
Abstract
Introduction:
End-of-life and palliative care are important aspects of trauma care and are not well defined. This analysis evaluates the racial and socioeconomic disparities in terms of utilization of hospice services for critically ill trauma patients.
Methods:
Trauma patients ≥15 years old from 2012 to 2015 were queried from the National Trauma Databank. Chi-square and multivariate logistic regression analyses for disposition to hospice were performed after controlling for age, gender, comorbidities, injury severity, insurance, race, and ethnicity. Negative binomial regression analysis with margins for length of stay (LOS) was calculated for all patients discharged to hospice.
Results:
Chi-square analysis of 2 966 444 patient’s transition to hospice found patients with cardiac disease, bleeding and psychiatric disorders, chemotherapy, cancer, diabetes, cirrhosis, respiratory disease, renal failure, cirrhosis, and cerebrovascular accident (CVA) affected transfer (P < .0001). Logistic regression analysis after controlling for covariates showed uninsured patients were discharged to hospice significantly less than insured patients (odds ratio [OR]: 0.71; P < .0001). Asian, African American, and Hispanic patients all received less hospice care than Caucasian patients (OR: 0.65, 0.60, 0.73; P < .0001). Negative binomial regression analysis with margins for LOS showed Medicare patients were transferred to hospice 1.2 days sooner than insured patients while uninsured patients remained in the hospital 1.6 days longer (P < .001). When compare to Caucasians, African Americans patients stayed 3.7 days longer in the hospital and Hispanics 2.4 days longer prior to transfer to hospice (P < .0001). In all patients with polytrauma, African Americans stayed 4.9 days longer and Hispanics 2.3 days longer as compared to Caucasians (P < .0001).
Conclusions:
Race and ethnicity are independent predictors of a trauma patient’s transition to hospice care and significantly affect LOS. Our data demonstrate prominent racial and socioeconomic disparities exist, with uninsured and minority patients being less likely to receive hospice services and having a delay in transition to hospice care when compared to their insured Caucasian counterparts.
Introduction
Many trauma studies focus on length of stay (LOS), morbidity, and mortality leaving transition to hospice as an understudied outcome. Various models and screening tools exist to identify those who would benefit from palliative and hospice services, but few focus specifically on the trauma population. 1 –5 By 2050, 40% of the trauma population will be greater than 65 years old and therefore a shift of focus on caring for the elderly trauma patient is necessary. 6 –8 Practitioners should understand these barriers and focus on improving end-of-life care for the critically ill trauma population.
Hospice improves quality of care, lowers costs, decreases rates of hospital service use, and lowers the number of in-hospital deaths. 9 Studies on the nontrauma populations show that Hispanics and African Americans with terminal illness typically desire aggressive life-sustaining treatment as compared to their Caucasian counterparts. 10 –12 Some studies have found that African Americans use end-of-life services less often, while other researchers have concluded that hospital-based systems and/or referral patterns are the cause for this disparity. 13 –16
Socioeconomic, racial, and ethnic disparities exist throughout the health-care system. 17,18 The current literature demonstrates that race and insurance status play a role in outcomes and care decisions in the trauma population. 19 –22 The aim of this analysis is to better define racial and socioeconomic disparities that exist for trauma patients with regard to access to hospice and end-of-life care.
Methods
A retrospective analysis was performed of all adult trauma patients (age 15 and older) who presented to trauma centers participating in the National Trauma Data Bank (NTDB) between 2012 and 2015. The NTDB is a deidentified trauma database through the American College of Surgeons that trauma centers across the country voluntarily contribute to. All patients with unknown disposition were excluded from this analysis.
The primary outcome for this study was disposition to hospice. The secondary outcome was hospital LOS. Factors associated with disposition were evaluated using the subset of patients discharged to hospice care. These patient factors included age, gender, medical comorbidities, prior need for inpatient care, race, and ethnicity (African American, Asian, Caucasian, Native American, or Hispanic). The analysis also investigated insurance status (uninsured, private insurance, Medicaid, Medicare, government insurance, and motor-vehicle insurance) as a potential barrier to hospice care. After creating a binomial variable for comorbidities, a chi-square analysis was conducted for comorbidities (Chronic obstructive pulmonary disease [COPD], bleeding disorder, psychiatric illness, current need for chemotherapy or disseminated cancer, diabetes, cirrhosis, esophageal varices, hypertension, respiratory disease, history of myocardial infarction [MI], angina within 30 days, congestive heart failure [CHF], renal failure, steroid use, peripheral vascular disease [PVD], and history of stroke), as well as prior need for dependent health care to determine whether they significantly affected transfer to hospice.
In medicine, dying patients are considered to have the same severity of illness, but this is not necessarily true in the trauma population. 23 Injury severity significantly influenced disposition to hospice and therefore was used as a control in this analysis. Additionally, multivariate logistic regression models with odds ratios (ORs) for disposition to hospice were created controlling for patient age, gender, significant univariate medical comorbidities, injury severity score (ISS), insurance status, race, and ethnicity for all patients. A subset analysis was done for patients with polytrauma, defined as an ISS greater than 15. Injury severity score is a verified method for calculating the severity of injury in trauma patients and correlates statically with mortality. 24 Injury severity score is a combination of a patient’s 3 most severe injuries defined by each injury’s Abbreviated Injury Scale (AIS) score. The AIS scale ranges from 1 to 6. Score 1 is minor injury, 3 is serious, and 6 is untreatable leading to mortality. To calculate the AIS, 6 regions of the body (head and neck, face, chest, abdomen or pelvis, and external causes of trauma) are used.
To evaluate hospital LOS, patients discharged to hospice were analyzed using a negative binomial regression with margins commands. This was done because the data failed to reject the null hypothesis that LOS suffers from overdispersion (α 0.54, 0.57). This analysis used the same covariates above for those patients who were discharged to hospice care. Secondary analysis looked at total hospital LOS for patients with polytrauma. Significance was defined as P ≤ .05. StataCorp 2015 was the software used for the analysis. Stata Statistical Software: Release 14. College Station, Texas: StataCorp LP. The data is reported as mean (standard deviation).
Results
In total, 2 966 444 patients were included in the analysis, of which 23 612 were discharged to hospice. Patients discharged to hospice were 73 (16) years old, 52% female, and 89% Caucasian. The most common comorbidity was hypertension (57%). The mean ISS for the hospice population was 13 (8.5) and 9874 patients had an ISS greater than 15. The majority of patients had Medicare insurance (71%), followed by private, Medicaid, and self-pay (Table 1). Prior to admission due to trauma, 14% of patients had history of health-care dependence.
Demographics by Insurance Status of Patients Discharged to Hospice.
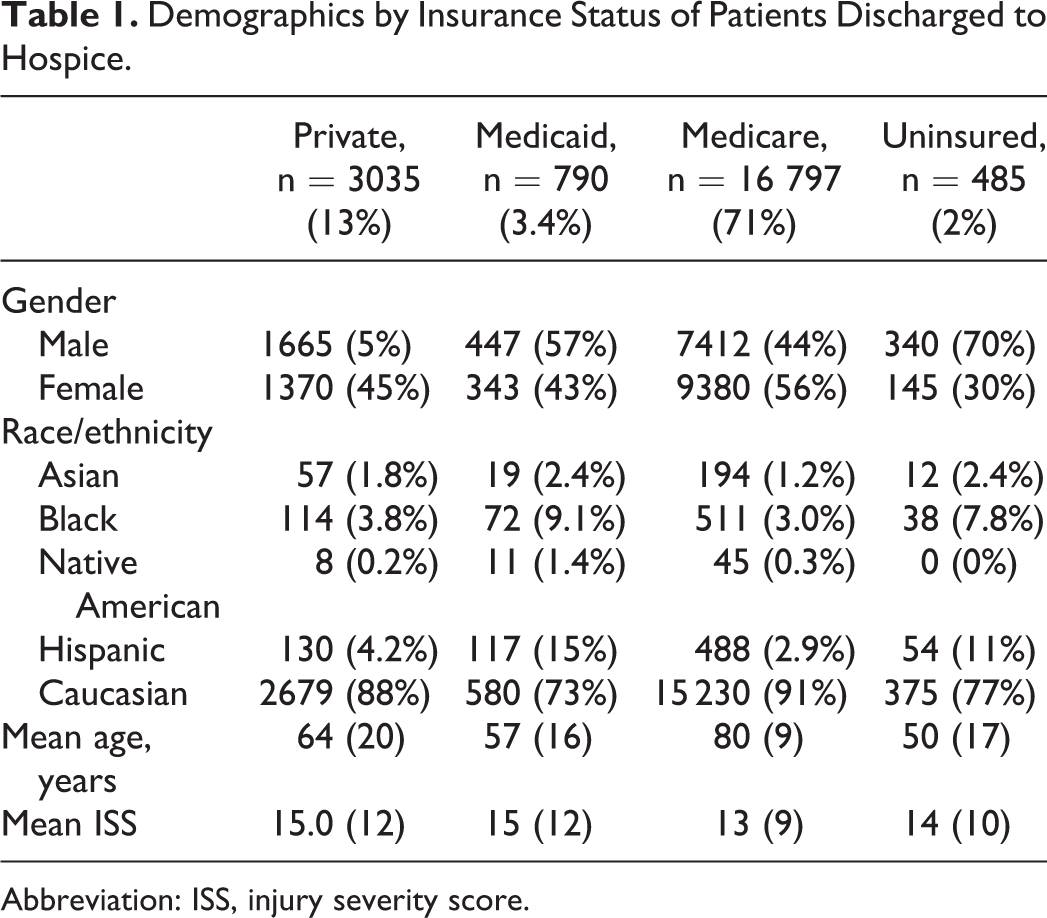
Abbreviation: ISS, injury severity score.
Variables that independently impacted disposition to hospice included COPD, CHF, bleeding disorder, psychiatric illness, current need for chemotherapy or disseminated cancer, diabetes, cirrhosis, hypertension, respiratory disease, MI, PVD, renal failure, esophageal varices, cirrhosis, and cerebrovascular accident (CVA) (P < .0001). A multivariate logistic regression controlling for significant covariates demonstrated that uninsured patients were discharged to hospice significantly less than insured patients (OR, 0.71; P < .0001, Table 2). Furthermore, Asian, African Americans, and Hispanic patients were less likely to receive hospice care than Caucasians (P < .0001).
Multivariate Logistic Regression Model—Discharge to Hospice.
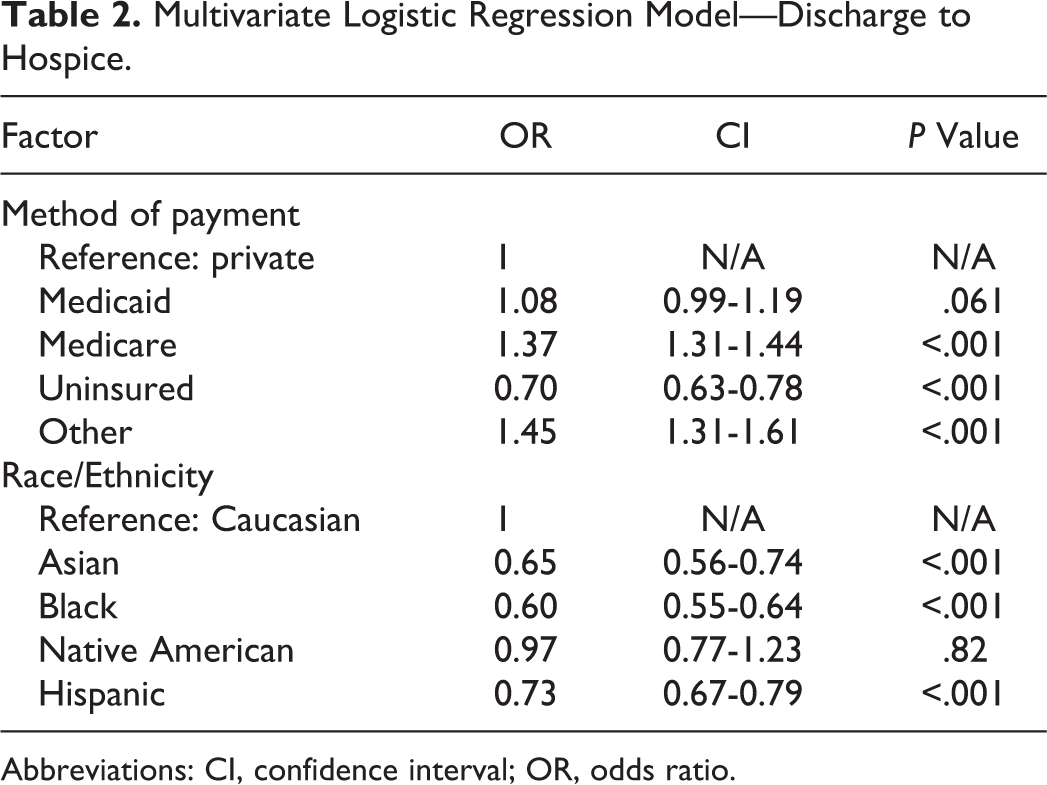
Abbreviations: CI, confidence interval; OR, odds ratio.
Additionally, socioeconomic status affected total hospital LOS. An analysis of 23 612 patients revealed that Medicare patients were transferred to hospice 1.2 days sooner than privately insured patients (P < .001), and uninsured patients remained in the hospital 1.6 days longer than privately insured patients (P < .001). When evaluating racial disparities, African American patients who were discharged to hospice stayed in the hospital 3.7 days longer and Hispanic patients stayed 2.4 days longer than Caucasian patients (P < .0001). A secondary analysis for the more severely injured trauma patients (ISS > 15) showed that African Americans stayed inpatient 4.9 days longer and Hispanics 2.3 days longer than their equivalent Caucasians counterparts (P < .0001).
Discussion
We set out to identify racial and socioeconomic disparities that exist in trauma patients’ access to hospice care. This is the largest analysis of trauma patients’ disposition to hospice. Furthermore, it is the first nationwide analysis defining socioeconomic disparities in the trauma population with regard to hospice transfer. This analysis shows that despite efforts to promote and improve access for end-of-life referrals, enormous racial disparities are prevalent in the trauma system separate from significant socioeconomic inequalities. 25,26 Additionally, this analysis demonstrates that for those uninsured and minority population who do receive hospice care, there is a delay in transfer to hospice when compared to their insured, Caucasian counterparts.
Patient and surrogate decision maker preference likely plays an important role in the choices surrounding transfer to hospice. A previously published study looking at patient preferences with regard to end-of-life decisions found that African Americans chose life-sustaining measures more than Caucasians and men more often than women. 10 Unfortunately, this study did not control for insurance status or income. In fact, the authors theorized that socioeconomic disparities could have been the driver for differences in end-of-life decisions, rather than race. In our analysis, socioeconomic status was controlled for and the same disparities exist. African Americans go to hospice less and if they do go, they are discharged following a longer hospital course when compared to matched Caucasian patients.
Studies of nursing home patients’ opinions on end-of-life cares have shown racial disparities, but studies within the trauma population specifically have not been performed. 11,27 It has been hypothesized that African Americans utilize end-of-life care less because they do not trust the health-care system and fear exploitation. 27 Additionally, a study evaluating the decision to withdraw mechanical ventilation in the intensive care unit showed that the health-care delivery system did not have a significant impact on the decision to withdraw, but that African American patients who underwent surgical intervention were less likely to transition to comfort care. 12 Contrary to this, a project exploring end-of-life barriers in lower income, African Americans, and Hispanics found that when focus groups were conducted, they were highly receptive to care that would provide relief for patients. This study found that improving awareness of hospice services would increase utilization in minority populations. 28 These analyses combined with the knowledge that minority trauma patients are transferred to hospice less often than Caucasians portend to the success of workgroups developed for minority trauma populations.
At our institution, we conduct multidisciplinary family meetings to discuss goals of care for all critical care trauma patients within 72 hours of admission. These meetings include participation by social workers, nurse navigators, case managers, nurse practitioners with a focus on palliative care, and the attending surgeon. The goal of these family meetings is to focus on the patient, caregiver, and family perceptions of end-of-life care to determine whether perceptions change once these caregivers and patients have a better understanding of hospice care services. We use a best-case/worst-case model to discuss the clinical picture and aid in family decision-making. 29
Limitations of this study include lack of long-term follow-up to determine whether some of the patients who were discharged to other facilities eventually ended up in hospice care as well as the inability to evaluate patients who were discharged to hospice after 30 days. Additionally, there is no ability to see referral patterns to determine whether the bias is staff referrals or patient preference. Furthermore, this data set, although robust, is voluntary and does not cover all hospitals in the trauma system creating some bias. Finally, this is a retrospective study so it cannot draw causal conclusions.
Conclusion
Although trauma surgeons often work tirelessly to save critically injured patients, they also understand the importance of addressing hospice care needs in order to allow those patients who cannot have meaningful recovery from their trauma the best quality of life with the time remaining. This analysis shows prominent racial and socioeconomic disparities in end-of-life trauma care. Once the trauma community better understands why these disparities exist, practitioners can develop tools developed to improve access to hospice care and ensure all trauma patients regardless of socioeconomic status have access to end-of-life services.
Footnotes
Authors’ Note
This research was conducted under the guidance of Suresh Agarwal, primarily by Krista Haines. Tiffany Zens, Scott Turner, and Charles Hillard made significant contribution to data collection and analysis. Hee Soo Jung provided meaningful guidance with regard to methodological approach, data analysis, and manuscript writing as well as redrafting and correcting the manuscript. This research was presented at the Society of Asian Academic Surgeons 2017.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.