
Abstract
Objectives:
To address perspectives of cardiology fellows on the current state of palliative education and palliative and hospice resource utilization within their fellowship experiences.
Methods:
We conducted an online national survey of cardiology fellows during the 2015 to 2016 academic year. Survey questions aimed to assess perceived importance of palliative care education, level of palliative care education during fellowship, and the structure of palliative care support at respondent institutions. Responses were collected anonymously. A total of 519 programs, including subspecialty programs, were contacted.
Results:
We received 365 responses, a number that represents roughly 14% of all cardiology fellows nationwide during the 2015 to 2016 academic year. Fellows reported discordance in the quality of education between general cardiology and palliative care principles as it relates to care of the patient approaching the end of life. Fellows infrequently received explicit training nor were observed or mentored in delivering end-of-life discussions. Respondents reported an underutilization of palliative care and hospice resources during fellowship training and also a perception that attending faculty were not routinely addressing goals of care.
Conclusions:
Our survey results highlight a need for enhanced palliative care and end-of-life training experiences for cardiology fellows and also suggest underutilization of hospice and palliative care resources for patients with advanced cardiac diseases. These findings create a platform for future work that might: (1) confirm this training deficit, (2) lead to exploration of educational models that could reconcile this deficit, and (3) potentially help improve palliative care support for patients and families facing advanced heart disease.
Keywords
Introduction
By the year 2030, over 40% of the US population will have some form of cardiovascular disease. 1 Between 1996 and 2000, an estimated 50% of men and 46% of women died within 5 years of onset of heart failure (HF). 2 In 2013, 1 in 3 American deaths was attributable to cardiovascular diseases. 3 Heart failure is projected to increase in prevalence from 2012 to 2030 by 46% and affect more than 8 million Americans. 3 The total cost burden of cardiovascular disease in the United States is expected to exceed US$1 trillion per year by 2030. 1
With a higher proportion of patients spending time in the advanced stages of HF, there is increased suffering and decreased quality of life (QOL). 4 The majority of HF patients die of progressive pump failure, with significant symptom burden prior to death. 5,6 Reflective of evidence for an unmet need for palliative care options in the HF population, 7 in 2013, the American College of Cardiology/American Heart Association (AHA) guidelines included a class I recommendation for advanced care planning and palliative care support in patients with advanced heart failure (AHF). 8
Health-related quality of life (HRQOL) 4,9,10 is a multidimensional construct composed of physical, mental, and social well-being. 11 Palliative care support can impact HRQOL by decreasing pain and suffering, providing family support, and assisting with difficult treatment decisions. Although the benefits of palliative care integration have been established, palliative care continues to be underutilized in patients with advanced cardiovascular disease and often utilized too late in these patients’ clinical course to allow maximal benefits. 4
In this article, we describe perspectives of current cardiology fellows regarding advanced cardiovascular disease, end-of-life care, and palliative care education. We aimed to better understand the prevalence and spectrum of palliative care training in cardiology fellowship in addition to perspectives on how often palliative and hospice care are appropriately utilized in their patient populations. We hypothesized that fellows were not routinely trained to take care of patients with advanced cardiac disease and toward the end-of-life and that palliative care resources were underutilized during fellowship training.
Methods
Population
Our target audience was cardiology fellows enrolled in Accreditation Council for Graduate Medical Education (ACGME)–accredited programs for the 2015 to 2016 academic year. Programs included general cardiology, electrophysiology, AHF, and interventional cardiology. Fellows were contacted via e-mail through program directors and program coordinators. Available e-mail addresses were obtained through the Fellowship and Residency Interactive Database Access System. There were 193 accredited cardiovascular disease umbrella training programs in the ACGME database. Within these umbrella programs were subspecialty programs along with general cardiology programs. Thus, a total of 519 programs, including subspecialty programs within a larger general cardiology program, were contacted. E-mails included a request to send a read receipt and to forward the survey on to program fellows.
Survey Development
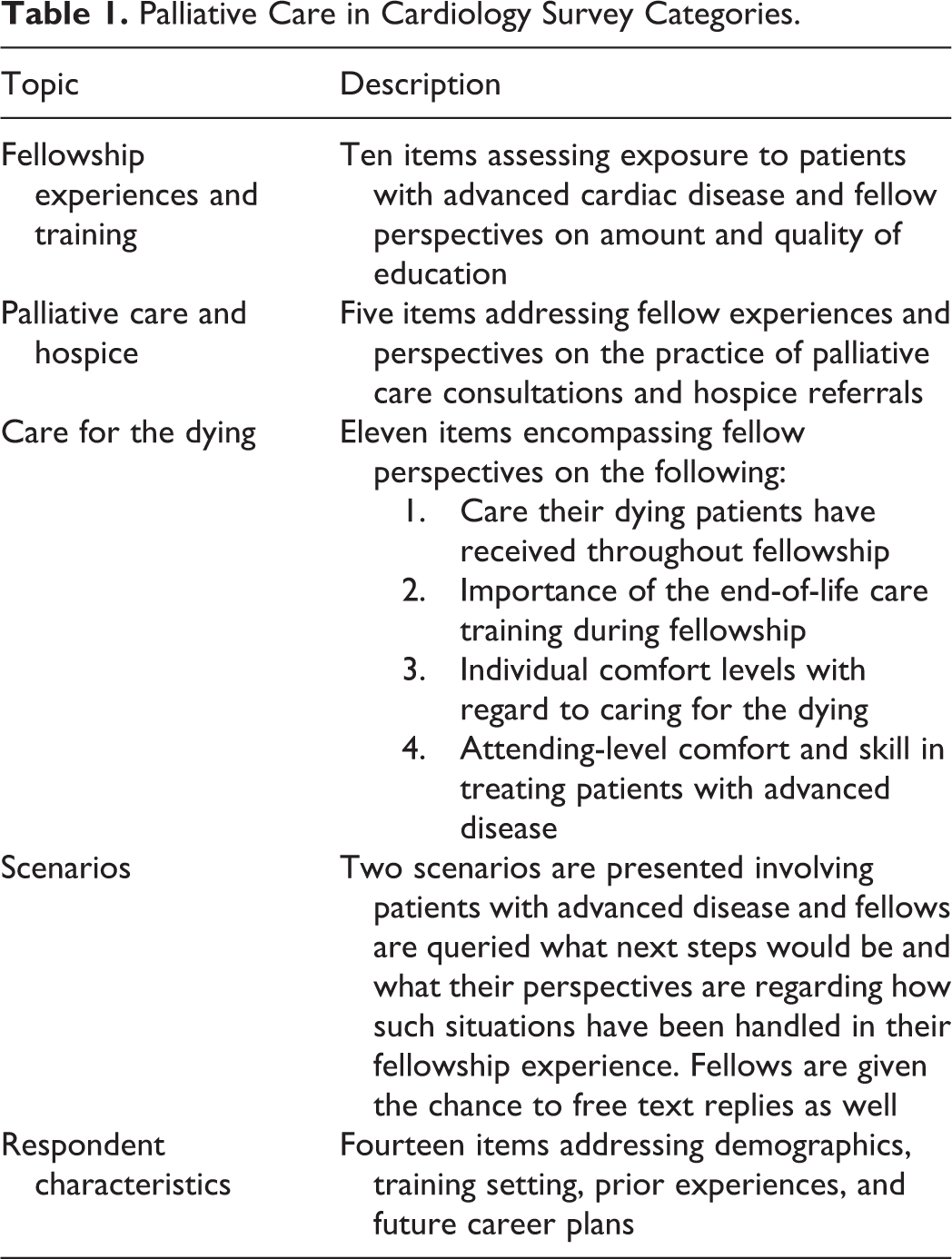
We adapted a previously utilized and published instrument 12 –14 to our cardiology domains. The survey consisted of 43 questions in 4 main categories, which included perceived strength of general cardiology and palliative care education, education in palliative approaches to end-of-life scenarios, and the need for palliative care consulting services (Table 1). We also included several clinical scenarios to gauge whether palliative care principles are actively integrated into fellows’ decision-making in difficult situations. This study was approved by the institutional review board of Medical College of Wisconsin.
Palliative Care in Cardiology Survey Categories.
Survey Distribution
The survey was created using SurveyMonkey and distributed using an embedded link in e-mails to program directors and coordinators. We asked that these contacts forward our initial e-mail to their fellows. A reminder to complete the survey was sent at 3 and 6 weeks after the initial e-mail, and the survey was closed after roughly 7 weeks. As an incentive, we offered the chance to win 1 of 5 US$100 raffled gift cards to fellows who participated.
Statistical Analysis
Descriptive analysis was performed for all responses. Student t test was used to compare the mean values as appropriate. A P value of <.05 was used to define statistical significance. All analyses were performed in STATA version 14.0 for Windows (StataCorp, College Station, Texas).
Results
There were 193 accredited general cardiovascular diseases training programs (many of which also had subspecialty programs) during the 2015 to 2016 academic year and about 2600 enrolled trainees in these programs during that time (https://apps.acgme.org/ads/public). Based on the replies from coordinators/directors and e-mail receipts, we estimate that fellows in roughly half of all programs had access to our survey through their respective contacts. The total number of survey responses we received was 365 (about 14%). Respondent characteristics are listed in Table 2. Most (91.9%) respondents reported the availability of an inpatient palliative care consult service in their training setting. Although few respondents participated in a palliative care rotation during fellowship, many (57.8%) reported rotating on a palliative care service during their residency training.
Respondent Characteristics.
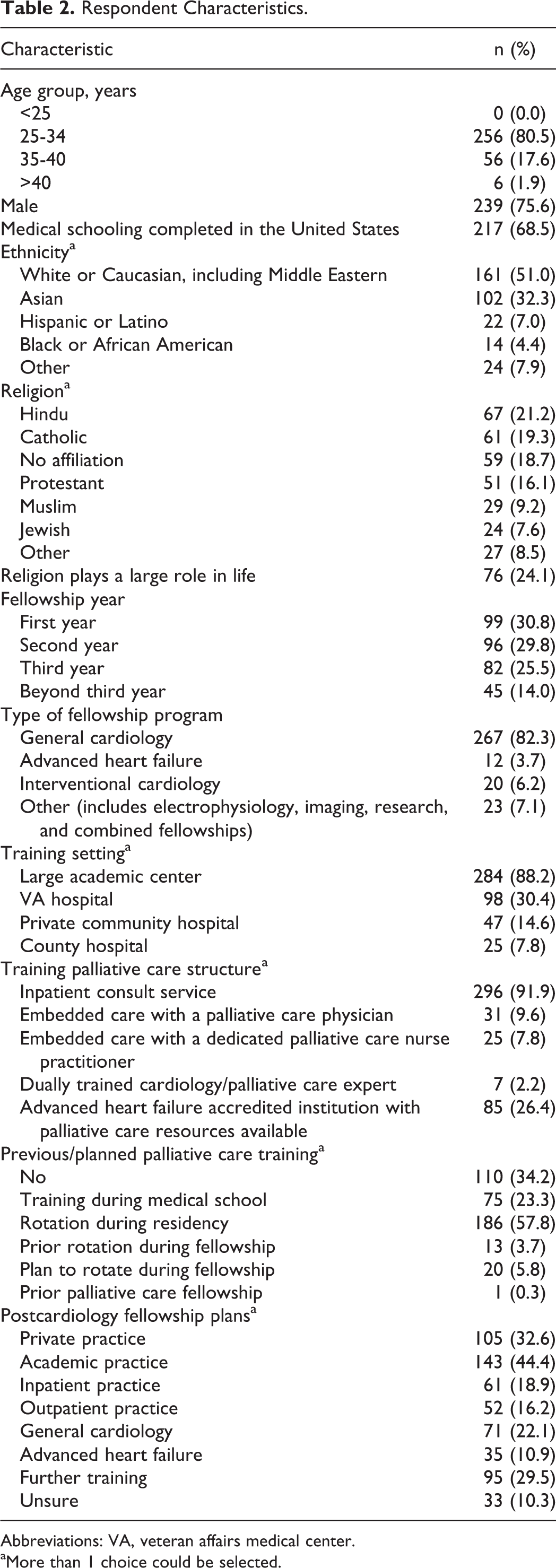
Abbreviations: VA, veteran affairs medical center.
aMore than 1 choice could be selected.
Of respondents, 83.6% of fellows reported frequently caring for patients with AHF and 73.7% of fellows reported frequently caring for a patient who is dying. Although fellows generally reported frequent teaching in the management of a patient with AHF, only 41.8% reported explicit teaching in the management of a patient who is dying. In terms of reported quality of teaching, 67.7% of fellows rated teaching of general cardiology principles as excellent, while this number was lower in the domains of end-of-life care, end-stage HF options, end-stage coronary disease options, and symptom control for a terminal or a dying patient (Figure 1). Compared to general cardiology principles, domains relevant to palliative management of cardiology patients (symptoms control for terminal/dying patients, end-of-life care) were felt to be taught at a significantly lower level of quality (P < .001). Although a majority of fellows reported discussing goals of care frequently (66.0% reported doing so more than 10 times and 12.9% 7-10 times), feedback was limited (Table 3). In addition, 13.2% of respondents reported not being confident in knowing the difference between palliative care and hospice (Table 3). This number was as high as 16.5% in fellows who were in their third year or beyond (data not illustrated). Of the 12 respondents who reported they were currently enrolled in an AHF program, 25% reported not being confident in the difference between palliative care and hospice.
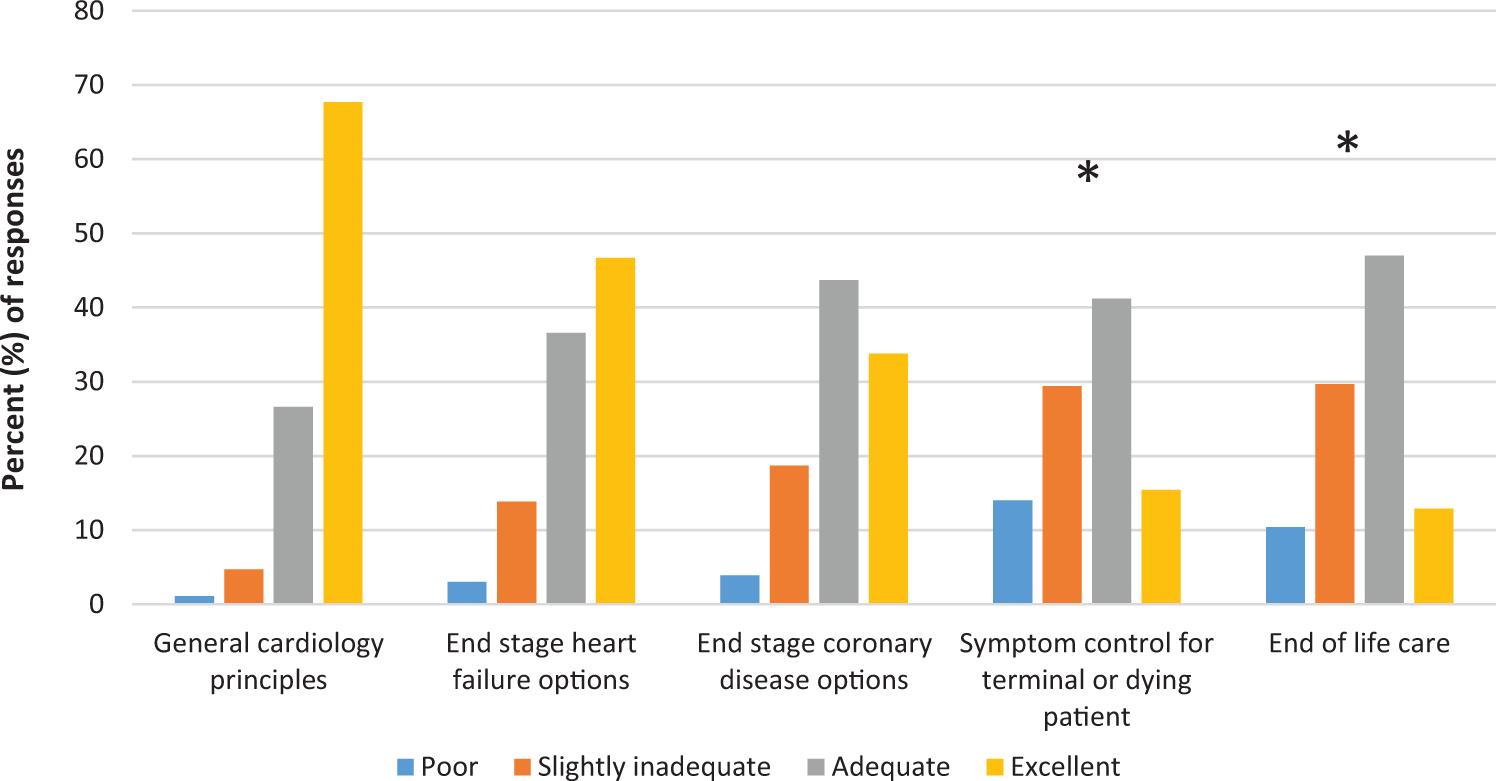
Perceived quality of fellowship teaching. *Significance of domains when compared with cardiology principles (P < .001).
Palliative Care Exposure.a
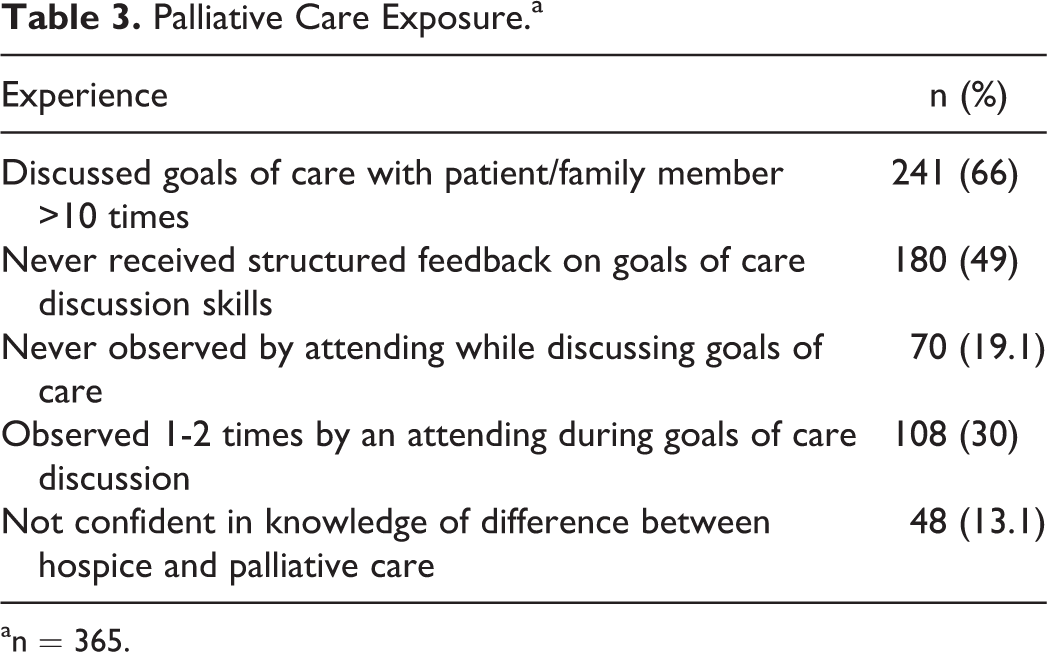
an = 365.
Perceived Importance of Palliative Care and Reported Referrals
We asked fellows how important it is for a cardiology fellow to learn to provide end-of-life care. Of respondents, 58.1% rated this as “extremely important,” 32.5% as “moderately important,” and 8.6% as “slightly important.” Among respondents, palliative care was reported to be useful in patients with end-stage HF or coronary disease “moderately often” by 40.6% and “extremely often” by 44.5% of fellows. Yet fellows reported consulting palliative care “extremely often” only 12.8% for their inpatients and 2.5% for their outpatients. A similar discrepancy in perceived usefulness of referrals and recollections of referrals made was seen for hospice. Hospice referral was thought to be important for inpatients by 49.0% of fellows. Only 8.7% and 2.3% of fellows reported referring an inpatient to hospice “extremely often” and “moderately often,” respectively. A similar pattern was reported for hospice referrals for outpatients, although the perceived utility of a palliative care consult for these patients was far lower (4.8% felt a referral to hospice was appropriately “extremely often”). Similarly, fellows reported that, despite anticipating their death, patients were infrequently enrolled in hospice at the time of death (Figure 2).
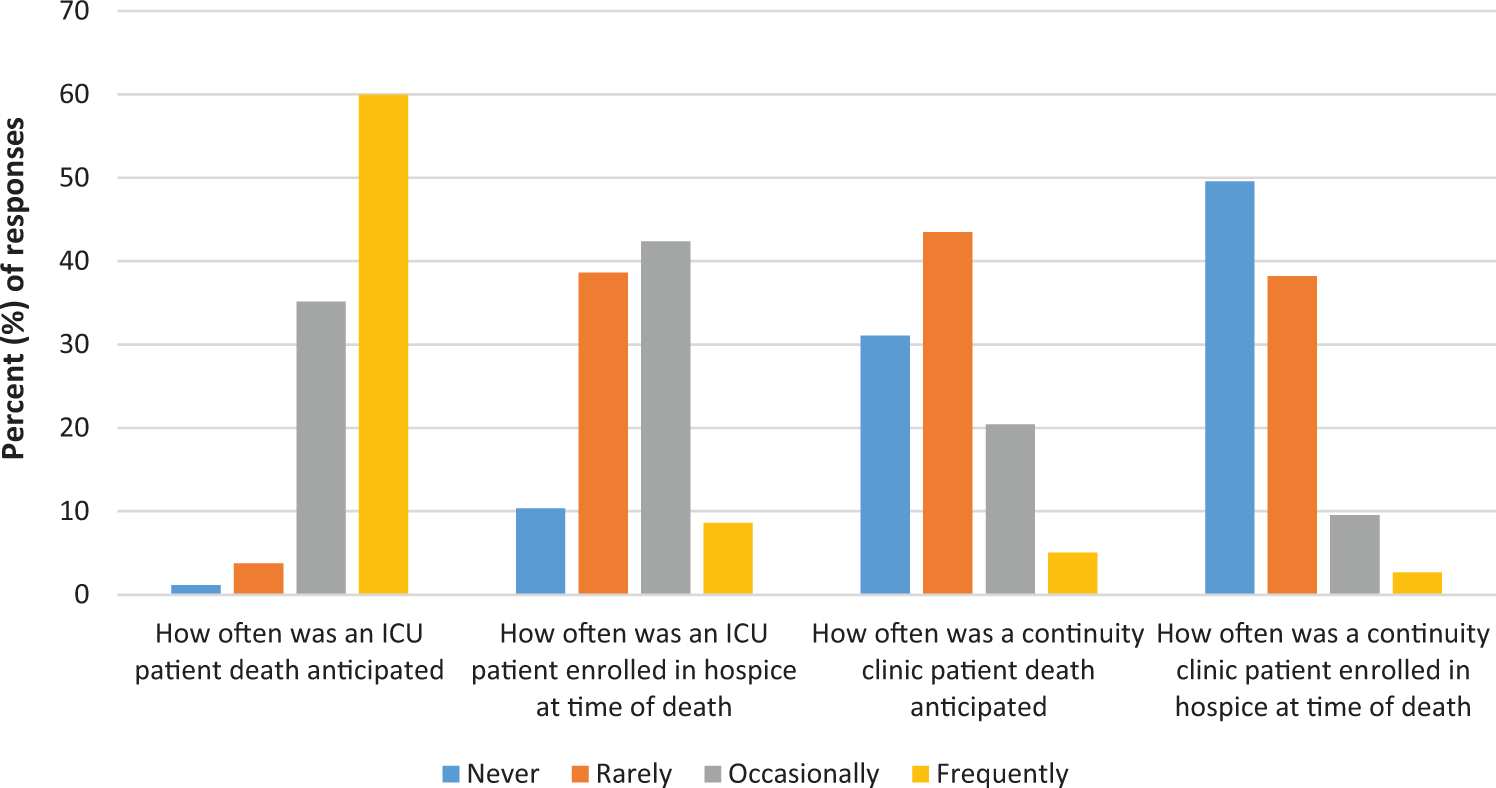
Recollections of relative hospice enrollment during fellowship.
Role Models and Perceived Preparedness
We attempted to measure whether fellows received informal training or exposure to palliative care through their cardiology attendings and whether this was enough to prepare them for independent practice (Figure 3). Of respondents, 57.1% thought their attendings addressed goals of care when appropriate. Only 52.6% thought their attendings did an exemplary job with end-of-life discussions. However, 63.2% of respondents strongly agreed that they feel comfortable addressing goals of care with a dying patient, and 49.0% and 33.4% of respondents strongly agreed and slightly agreed that they feel comfortable informing a patient that he or she is dying, respectively. Only 63.1% of respondents agreed that they are better now at end-of-life conversations than at the start of fellowship, and 64.7% agreed they are better now at caring for the dying than at the start of fellowship (Table 4). These numbers increased to 75% and 75.6%, respectively, in subgroup analysis of those in their third year of fellowship and beyond.
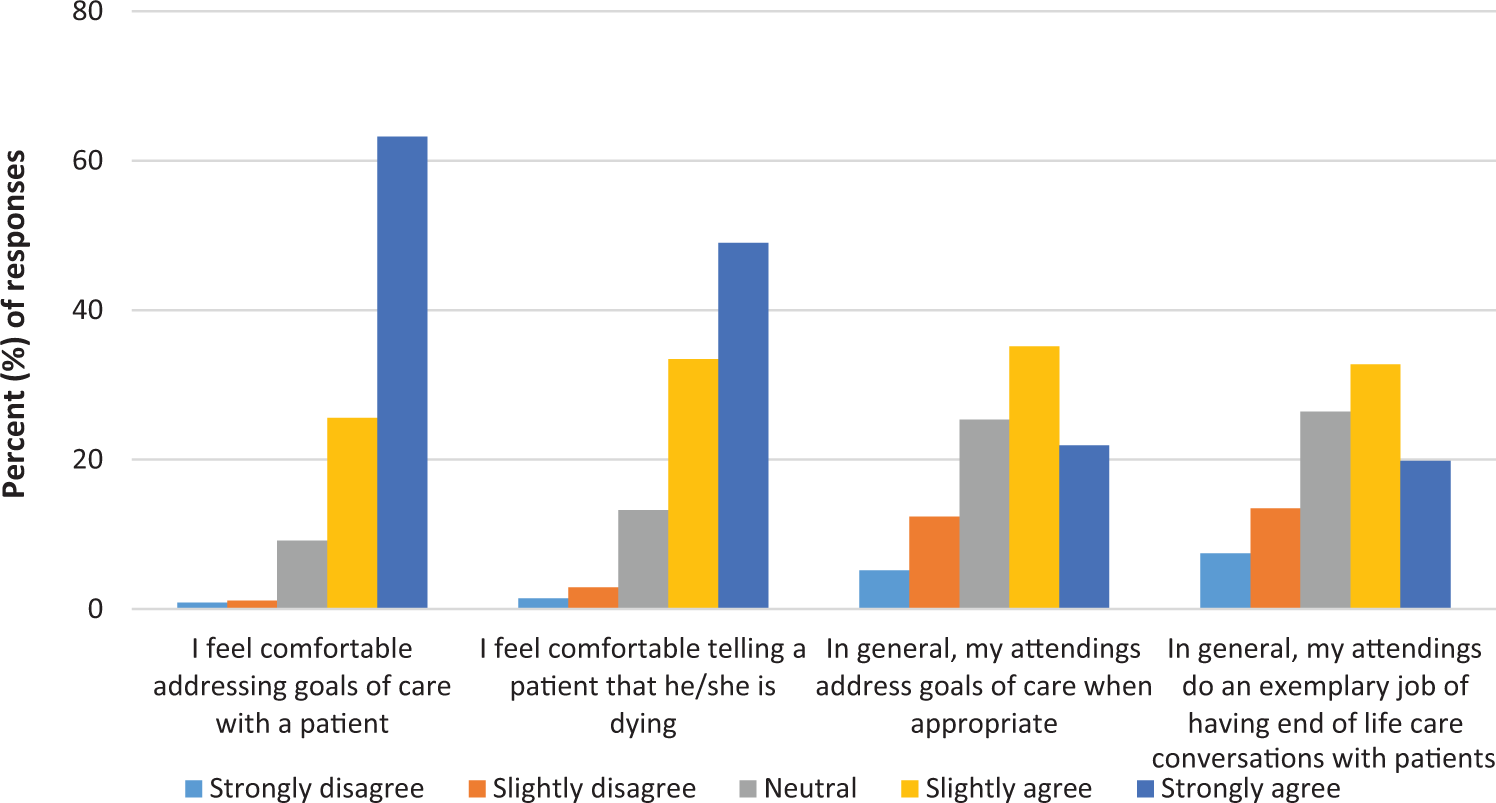
Experiences addressing goals of care.
Level of Preparedness Caring for Patients With Advanced Disease.a
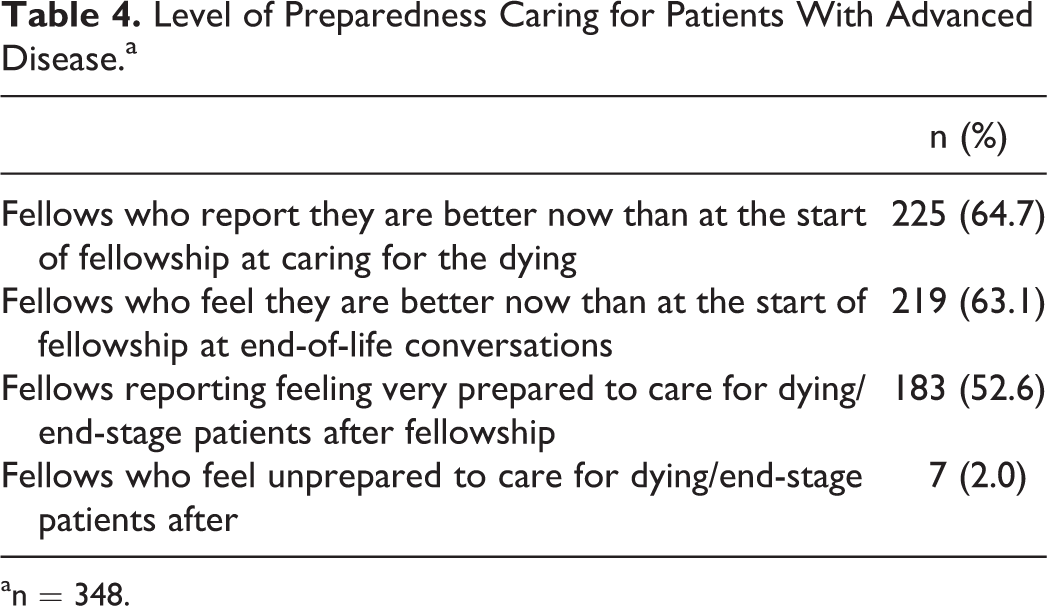
an = 348.
Discussion
This is the first nationally representative study of cardiology fellows’ self-assessment of palliative care education during their fellowship, a timely topic considering the prevalence and estimated national health costs of cardiovascular diseases nationwide. Recognition of palliative care needs in patients with advanced cardiovascular diseases has lagged behind recognition of these diagnoses as a major chronic health problem. 15 –17 A recent AHA and American Stroke Association (ASA) policy statement regarding palliative care and management of patients with advanced cardiovascular disease and stroke included comments on training of health professionals. 18 Our study addressed current cardiology trainees’ perspectives of their educational experiences with regard to palliative care approaches in cardiovascular diseases.
Deficits in Training
The overwhelming majority of fellows reported frequent experiences in the care of patients with advanced illness or those facing end of life and view formal training in this arena as important. Although formal palliative care training might increase the utilization of palliative and hospice resources as has been suggested, 4 our respondents reported a discrepancy in intensity and quality of training in palliative care compared to general cardiology principles. There was infrequent attending observation or structured feedback on communication skills during goals of care discussions. A similar gap between perceived importance of palliative care competencies and resident/fellow skill level in palliative care training has been reported in other disciplines. 12 –14,19,20 This training deficit may influence posttraining practices, as primary and subspecialty physicians frequently defer end-of-life conversations. This may also add to the dilemma that many of these discussions have to be initiated in an urgent or emergency department setting. 21 Recently published competencies in palliative care for cardiology fellows 22 detail education domains of care relevant to cardiology that may help to lessen the physical, emotional, and financial burden of patients and families.
Underutilization of Palliative care and Hospice Resources
Respondents reported underutilization of clinical palliative care and hospice resources for their patients during fellowship training, despite the recognition that patients had a limited prognosis and/or significant symptom burden. The majority of clinic patients were not enrolled in hospice at the time of death, and respondents reported patients frequently dying in the hospital. These findings may reflect not only challenges in determining prognosis for patients with HF 4 but also a knowledge gap in how to mobilize hospice resources for patients in the outpatient setting. Interestingly, instruments to determine when to refer HF patients to palliative care or hospice have been studied and have correlated with palliative care scales that estimate disease severity and thus could help direct timely referral to palliative care services. 23
American College of Cardiology/AHA guidelines now include recommendations for assessing prognosis and prompting advanced care planning. 4,24 Despite these guidelines and the evidence for increased QOL and cost savings with early palliative care support in other terminal conditions, 25,26 only 6% to 10% of patients with HF are referred for palliative care consultation. Referrals commonly do not take place until the last month of life. 17,27 In our study, many fellows perceived their cardiology attending physician’s skills in goal setting as less than optimal, consistent with studies of trainees in other fields. 12 –14,20 Upon consideration of a clinical scenario of a patient with end-stage HF, over 35% of fellows responded that their attendings would not want to consult palliative care, and over 70% of fellows responded that frequently such patients are treated for an acute exacerbation and discharged home with medical management without accompanying goal setting or discussion of prognosis.
Training–Confidence Mismatch
Most fellows felt comfortable addressing goals of care independently, yet many, and in particular, 25% of AHF trainees, were not confident they know the difference between palliative care and hospice. Despite commonly acknowledging their lack of palliative care formal education during fellowship or education by attending example, most fellows noted increased confidence in caring for the dying during the course of their fellowship. It is unclear whether this represents a lack of insight into their own limitations or whether fellows recognize the need for incorporation of more palliative care approaches as they take care of a sicker patient population. The fact that there were few reported hospice referrals does not lend support to the latter possibility, but this may simply mean that fellows did recognize the need for palliative care and hospice referrals yet felt these referrals might be discouraged by supervising attending physicians. Additionally, physicians often poorly assess their own competence. 28,29
In the current era, most hospitals have palliative care services. 30 Over 60% of fellows had had some training in palliative care either during medical school or residency, while the majority of cardiology fellowship attendings likely developed end-of-life care skills experientially in their practice. This is reflective of the efforts of several palliative care experts across the country to further the educational reach of the field 31 –33 and lends promise to the possibility of including formal palliative education programs in cardiology fellowships in the near future. Our overall synthesis of survey results offers promise of a paradigm shift in the field of cardiovascular medicine that can begin at the fellow level.
Limitations
This study had several limitations. The response rate lends itself to sampling bias, as respondents may already have strong feelings about the field of palliative care education, due to personal experiences, experiences with patients, or perceived lack of education in their programs. A variety of factors may have led to this low response rate. First, we relied on program directors and coordinators to honor requests to distribute surveys to trainees in their programs and requested read receipts. We received approximately 75 alerts that coordinators and directors were no longer with their respective programs, that e-mail addresses were not valid, or that our e-mail message was not read. These alerts suggest that a large group of fellows was not reached. Second, e-mail requests may have led to fewer responses, due to the volume of e-mails fellows receive. Due to the anonymous nature of the survey, we were unable to assess differences between programs that yielded different response rates. Additionally, experiences unique to programs may have been missed due to survey anonymity/inability to collect institutional data. We adapted questions’ response ratings (ie, slightly inadequate vs adequate or moderately often vs extremely often) from previously utilized instruments 12 –14 as described and did not offer guidance as to how to apply these ratings. This was a study of fellow perception, and thus, we left the interpretation of the rating to respondents. However, some respondents may have found our rating scale to be challenging and may have elected not to complete the survey. Additionally, while we only surveyed fellows, a survey of training program directors may provide more information regarding current training practices. Finally, recent data suggest that response rates of physician surveys are decreasing. 34 These findings are consistent with our data. Researchers who survey physicians are therefore left to use methods that may increase response rates, some of which we have employed to address this limitation. 34 –37 Despite these limitations, we did receive over 350 survey responses, which is larger than other fellow surveys published 12 –14,20 and serves as a good initial analysis of cardiology training practices.
Future Directions
For years it has been recognized that palliative care approaches can improve QOL and decrease costs spent toward the end of life. 4,24,26,38 The AHA/ASA policy statement published within the last few months again establishes recommendations for early palliative care in the management of patients with advanced cardiovascular disease and also addresses reimbursement for palliative care services and payer–provider relationships. It also recommends palliative care education for health professionals. 18 These reforms will hopefully increase referrals for “upstream” palliative care support, but they also highlight the pressing need for integrated primary palliative care education in specialist training in order to meet the future clinical demand.
Our study yields 2 major findings that need further investigation. First, we highlight an area in cardiology training with room for improvement, namely palliative and end-of-life care training for cardiology fellows. Second, our results point to an underrecognized need for palliative care resources in patients with advanced heart disease and underutilization of palliative and hospice resources that are not only available but also encouraged for these patients. 8 Although a mismatch between need for and access to palliative care has been recognized, 39 in our study, most fellows did report access to palliative care resources, suggesting there are additional barriers to address. Future training efforts could include creating educational paradigms that encourage trainees to readily assess and monitor QOL in their patients and to advocate for early palliative care and hospice referrals. Formal palliative care training during fellowship, in the form of a clinical rotation with palliative care faculty, regular scheduled didactic curricula or online modules, or additional training for core faculty who could then serve as palliative care experts, might help advance the palliative care skills of cardiology trainees. 13 Still, ensuring an adequate number of future palliative care providers to meet the clinical demand could be challenging, as previously described. 39 It may be time to train a generation of physicians with expertise in both the palliative and cardiology arenas.
Appropriately, palliative care consultation at the time of left ventricular assist device or heart transplantation referral is an evolving standard of care. 40 All patients with advanced disease, whether they have options for advanced therapies, should have the opportunity to engage in shared decision-making. Addressing this benefit in AHF training programs as well as general cardiology fellowships is important.
A major obstacle to palliative care and hospice referrals that has been reported is the nonlinear trajectory during the last few months of life of patients with advanced cardiovascular disease. 4,41,42 Evidence-based tools that can help prognosticate a patient’s course exist; including these in a general cardiology fellow’s educational curriculum could help to improve our understanding of patient trajectory and utilization of appropriate palliative care resources. 4,42 Although it may be difficult to add another component to an already rigorous training curriculum, tools such as the HF Survival Score, 43 the Zugck 2-variable model, 44 and the Seattle HF model 45 have all shown relative accuracy in predicting death at 1 to 3 years, depending on the model. Incorporating the utilization of these tools into a fellow’s clinical practice, in much the same way we use Thrombolysis in Myocardial Infarction 46 or Global Registry of Acute Coronary Events 47 scores to risk stratify patients with acute coronary syndromes, could help fellows develop the ability to recognize when a referral to palliative care might be warranted. Another approach could be training fellows to screen for triggers that might suggest a role for advanced therapies or for palliative care resources. 48 This could be accomplished through creation of a simple case-based workshop, which has been effective in changing both knowledge and attitudes of trainees in other specialties toward palliative care. 49 Further study should focus on attempts to implement educational programs that may incorporate some of these approaches and measuring fellow readiness for caring for patients with advanced cardiac diseases before and after implementation, as well as on describing the cost-saving effects that such training may have on QOL and on our already burdened health-care economy.
Conclusions
With recent advances in the care of patients with advanced heart disease, and in particular the rapid recent growth in the field of AHF, patients live longer in the last few decades than they had been previously. Although many patients are not candidates for AHF therapies, more patients are post transplant or are on inotropes or mechanical support. 4,50,51 Recognizing that these patients may eventually succumb to their heart disease, and seizing the opportunity to improve their symptom control, will allow for a more holistic approach to care that centers on the patient as opposed to just 1 organ system. Indeed, the time may have come for the development of palliative cardiology as a new subspecialty of cardiovascular medicine. Continued efforts toward improving palliative care education among cardiologists, starting in fellowship, are imperative as we continue to see advancements in the medical therapies for patients with advanced cardiovascular diseases.
Footnotes
Acknowledgments
The authors would like to thank Dr Nunzio Gaglianello for his feedback and input on the survey and on our manuscript. The authors would also like to thank Dr Michael Widlansky for helpful feedback on our manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Medical College of Wisconsin Cardiovascular Division funds.