
Abstract
Objectives:
We present a pilot study exploring the effects of a brief, 30-minute educational intervention targeting resident communication surrounding dying in the intensive care unit (ICU). We sought to determine whether simulation or didactic educational interventions improved resident-reported comfort, preparation, and skill acquisition. We also sought to identify resident barriers to using the word “dying.”
Methods:
In this mixed-methods prospective study, second- and third-year medical residents were randomized to participate in a simulation-based communication training or a didactic session. Residents completed a pre–post survey after the sessions evaluating the sessions and reflecting on their use of the word “dying” in family meetings.
Results:
Forty-five residents participated in the study. Residents reported increases in comfort (Mean [M]-pre = 3.3 [standard deviation: 0.6], M-post = 3.7 [0.7]; P < .01, Cohen d = 0.75) and preparation (M-pre = 3.4 [0.7], M-post = 3.9 [0.6]; P < .01, d = 1.07) using the word “dying” after both the simulation and didactic versions. Residents randomized to the simulation reported they were more likely to have learned new skills as compared to residents in the didactic (M-simulation = 2.2 [0.4], M-didactic = 1.9 [0.3]; P = .015, d = 0.80). They estimated that they used the word “dying” in 50% of their end-of-life (EOL) conversations and identified uncertain prognosis as the main barrier to explicitly stating the word “dying.”
Conclusion:
A 30-minute educational intervention improves internal medicine residents’ self-reported comfort and preparation in talking about death and dying in the ICU. Residents in simulation-based training were more likely to report they learned new skills as compared to the didactic session. Residents report multiple barriers to using the word “dying” EOL conversations.
Keywords
Introduction
High-quality communication during end-of-life (EOL) discussions is vital in the intensive care unit (ICU), where one-fifth of Americans die. 1 End-of-life conversations are associated with less aggressive medical care near death, reduced costs, improved quality of dying, and reduction in major depression among bereaved family caregivers. 2,3 Despite the well-established benefits of effective EOL communication, one-third of patients and their surrogates report dissatisfaction with communication in the ICU, and one-half of patients and their surrogates report not understanding their diagnosis or prognosis. 4 A recent mixed-methods analysis of family members’ experience with EOL discussions found that half of respondents wanted more direct information about outcomes of care, specifically that the patient was “sick enough to die.” 5
Barriers to improving this significant doctor–patient/family interaction may include time and resource constraints in training programs as well as resident physician discomfort. Physicians and resident trainees report they do not receive adequate training in EOL communication, leading them to feel both uncomfortable and unprepared to have these conversations. 6 -8 Various educational interventions involving simulation, 9 -11 skills workshops, 12,13 and traditional didactics 14,15 have been shown to improve communication skills, but there is a lack of data evaluating the most effective way to teach EOL communication.
In this study, our first objective was to investigate the most effective strategies for teaching a specific EOL communication skill. We performed a pre–post analysis of a novel EOL communication curriculum for internal medicine residents. We sought to (1) determine whether a brief, 30-minute targeted educational intervention improved resident comfort and preparation in talking about death and dying in the ICU, and (2) evaluate 2 different forms of the communication training—simulation versus didactic—with regard to resident self-report of comfort, preparation, and skill acquisition.
Our second objective was to explore internal medicine residents’ reported use of the word “dying” in EOL conversations in the ICU. In particular, we sought to determine whether a discrepancy existed between “resident-perceived prognosis” (imminent death) and “patient-conveyed prognosis” (use or nonuse of the word “dying”). We then attempted to identify any themes and barriers underlying this disconnect among residents at our institution.
Methods
To accomplish our first objective, second- and third-year internal medicine residents at Beth Israel Deaconess Medical Center rotating in the ICU were randomized to participate in either a simulation-based educational session or a didactic-based educational session (see Figure 1). The sessions occurred once during their rotation during a scheduled ICU didactic period from 8:00
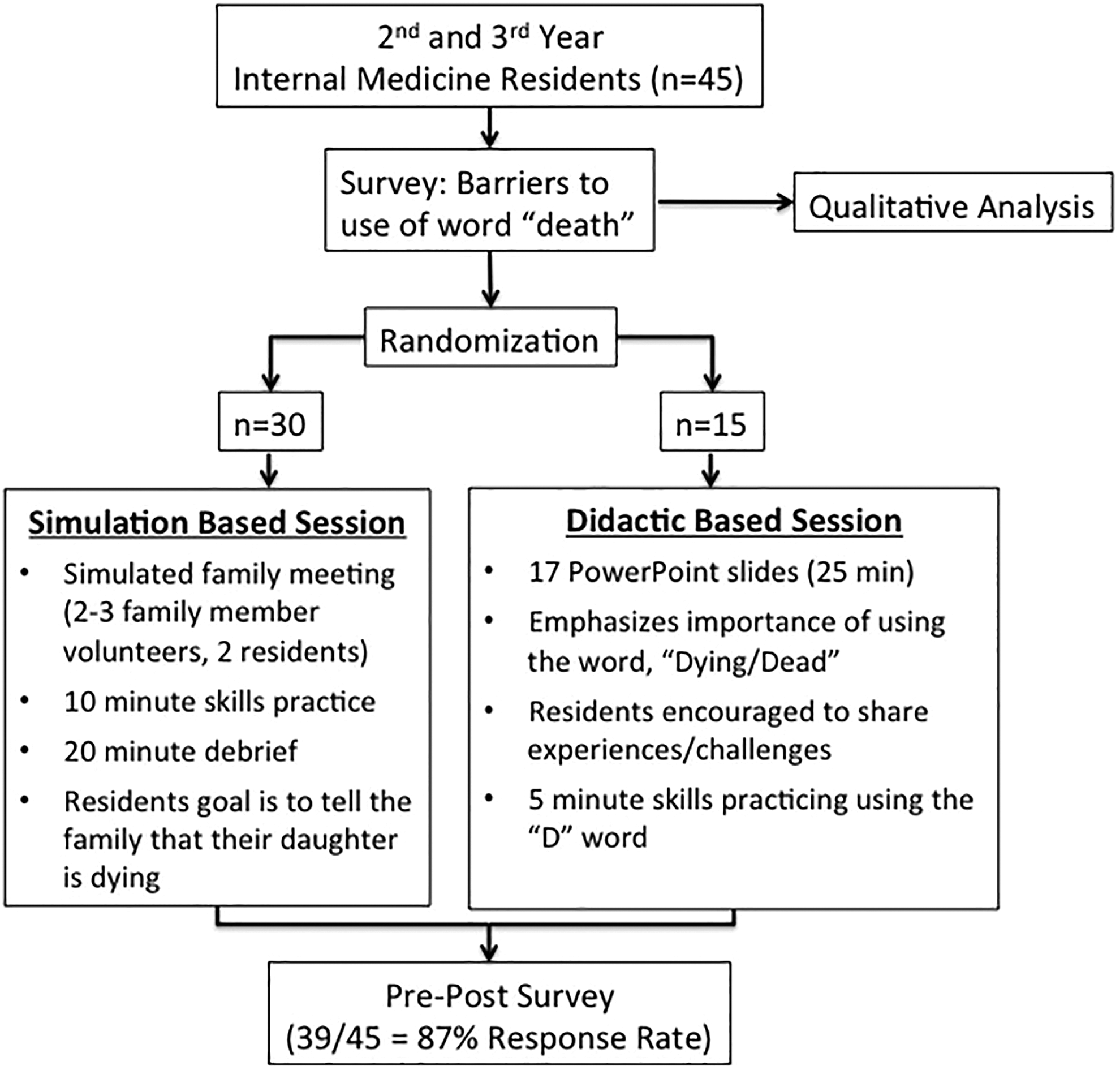
Study population, randomization methods, and educational session descriptions.
Both the simulation and didactic sessions were led by a clinical faculty instructor with experience in critical care and EOL education. Residents completed a retrospective pre–post training survey at the conclusion of each educational session in which they self-assessed their perceived skills prior to and immediately after the course at a single point in time.
In the facilitated simulation session, faculty briefly introduced the session. Two residents then led the simulated family meetings, which had an average duration of 10 minutes. After the simulation, the faculty facilitated a 20-minute debriefing. The debriefing was structured using a method of reflection and inquiry which promoted curiosity for understanding the drivers of resident behaviors related to discussing dying. Faculty ensured psychological safety by clarifying expectations and rationale for the experience. Family members were played by patient and family member volunteers, all of whom were veteran communication volunteers, trained on the case, objectives of the session, and giving feedback.
The didactic session consisted of a 17-slide PowerPoint (Version 14.7.1 Microsoft) presentation during which residents were encouraged to share their experiences, most importantly their challenges with telling family members that a loved one was dying. For the last 5 minutes, residents formed pairs and practiced the skill of telling a family member their loved one was dying, using the word “dying.”
To account for instructor effect, 6 different instructors facilitated the debriefing and presented the didactic session. One of the creators of the curriculum (M.M.H.) trained these instructors. Additionally, authors (D.C.M. and A.M.S.) observed sessions to ensure that content delivery was similar across instructors.
Statistical analyses were completed using JMP Pro Version 12, SAS Institute Inc, Cary, North Carolina, 1989 to 2012. As our groups each had greater than 10 observations and the data were nearly normally distributed, we used a parametric analysis with a 2-tailed independent samples t test assuming unequal variance. By convention, we assumed a P value of <.05 to represent statistical significance. Effect sizes (Cohen d) were calculated based on the JMP software guidelines as the difference in means divided by the product of the standard error and the square root of the number of participants. A Cohen d value between 0.0 and 0.3 was considered to represent a small effect size, 0.3 to 0.6 a moderate effect size, and >0.6 a large effect size. 16
To accomplish our second objective, residents retrospectively estimated the number of times in residency that they communicated to patients or patient surrogates that the patient was imminently dying. They were then asked to estimate the number of times they specifically used the word “dying” in their conversations. Residents were then asked to reflect and identify barriers or difficulties they experienced in telling a patient or patient surrogates that the patient was dying in free-response format.
Resident responses were coded for specific barriers to using the word death in EOL conversations and common themes were identified. Using a framework analytic method, 17 2 independent coders (D.C.M. and M.M.H.) created themes and codes. Trustworthiness was ensured by having 2 researchers, a resident and an ICU attending, ingrained in the culture create the questions and analyze them. 18 The researchers met regularly and openly discussed their assumptions and biases and additionally discussed their themes and codes with a nonphysician (A.M.S.). 18 Refined codes were independently applied to the initial resident-identified barriers using the web-based analytics program, Dedoose (Version 7). Inter-rater reliability was assessed using a pooled-Cohen κ.
Both portions of the study were reviewed by the Committee on Clinical Investigations at Beth Israel Deaconess Medical Center and determined to be an educational quality improvement project, not meeting criteria for human participants research.
Results
In the first portion of our study, aimed to investigate effective strategies for teaching a specific EOL communication skill, a total of 45 seconds and third-year internal medicine residents participated. It was not our objective to give residents more certainty about prognosis. Rather, the education emphasized using direct language (such as “dying”) in the face of an uncertain prognosis. Thirty-nine (87%) residents completed the survey. Twenty-one of the 39 respondents were second-year residents and 18 were third-year residents. There was no meaningful difference between the 2 groups in average postgraduate training year (simulation Post-Graduate-Year (PGY) avg = 2.5, didactic PGY avg = 2.4) or exposure to prior communication training at our institution. The prior clinical and educational training between the groups was similar as both groups were drawn from the same residency program.
In aggregate, following each of the 30-minute sessions, residents reported increased comfort using the word “dying” after the sessions. The mean preintervention score on a 5-point Likert scale was 3.3 (0.6) and improved to 3.7 (0.7) postintervention (P < .01; d = 0.75). Residents also reported they were more prepared to use the word “dying” after the sessions (P < .01; d = 1.07). Although residents in both the simulation and didactic groups reported significantly improved comfort and preparation following the sessions, there was no statistically significant difference between the simulation and the didactic in self-reported comfort-post (3.8 vs 3.5; P = .12) or preparation-post training (3.9 vs 3.9; P = .46; see Figure 2).
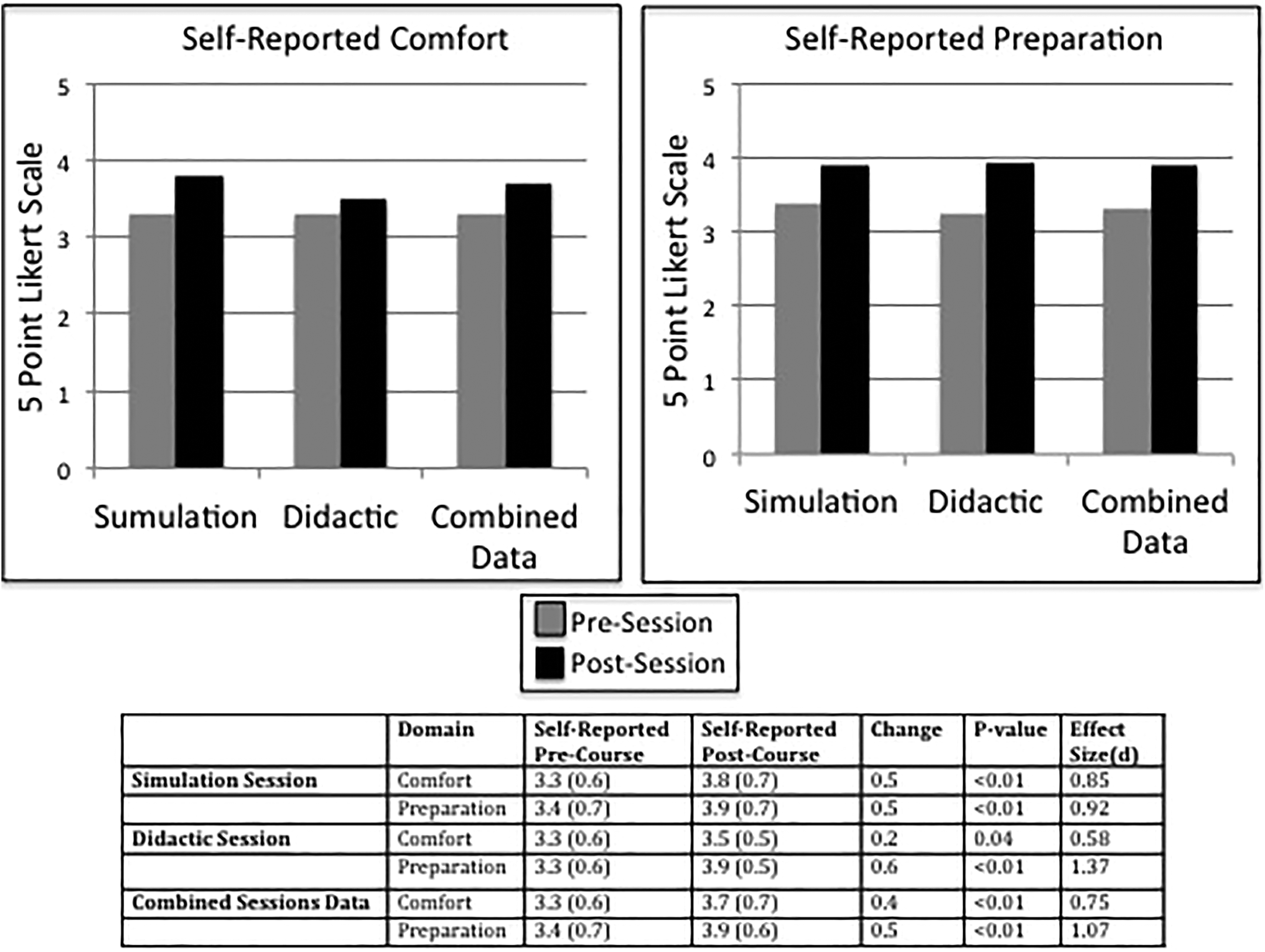
Self-reported resident comfort and preparation before and after the 2 versions of the educational interventions.
Residents randomized to the simulation session reported that they were more likely to have learned new skills compared to residents who underwent the didactic session on a 3-point Likert Scale (Msimulation = 2.2 [0.4], Mdidactic = 1.9 [0.3]; P = .015, d = 0.80; see Figure 3).
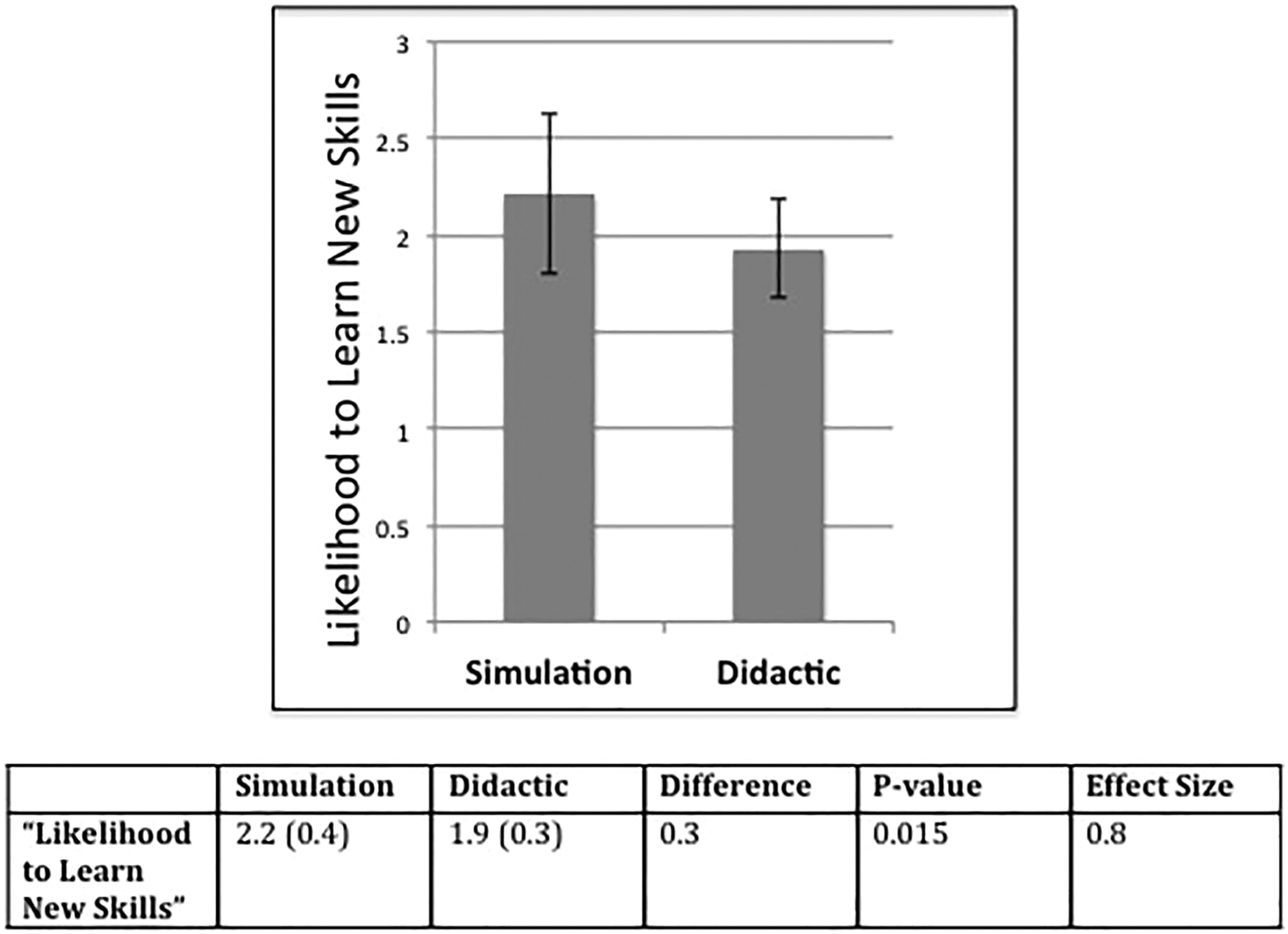
Likelihood to learn new skills following the simulation-based educational session compared to the didactic-based educational session.
Feedback on both interventions was positive. Residents who participated in the didactic session often suggested that the material may be better taught through simulation.
Thirty-eight (21 PGY-2, 17 PGY-3; 84%) of 45 residents completed the second, qualitative portion of the survey. On average, residents recalled having 8 (standard deviation: 1.6) conversations with patients or patient surrogates in which they discussed the resident’s perceived prognosis of imminent death. Of those conversations, residents estimated that they specifically used the word “dying” 50% of the time.
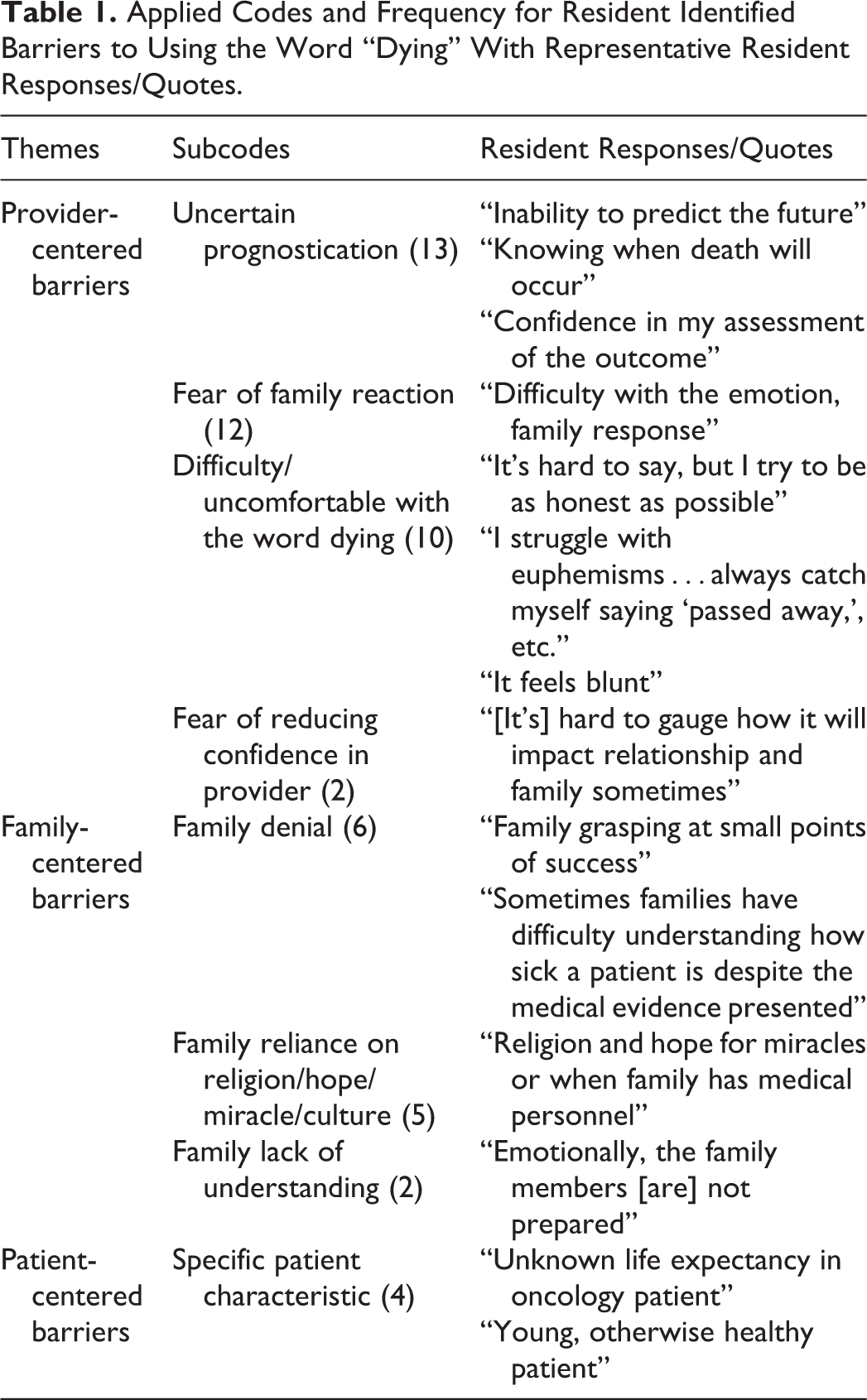
In the qualitative analysis of the resident barriers to using the word “dying,” we identified 3 specific themes: patient-centered barriers, family-centered barriers, and provider-centered barriers. These 3 themes were further subcoded into 8 resident-identified barriers listed in descending order of frequency of code application: uncertain prognostication (13), fear of family reaction (12), discomfort with the word “dying” (10), family denial (6), family reliance on religion/hope/miracle/culture (5), specific patient characteristic such as young age (4), family lack of understanding (2), and fear of reducing family confidence in provider (2) (see Table 1 for themes and subcodes with brief examples of representative quotes). Independent inter-rater reliability of code application indicated good agreement (pooled Cohen κ statistic = 0.68).
Applied Codes and Frequency for Resident Identified Barriers to Using the Word “Dying” With Representative Resident Responses/Quotes.
In the mixed-methods analysis of the resident barriers, there was a trend toward identifying a family-centered barrier among the PGY-2 residents as compared to the PGY-3 residents. There was a trend toward PGY-2 residents reporting a specific difficulty or being uncomfortable using the word “dying” as compared to the PGY-3 residents. There was no clear association between resident self-reported comfort or preparation in EOL conversations with any of the themes identified as barriers.
Discussion
Data from the first objective of our study indicate that a 30-minute educational intervention is associated with improved self-reported comfort and preparation in talking about dying with patient surrogates in the ICU. Furthermore, our results suggest that residents are more likely to report acquisition of new communication skills after a simulated family meeting and debrief as compared to a didactic session without simulation.
One important aspect of our intervention was its brevity. Many recent larger studies regarding communication interventions surrounding EOL communication focus on more time-intensive interventions—some as much as 3 days long—which can be impractical in the current graduate medical education system. 9 -12 Our 30-minute intervention can be easily assimilated into the daily routine of residents on their ICU rotations.
To our knowledge, there is a paucity of data comparing differing educational modalities in EOL communication training. Our study suggests that simulated family meetings may lead to improved resident reported skill acquisition as compared with didactic sessions. These results support those of a recent study by Downar et al in which there was a trend toward improved communication skills in the simulation group as determined by blinded evaluators. 19 It is possible that simulation is more likely to improve skill acquisition as trainees have the opportunity to actively participate and test new methods and skills in real time rather than a theoretical discussion of skills.
In our study, residents estimated using the word “dying” to convey the prognosis of imminent death to patients and their families 50% of the time in EOL conversations. There are obvious limitations in resident retrospective recall and estimations of the number of EOL conversations previously conducted. There are likely further limitations in the ability of residents to recall specific word choices—specifically “dying”—used during these conversations. It follows that residents actually used the word “dying” in far less than 50% of EOL conversations. However, our likely overestimated finding highlights a disconnect or at the very least the significant resident discomfort with using the word “dying.”
The most commonly cited barrier to using the word “dying” was uncertain prognostication. Specific representative quotes for this subcoded theme included “confidence in my assessment about the outcome,” “discomfort or lack of clarity about if [the patient] will die soon,” and “uncertainty about predicting who will die.” Resident comments seem to suggest a lack of comfort in relaying death as a possible patient outcome. As is eloquently argued by Back et al in their book, Mastering Communication with Seriously Ill Patients, physicians need to “buck a ‘death-denying’ culture.” 20 Teaching residents to use direct language and the specific word “dying,” even when outcomes are not certain, is one step toward achieving this goal.
There are several limitations to our study. First, this study included residents from a single training program and given that this was a pilot, the reported data are only reactionary and not behavioral based. We relied upon residents to estimate the number of times they used the word “dying” in EOL conversation, subjecting them to recall bias. Additionally, the use of a pre–post design may have biased students toward a “good-student effect” in which they may have responded to the survey as the researcher would want them and thus influenced our comfort, preparation, and learning new skills results. However, both reactionary data and any “good student effect” may not have influenced our data. Assessing perceived skills retrospectively has been shown in the educational research setting to reduce the effect of “response shift bias,” that is, where trainees overestimate their precourse skills prior to training and downgrade their estimates of their precourse skills after they learn the course material. 21 This response shift can result in underestimating the impact of an intervention, whereas a retrospective pretest—as was the case in our study—would be more likely to reflect a learner’s more accurate assessment of their pre- and postskills after they have completed training.
Although our sample size was small and limited to a single department’s trainees and our randomization groups were not equal in number, it was a relatively large sample size compared to other studies that address EOL communication training. Finally, many residents involved in our study participated in a previous general communication training program during their ICU rotations as interns that involved both simulation- and didactic-based education, which may have biased them toward preferring simulation and role play.
It is important to recognize that resident self-reported improvement in comfort, preparation, and skill acquisition may not engender improved patient and family communication and outcomes. In addition, our study did not directly address how families may react to conversations that include the specific word “dying.” Further research is needed to determine whether simulation-based learning leads to improved patient and family outcomes as compared to didactic-based communication training.
Conclusion
In summary, we found that a brief educational intervention resulted in improved self-reported resident comfort and preparation in talking about death and dying with patients and their surrogates in the ICU. End-of-life communication skills can be taught in 30 minutes. Furthermore, simulation may be superior to traditional didactics when attempting to teach vital EOL communication skills to trainees.
Second, a brief survey of internal medicine residents at a single institution identified a disconnect between “resident-perceived prognosis” (death) and “patient-conveyed prognosis” (use of the word “dying”). Residents report using the word “dying” in EOL conversations 50% of the time and identified prognostic uncertainty as the most common barrier to using the word death.
We plan to design future curricula to teach residents to communicate prognostic uncertainty in EOL conversations in the ICU, effectively and directly identifying death as a potential outcome to patients and their surrogates.
Footnotes
Authors’ Note
M.M.H., A.A., J.I.M., and L.R. contributed significantly to curriculum development. D.C.M., A.M.S., and M.M.H. contributed to study design and data acquisition. D.C.M., A.M.S., B.A., and M.M.H. contributed to data analysis. M.S., D.C.M., and M.M.H. contributed to writing and editing the manuscript.
Acknowledgments
The authors wish to acknowledge Henry Fessler, MD (Johns Hopkins University School of Medicine) for allowing us to adapt his case for use in our simulated family meeting. The authors also want to acknowledge the volunteers who role-played in our simulated family meetings.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.