
Abstract
Purpose:
Although radiation therapy (RT) can provide palliative benefits for patients with metastatic rectal cancer, its role at the end of life remains unclear. The objective of this study was to assess sociodemographic and clinical factors associated with the use of RT during the last 30 days of life and to evaluate yearly time trends in RT utilization among stage IV patients with rectal cancer.
Methods:
The 2004 to 2012 National Cancer DataBase was queried for patients with metastatic rectal cancer who had a documented death during follow-up. A Bayesian multilevel logistic regression model was used to characterize predictive factors and yearly time trends associated with RT use in the last 30 days of life.
Results:
Among 10 431 patients who met inclusion criteria, 345 (3%) received RT during the last 30 days of life. Factors independently associated with RT use included older age, female sex, African American race, nonprivate insurance, higher comorbidity burden, and worse grade. The odds of RT use at the end of life decreased by 28% between 2007 and 2009 (odds ratio [OR] = 0.72, 95% Credible Interval (CI) = 0.58-0.93), but then increased by 16% from 2010 to 2012 (OR = 1.16, 95% CI = 1.13-1.33), relative to 2004 to 2006.
Conclusion:
Radiation therapy use for patients with metastatic rectal cancer is beneficial, and efforts to optimize its appropriate use are important. Several factors associated with RT use during the last 30 days of life included disparities in sociodemographic and clinical subgroups. Research is needed to understand the underlying causes of these inequalities and the role of predictive models in clinical decision-making.
Keywords
Introduction
Stage IV rectal cancer is characterized by distant spread of the primary tumor to surrounding organs such as the liver and is associated with poor survival. 1 –3 Given that a stage IV rectal malignancy is no longer localized, the goals of oncologic care are not of curative intent and instead prioritize pain management, functional status, and psychosocial health among other factors. 4 –6 Radiation therapy (RT) can be used as palliative treatment for patients with metastatic rectal cancer and is effective in reducing the size of the tumor, diminishing pelvic pain, controlling bleeding, and improving the quality of life. 7 –9 Current National Comprehensive Cancer Network practice guidelines recognizes RT as an appropriate treatment option for both resectable and nonresectable stage IV patients with rectal cancer. 10
Despite the promising benefits that palliative RT offers, treatment guidelines do not discuss timing of initiation, even though timing can impact the effectiveness of RT, particularly at the end of life. Radiation therapy is optimal when it is given with enough time for its therapeutic effects to manifest themselves, but treatment may lead to unnecessary health-care utilization and decreased the quality of life if delivered during the end-of-life setting. 11,12 Studies have reported increasing trends in the use of ineffective cancer treatment, particularly in the last 30 days of life. 13 –17 To date, however, no consensus guidelines have been developed to guide clinical decision-making about the appropriate use of RT specifically in the end-of-life setting, likely leading to variation and physician subjectivity in the decision to recommend RT.
Although several studies have attempted to elucidate factors and trends associated with RT use during the end of life, they have been mostly limited to the Medicare population, thus limiting generalizability to younger populations. 18 –23 In addition, these studies have not examined RT use during the end of life specifically for patients with rectal cancer. Given the particular clinical management and natural history of a rectal tumor, factors associated with RT use as well as its prevalence in the end-of-life setting may differ for patients with rectal cancer compared to other malignancies. 24 –26
The objective of this study was to provide a descriptive profile of the national patterns of RT use in the last 30 days of life among stage IV patients with rectal cancer diagnosed between 2004 and 2012. Specifically, we sought to identify factors and yearly time trends associated with the use of RT in the last 30 days of life among patients with rectal cancer.
Methods
Study Population and Data Source
A retrospective cohort study was conducted by selecting patients from the National Cancer DataBase (NCDB). The NCDB is a collaborative program between the Commission on Cancer (CoC) of the American College of Surgeons and the American Cancer Society that collects tumor registry data from approximately 70% of all incident cancer diagnoses treated at 1500 institutions in the United States. 27
Adult patients who were diagnosed with rectal cancer adenocarcinoma, mucinous adenocarcinoma, and signet ring cell carcinoma between 2004 and 2012 were included. The cohort was restricted to clinical stage IV patients with complete data and a documented vital status indicating death (Figure 1). Approximately, one-third of patients with a documented death had at least 1 missing covariate. The most common variable that was missing among those who had at least 1 covariate missing was RT (81%). In order to assess the influence of these missing data patterns, a multivariable analysis was conducted by including a dummy variable indicating whether a patient had any missing data (yes vs no). Results indicated that patients who had missing data had no difference in the odds of receiving RT in the last 30 days of life relative to patients who had complete data (OR = 0.89, 95% credible interval = 0.67-1.27).
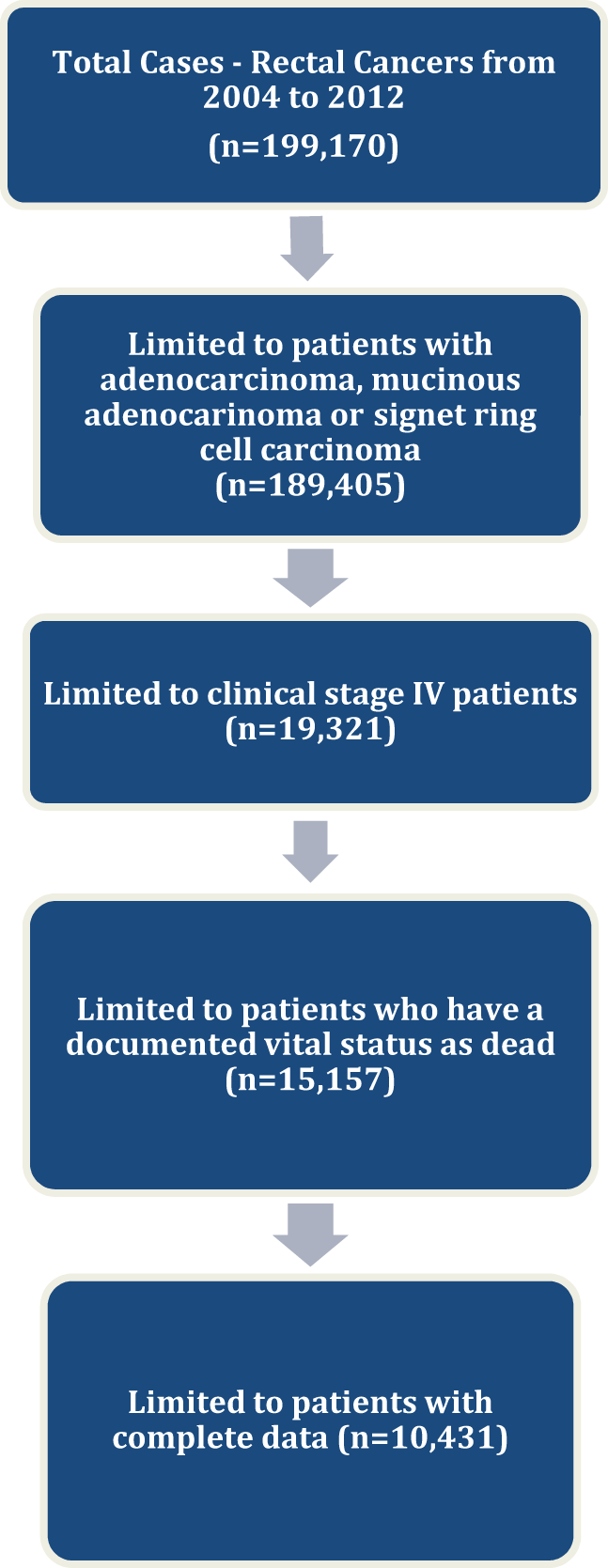
Inclusion diagram.
Definition of RT Use
The primary outcome of this study is RT use in the last 30 days of life (yes/no). The following variables were used to define the outcome: number of days between the date of diagnosis and the date of death (A), number of days between the date of diagnosis and the date of RT initiation (B), and number of days of RT treatment (C). The following formula was used: time from end of RT to death = A − B − C. This continuous variable was converted into a dichotomous variable representing receipt of RT in the 30 days of life. The cutoff of 30 days prior to death was chosen a priori in order to be consistent with prior literature on the end-of-life cancer care. 15 –19,22,23
Patient and Hospital Covariates
Several patient factors were considered using standard NCDB coding. These characteristics included tertiles of age, sex, race/ethnicity, insurance status, education (proportion of adults in zip code who did not graduate high school, divided into quartiles), income (quartiles of median household income in zip code), and a modified version of the Charlson Comorbidity Score, histology, tumor grade, and year of diagnosis (2004-2006, 2007-2009, and 2010-2012).
Hospital characteristics were also considered. Hospital volume was calculated as tertiles of the average annual number of rectal cancer resections. Hospital type and hospital geographic location based on NCDB categories were assessed.
Statistical Analysis
χ2 tests examined differences in RT use in the last 30 days of life across distributions of patient and hospital covariates. Independent multivariable predictors of RT use were subsequently assessed using a Bayesian multilevel logistic regression model that controlled for the unique hospital identifier as a clustering variable. Bayesian models are different than their frequentist/classical counterparts because the beliefs about the uncertainty are specified not only with the available data but also with a prior distribution. Bayesian statistical methods employ “prior” beliefs and combine them with the available data to give “posterior” beliefs, which may be used as the basis for inferential decisions. An inverse Wishart prior for the variances and a normal prior for the fixed effects were specified. Bayesian multilevel logistic regression model estimated the log odds associated with each risk factor using Markov Chain Monte Carlo simulation and Gibbs sampling. We used the deviance information criterion to assess model fit and plots of the posterior distributions to diagnose convergence of the model. Furthermore, due to their nature, Bayesian models do not generate P values and estimate credible intervals that are analogous to confidence intervals.
Previous literature has examined different cut points to determine the end-of-life RT utilization, thus, we conducted separate sensitivity analyses with the outcome of RT use, 15 and 45 days prior to death. 12,18 We repeated the above analyses for these separate cut points.
Results
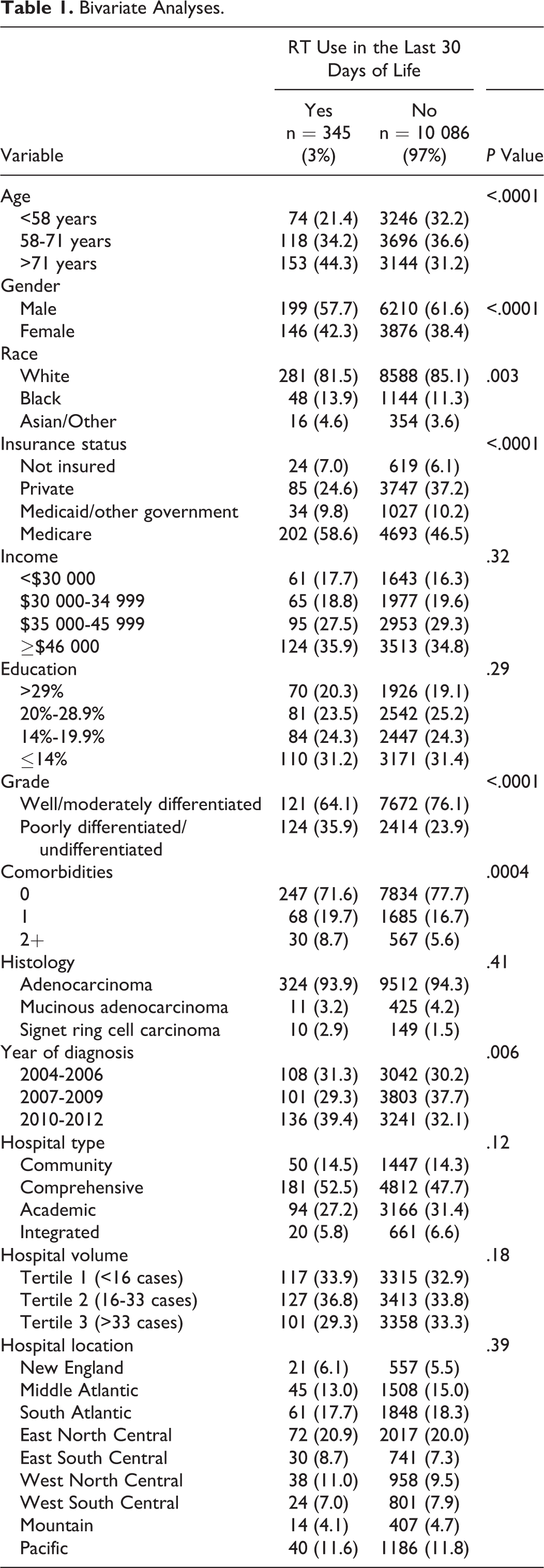
A total of 10 431 clinical stage IV patients with rectal cancer treated at 1203 CoC-accredited hospitals met inclusion criteria. Approximately 3% of patients received RT in the last 30 days of life, and the average age in the cohort was 65 years. In addition, 39% of patients were female, and 94% carried some type of health insurance. The median follow-up time from diagnosis to death was 13.5 months. The average and median percentage of remaining life spent while on RT were 12% and 8%, respectively. Table 1 reports the distributions of patient and hospital characteristics stratified by whether or not patients received RT in the last 30 days of life.
Bivariate Analyses.
Independent Predictors of RT Use in the Last 30 Days of Life
After simultaneously controlling for all covariates, as well as clustering by hospitals, several characteristics remained independent predictors of RT use in the last 30 days of life (Table 2). Older and female patients were more likely than younger and male patients to receive RT in the last 30 days of life (age >71 vs age <58, OR = 1.88, 95% Credible Interval [CI] = 1.76-2.09; female, OR = 1.15, 95% CI = 1.01-1.34). Patients with poorly differentiated or undifferentiated tumors had an almost 50% increase in the odds of using RT in the last 30 days of life relative to patients who had well-differentiated or moderately differentiated tumors (OR = 1.45, 95% CI = 1.19-1.89). Insurance status was an independent predictor of RT use in the last 30 days of life, as patients without any insurance, Medicare/other government insurance and Medicaid insurance all had increased odds of using RT in the last 30 days of life relative to patients with private insurance. Additionally, there were racial disparities reflected by a 1.6-fold difference in the odds of RT use in the last 30 days of life for African American patients relative to white patients (OR = 1.62, 95% CI = 1.33-1.98). Further, higher comorbidity burden was associated with increased odds of receiving RT in the last 30 days of life (2+ vs 0, OR = 1.52, 95% CI = 1.15-2.02).
Multivariable Analysis of Factors Associated With RT Use in the Last 30 Days of Life.
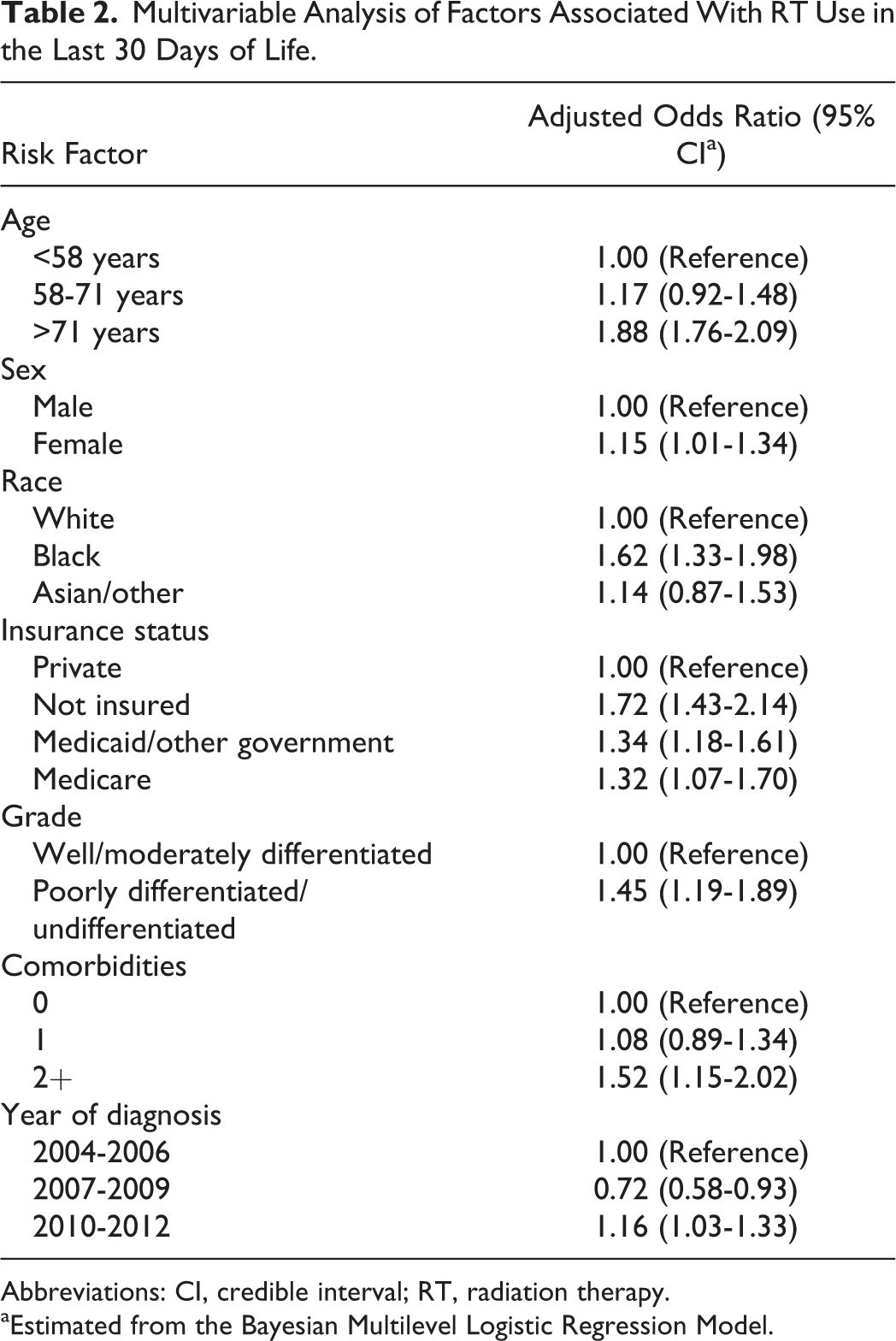
Abbreviations: CI, credible interval; RT, radiation therapy.
aEstimated from the Bayesian Multilevel Logistic Regression Model.
Yearly Time Trend Analysis
The use of RT in the last 30 days of life changed over time. Figure 2 illustrates the proportion of patients with rectal cancer who received RT in the last 30 days of life for each year between 2004 and 2012. In 2007, the percentage of patients with metastatic rectal cancer who received RT in the last 30 days of life decreased by 25% relative to 2004 (3.2% vs 2.4%). By the end of the study period in 2012, RT utilization increased to 4.4%. These patterns were reflected and maintained in multivariable analysis (Table 2). Patients diagnosed in the years 2007 to 2009 had a 28% decrease in the odds of RT use in the last 30 days of life relative to patients diagnosed in 2004 to 2006. Alternatively, patients diagnosed in the years 2010 to 2012 had a 16% increase in the odds of RT use during the last 30 days of life relative to patients diagnosed in 2004 to 2006.
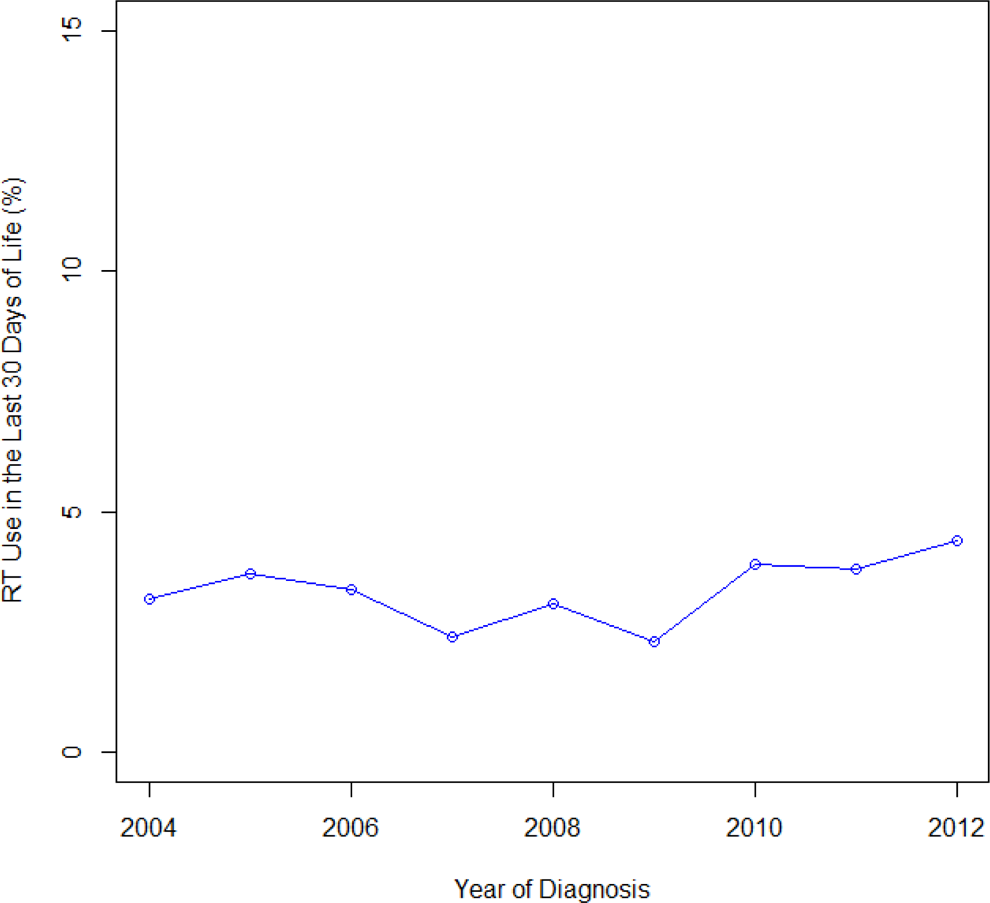
Yearly radiation therapy (RT) use during the last 30 days of life.
Sensitivity Analyses
The proportion of patients receiving RT in the last 15 and 45 days of life was estimated to be 2.1% and 4.5%, respectively. After repeating analyses for these 2 different cut points, results were similar, both in bivariate or multivariable analyses as compared to the primary analysis.
Discussion
Radiation therapy can be an effective treatment option for patients with metastatic rectal cancer being managed in a palliative care setting. Effective treatment applied to an a priori unfavorable cohort of patients may be erroneously interpreted as lacking benefit. The goals of this study were to examine factors and yearly time trends associated with RT utilization in the last 30 days of life among stage IV patients with rectal cancer. We report discrepancies in the use of RT in the last 30 days in life across several sociodemographic subgroups, clinical factors, and time periods.
Previous studies have examined factors associated with RT use in the end of life for patients with rectal cancer. 18 –23 However, most of these studies evaluated these associations using cohorts consisting of several malignancies including colorectal, lung, breast, and prostate, thus limiting knowledge about cancer-specific trends. This is an important limitation in the current literature since the clinical management of cancer is heterogeneous across disease sites. 24 –26 Differences in clinical management of these malignancies imply differences in the team of providers that are consulted, which can influence RT use in the end-of-life setting. For example, there exist large differences in the frequency of radiation oncologist consultations across several malignancies thus likely leading to different patterns in futile use of RT at the end of life. 28,29
The first objective of this nationwide hospital-based study was to evaluate independent factors associated with RT utilization during the last 30 days of life among patients with metastatic rectal cancer. Independent sociodemographic and clinical predictors of RT use in the last 30 days of life included older age, female sex, African American race, nonprivate insurance, higher comorbidity burden, and worse grade. Although results for some of these factors mirror previous reports, the patterns for age and sex are quite different to studies currently in the literature. Specifically, all previous studies of RT use at the end of life have reported older age to be associated with decreased likelihood of RT utilization, yet our study reports that patients aged greater than 71 years had an 88% increase in the odds of RT use relative to patients aged less than 58 years. This may likely reflect the fact that most of the previous studies combined different malignancies into 1 cohort, of which a very small percentage had a rectal malignancy. Since these studies did not assess effect modification by cancer type, they may have not captured the heterogeneous effects of age on RT use across organ systems. We report that older patients with rectal cancer are at higher risk of receiving ineffective treatment at the end of life.
Our study also reports sex discrepancies with women being more likely to receive RT in the last 30 days of life, unlike most studies that have reported no such association. Although the mechanisms underlying this observation are not clear, it is likely that this reflects unnecessary gender disparities in the end-of-life care setting. Further, most previous studies assessing RT use in the end-of-life setting have been limited to Medicare cohorts, and thus there is limited data on the effects of insurance type. We observed that patients with Medicaid, Medicare, and those without any form of insurance all had increased odds of aggressive RT use relative to patients with private insurance. This may reflect the quality of health-care coverage and benefits (such as hospice care) that are provided by different insurance plans. Finally, we report that patients with high comorbidity burden had a higher chance of receiving RT in the last 30 days of life, and because higher comorbidity burden is associated with worse survival, it may not be prudent to use RT for patients with significant comorbid illnesses. 30
The second goal of this study was to assess yearly time trends in the use of RT in the last 30 days of life. The frequency of RT utilization during the end of life changed yearly and resulted in decreased utilization during the years 2007 to 2009, followed by increased utilization in the subsequent 2010 to 2012 time period. These trends were independent of all other factors considered. Reasons for this finding may include an unclear consensus about the appropriate timing of RT utilization as well as variation in practice patterns. Given that no hospital factors were associated with RT use during the last 30 days of life, it is possible that this variation reflects subjective decision-making on the part of providers as opposed to systematic pressures from the institution.
The findings from this study need to be interpreted within the context of the study’s limitations. First, palliative care is not captured in NCDB and thus, it is likely that a subset of these patients were treated with RT for curative intent. Second, NCDB does not collect important information such as the cause of death or reasons behind treatments given. Finally, this study is retrospective and observational in nature and the possibility of selection bias cannot be ruled out. For example, while NCDB collects data on approximately 70% of all cancer cases, they only include hospitals that have a CoC designation and thus the frequency and patterns in RT utilization may be different at non-CoC centers.
Notwithstanding these limitations, this is the largest study to date examining RT utilization in the last 30 days of life specifically for rectal cancer. The study takes advantage of a heterogeneous population across the entire United States, thus making the results generalizable to a large sample of patients. Finally, this study employed Bayesian multilevel modeling, which allows for clustering of patients within hospitals to be appropriately controlled for.
Although RT is beneficial when delivered under appropriate palliative care settings, the role of RT for patients with rectal cancer near the end of life needs to be clarified. Delivery of RT in the last 30 days of life is a concern because it can undermine patient quality of life and lead to economic burdens on the health-care system and also undermine the effective use of RT. This study reports modest, but important disparities in RT utilization at the end of life across several sociodemographic and clinical factors. Also, the rate of RT utilization in this cohort was substantially lower than for other malignancies, which may likely be explained by the fact that many patients with metastatic rectal cancer receive RT as a primary treatment. Taken together, these observations suggest that RT is an important treatment modality for stage IV rectal cancer and its role needs can be further optimized, in particular as a palliative treatment option. The balance between palliation and the potential dangers in delivering RT to an already unfavorable group, those in the last 30 days of life, should to be considered. Future research necessitates the investigation of incorporating predictive models into clinical decision-making as well as the mechanisms by which these differences arise.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.