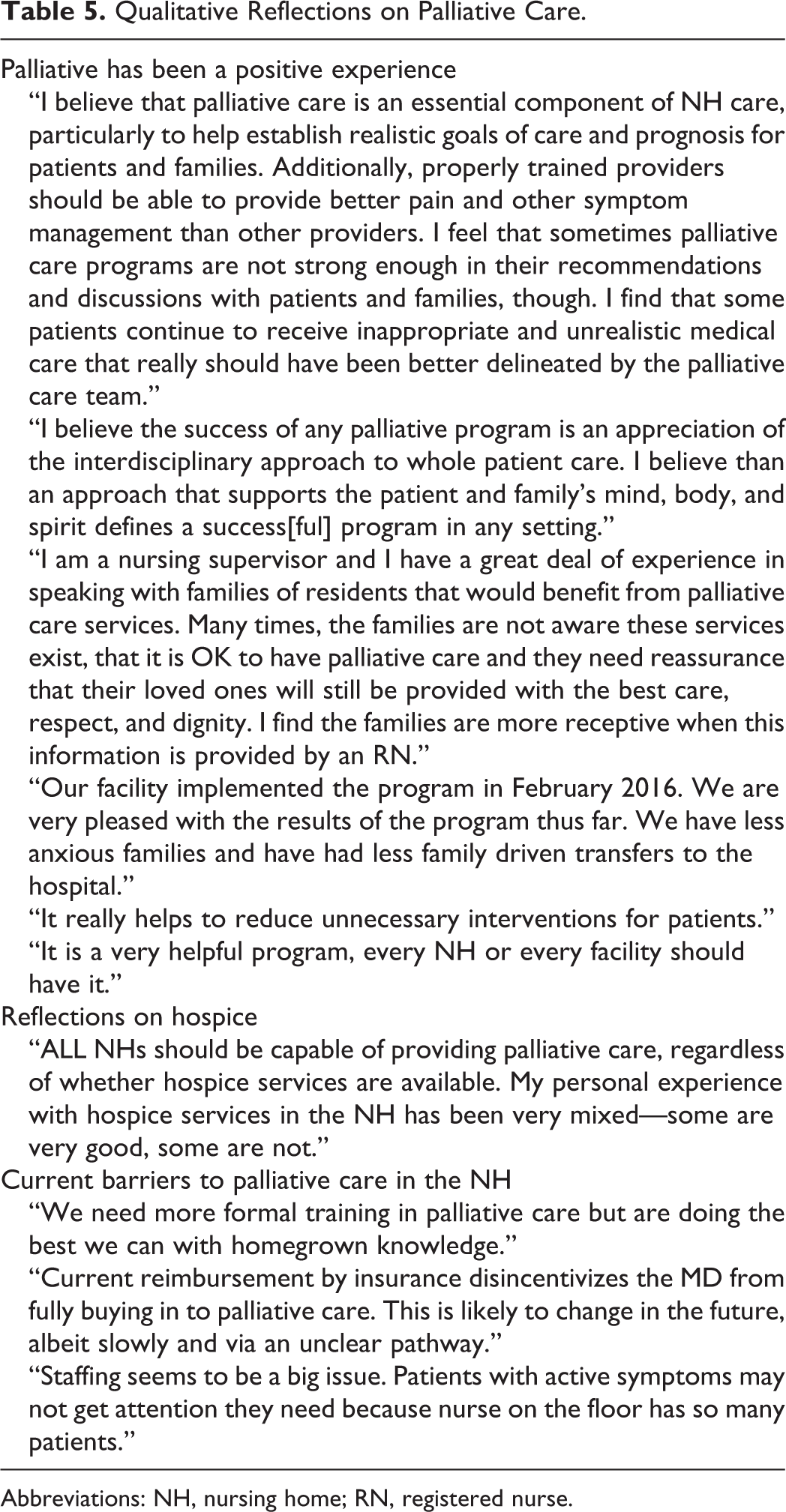
Abbreviations: NH, nursing home; RN, registered nurse.
Discussion
This study shows that 3 quarters of the 61 NYS NHs that responded reported availability of PC programs, demonstrating a significant presence of PC in the NH setting. Almost half (47%) of those with PC programs have been present for 6 years or longer, which demonstrates longevity and implies value of having the program present. Programs were generally interdisciplinary, which is appropriate and recommended by the National Consensus Project Guidelines for Quality Palliative Care. 2,21
The lower presence of hospice programs compared to PC programs in the NH is interesting and merits further investigation. It is plausible that the presence of a comprehensive PC program may reduce the need for hospice presence as on-site staff is better equipped to manage end-of-life care. Other factors may include the following: the generally lower reimbursement rate for long-term care beds through hospice, physician billing complexities associated with hospice, and clinician and/or families’ negative perceptions about hospice.
Most respondents demonstrated good understanding of the role of PC. The percent of what is considered correct answers about the role of PC ranged from 80% to 94%, except for the question concerning whether PC hastens the dying process. The overall good understanding reflects a growing recognition in the health-care community about the role and impact of PC.
This study helped identify barriers to implementing PC in the NH environment. (1) Limited availability of PC-trained or PC-certified physicians and other staff has made it challenging for facilities to implement and maintain programs. (2) Financial barriers exist as well. Palliative care is time consuming but not well reimbursed. Providers and facilities may find it difficult to prove cost “savings” by avoiding unnecessary tests, procedures, or hospitalizations. Palliative care providers may not want to be perceived as trying to “save money” for the health-care system, for fear that some patients and families might consider that to mean limiting care for financial reasons instead of based on achievable health goals.
This study suggests that providers in NHs with PC programs quickly understood the role of PC since 12 of the 13 “perception” questions were answered correctly regardless of duration or maturity of the NH PC program. The only exception was the question about “Palliative care is only for people who are dying soon”—which mature programs responded more correctly.
The qualitative reflections on PC in the NH demonstrate the perception that PC has provided benefit to patients, caregivers, and staff by providing a more interdisciplinary approach and by reducing unnecessary hospitalizations. Also expressed was interest in more formal training in PC as well as better reimbursement for PC providers and improved staffing to provide PC.
This study found interdisciplinary variations in perception about PC in the NH based on clinical roles. In general, medical directors and physicians were more similar in perspective compared to nursing and others. Nurses appeared to have a lesser grasp of PC: Less than half of nurses agreed that “Palliative care makes it more likely for patients/residents to die in the NH instead of the hospital”; Nurses and other staff disagreed that “Palliative care means giving up all medical treatment” at significantly lower rates than physicians and medical directors did. This suggests that targeted educational efforts should be made for nursing and other clinical staff about the role of PC. This is especially important in the NH milieu where nurses are front-line providers to frail elderly patients who are seriously ill.
Current NH regulations and quality reporting continue to have little focus on end of life and PC needs. The lack of explicit payment for PC in the NH beyond the basic daily rate can limit the ability of facilities to provide such care which is usually more time consuming, especially when patients are actively dying. 1,19 Reimbursement for physician services in PC does not reflect the provision of communication about complex medical care, goal setting, difficult decision-making, or acute symptom management, thereby providing low compensation for complex work.
Palliative care in the postacute setting for rehabilitation patients can manage distressing symptoms for patients who might otherwise need hospice for symptom management but could still benefit from restorative therapy. For some, better symptom control through palliative interventions may enable patients to participate more fully in physical therapy and improve functional status.
There are some limitations to this study. (1) This study surveyed only 1 state, although respondents represented various geographic regions and sizes within NYS. (2) There may be a response bias associated with a greater participation rate by respondents who have hospice, palliative, or comfort care programs, and the response rate was not as high as desired. However, our results do not show uniform use of PC services or consistent perspectives about the role of PC in the NH. (3) Results are based on self-report. Although self-administered surveys inherently provide subjective responses, this is a reasonable tool to assess facility policies and practices. Surveys were completed anonymously and without time constraint. (4) The response rate of 9.3% may seem low, however, external surveys commonly generate a 10% to 15% response rate, and a similar survey about PC in NHs nationwide had an 11% response rate. 20,22 Additionally, 43 of the respondents did not name their facility, so it is likely that more facilities were represented than the 61 that were named.
Conclusion
This study found growing penetration of PC programs in NH facilities in NYS, with good perception of the appropriate utilization of PC programs, although there were interdisciplinary differences. Financial reimbursement and staffing were clear barriers to providing PC in the NH environment and need to be addressed by the health-care system.
Footnotes
Appendix A
Authors’ Note
Dr Lester contributed to study design and conception, data analysis, and preparation of the manuscript. Drs Kawai and Pan contributed to study design and conception, data analysis, and critical revision of the manuscript. Drs Rodrigues, Martins-Welch, and Lolis contributed to literature review, study design and conception, and review of the manuscript. Dr Shalshin participated in data analysis and review of the manuscript. Dr Fazzari provided statistical analysis and data review. All authors have contributed to the manuscript and have agreed with its submission. The research was solely funded by the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.