
Abstract
Background:
Older black and Latino Americans are more likely than white Americans to die in the hospital. Whether ethnic differences in expectation of death account for this disparity is unknown.
Objectives:
To determine whether surviving family members’ expectation of death has a differential association with site of death according to race or ethnicity.
Methods:
We conducted an analysis of decedents from the Health and Retirement Study, a nationally representative study of US older adults. Telephone surveys were conducted with family members for 5979 decedents (decedents were 55% were women, 85% white, 9% black, and 6% Latino). The outcome of interest was death in the hospital; the predictor variable was race/ethnicity, and the intervening variable was expectation of death. Covariates included sociodemographics (gender, age, household net worth, educational attainment level, religion) and health factors (chronic conditions, symptoms, health-care utilization).
Results:
Decedents’ race/ethnicity was statistically related to the expectation of death and death in the hospital. When death was not expected, whites and Latinos were more likely to die in the hospital than when death was expected (49% vs 29% for whites and 55% vs 37% for Latinos; P < .001). There was no difference in site of death according to family’s expectation of death among blacks.
Conclusion:
Expectation of death did not fully account for site of death and played a greater role among whites and Latinos than among black Americans. Discussing prognosis by itself is unlikely to address ethnic disparities. Other factors appear to play an important role as well.
Introduction
Palliative care is a philosophy and mode of care that is considered the “gold standard” for those facing life-limiting illnesses. 1 The goals of palliative care are to maximize quality of life, minimize pain and distressing symptoms, and ensure that patients’ preferences for care are respected. These goals are consistent with older adults’ stated preferences for care at the end of life, including place of death. 2 Although older adults mostly prefer to avoid dying in a hospital, most still die there. 3 There are many valid reasons why seriously ill patients die in the hospital, such as uncontrolled pain, personal preferences, and lack of in-home resources. 4 However, death in a hospital has become an important quality metric in palliative care, as it generally indicates that patients have received treatment that negatively impacts quality of life and interferes with the provision of early palliative interventions. 5
However, ethnic differences exist in the care older adults receive at the end of life. Compared to whites, blacks and Latinos are less likely to use hospice. 6 Older blacks and Latinos are more likely to be seen in emergency departments (EDs), resulting in higher rates of hospital admissions and intensive care unit stays. 3 Thus, members of nonwhite ethnic groups are more likely to die in the hospital than whites. These disparities persist among hospice patients for whom care in the home is a priority, 7 despite evidence that hospice is viewed favorably across ethnic groups, albeit at lower rates. 8,9
One possible explanation may be that many older adults, especially older blacks and Latinos, do not recognize that they are nearing the end of their lives. Although older adults are more willing to go to EDs and be hospitalized when near death, 10 those who understand their prognosis is limited are more likely to focus on palliative approaches and want to avoid hospitalizations. 11 This phenomenon has been well-documented among patients with cancer. 12,13 However, little is known about how perceived life expectancy impacts the racial and ethnic differences noted above, though evidence suggests that ethnic differences exist in prognostic awareness. 14,15
Research has focused on older adults’ estimates of long-term prognosis but few, if any, studies have focused on the perception of short-term life expectancy. The Health and Retirement Study (HRS) 16 provides a variable that gives insight into the impact of short-term life expectancy by asking if a loved one’s death was expected at the time it occurred. We hypothesized that a surviving family member’s expectation of death lies on the pathway between race/ethnicity and death in the hospital and would reduce the ethnic differences seen in hospital deaths.
Methods
Participants
We drew a sample of decedents enrolled in the HRS from 2002 to 2012. The HRS is an ongoing longitudinal study of health, retirement, and aging that uses a multistage national area probability sampling design to form a nationally representative sample of all persons in the United States older than 50 years of age. 16 Blacks and Latinos are oversampled to allow analysis within these subgroups. Participants are interviewed every 2 years; additional participants are recruited every 6 years to maintain an on-going representation of older adults. After a participant dies (confirmed using the National Death Index), an interview is conducted with a proxy, generally a surviving spouse or child.
Decedents were included if they were 65 or older at the time of death and if an interview was conducted with a surviving family member after the participant’s death. Exclusion criteria were invalid date of death; race/ethnicity not white, black, or Latino; after-death interview was more than 5 years after the last participant interview; or there was no answer to the HRS’s question on the expectation of death.
Measures
The outcome of interest was death in the hospital, measured by HRS’s question: “At the time of death, was the participant in a hospital, in a nursing home, at home, in a hospice, or what?” Responses were recoded as “yes” (in a hospital) or “no” (all others). The predictor variable was the participant’s race/ethnicity. Using responses to the HRS questions on race and Hispanic ethnicity (Latino), participants were identified as non-Latino white, non-Latino black, and Latino. The expectation of death was the intervening variable, assessed by asking the HRS question: “Was the death expected at about the time it occurred, or was it unexpected?”
We included several covariates that are known predictors of ethnic disparities in end-of-life care and hospital utilization. Categorical variables were created for age at death (65-74, 75-84, 85+), marital status (not married/married), education (high school graduate no/yes), region (urban–suburban no/yes), and wealth (net worth quartiles). Religiosity was assessed using the question: “How important would you say religion is in your life?” (responses: “very important,” “somewhat important,” and “not too important”). We used the Lee prognostic index 17 to estimate prognosis at the participant’s last interview prior to death and control for the effect of prognosis in the analysis. The Lee index uses demographic characteristics (gender, age), health factors (body mass index, smoking, chronic conditions), and functional measures (activities of daily living [ADLs]) to predict 4- and 10-year mortality risk and captures important health-related covariates in one measure. Thus, adjusting for the Lee index allowed us to examine the independent relationships between race/ethnicity and hospital death, thereby accounting for potential inequalities in prognosis between ethnic groups. The Lee index ranges from 1 to 26, with higher scores indicating a higher mortality risk. Because the time from death to the after-death interview varied from decedent to decedent, we included this time interval as a variable.
Analysis
We describe decedent characteristics using descriptive statistics for the total study sample and by ethnic groups. Independent variables included were gender, age, marital status, net worth, education, urban/suburban versus rural location, importance of religion, death was expected, died in hospital, time from death to the final interview, Lee prognostic index, ADL dependencies, chronic conditions, and presence of an advance directive. Age and gender were only included in the descriptive analysis, as they are included in the calculation of the Lee index. The differences between ethnic groups were evaluated using Pearson χ2 tests for categorical variables. A nonparametric (Kruskal-Wallis) test was used for the Lee index and time from death to the exit interview due to the non-normal distribution of these variables.
We used a series of modified Poisson regression models to examine the relationship between race/ethnicity and hospital deaths. We started with an unadjusted model, looking at bivariate relationships between 2 variables. Next, we included known predictors of racial disparities at the end-of-life care and hospital utilization, the Lee index, importance of religion, and time from death to exit interview. We then included expectation of death in our model. This variable was included as both a confounder and an effect modifier to test whether the relationship between race/ethnicity and hospital deaths changes depending on the expectation of death. All analyses used survey weights to account for the complex survey design and were conducted using Stata 14.2 software. 18
Results
Sample Characteristics
The characteristics of the 5979 HRS decedents included in this analysis are shown in Table 1 and are stratified by race and ethnicity. The decedents were mostly female (52.1%), unmarried (53.5%), high school graduates (64.3%), and lived in an urban/suburban community (56.1%). Overall, death was expected for 59.3% of the decedents and 38.8% died in the hospital.
Decedent Characteristics.a
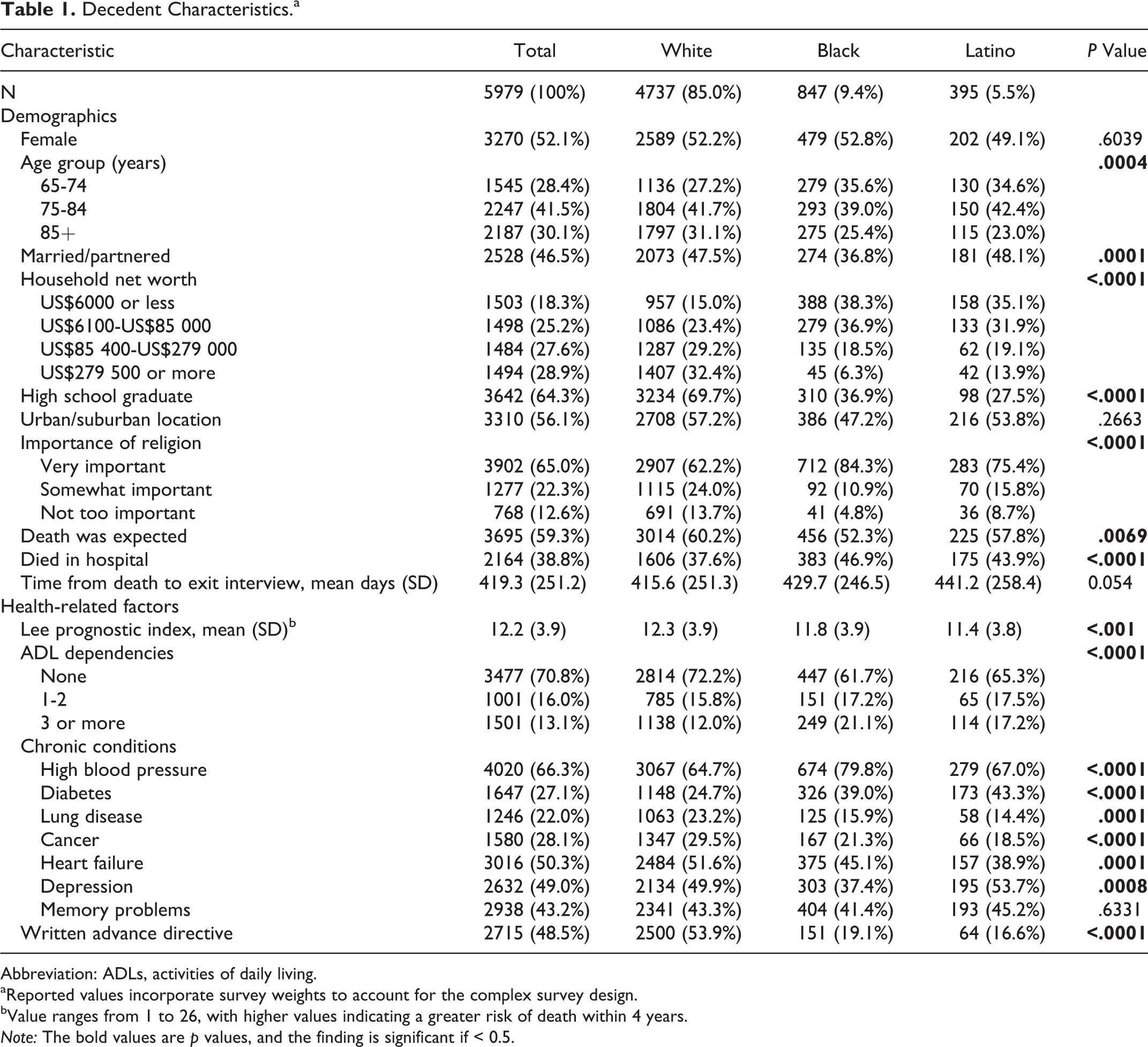
Abbreviation: ADLs, activities of daily living.
aReported values incorporate survey weights to account for the complex survey design.
bValue ranges from 1 to 26, with higher values indicating a greater risk of death within 4 years.
Note: The bold values are p values, and the finding is significant if < 0.5.
We found significant differences between racial and ethnic groups in demographic characteristics, health and health conditions, and health resource utilization. Compared to blacks and Latinos, whites were older, more likely to be high school graduates, and less likely to rate religion as very important. Lee index scores were lower for blacks and Latinos than whites, indicating less risk of death. However, blacks and Latinos reported more ADL impairment than whites. Compared to whites, blacks and Latinos were more likely to die in a hospital, have more chronic conditions (except heart failure), and lack a written advanced directive. We found no significant differences between racial and ethnic groups for urban/suburban residence, the length of time from death to the after-death interview, or memory problems.
The Expectation of Death and Death in the Hospital
The expectation of death was a significant predictor of death outside the hospital (68.2% died outside when death was expected, whereas 50.9% died outside the hospital when death was not expected; P = .006). Significant differences were found when comparing race/ethnicity. Death was expected more among white decedents than blacks and Latinos (whites = 60.2%; blacks = 52.3%; Latinos = 57.8%; P = .007). Expectation of death was also associated with older age (85+ years old = 66.2%; ages 65-74 = 55.3%; ages 75-84 = 57.1%; P < .001), increased ADL dependencies (3+ ADLs = 70.4%; 0 ADLs = 56.0%; P < .001), and the presence of a chronic condition, except diabetes and heart failure (hypertension, P = .04; lung disease, P = .02; cancer, P < .001; memory problems, P < .001; diabetes, P = .16; and heart failure, P = .97).
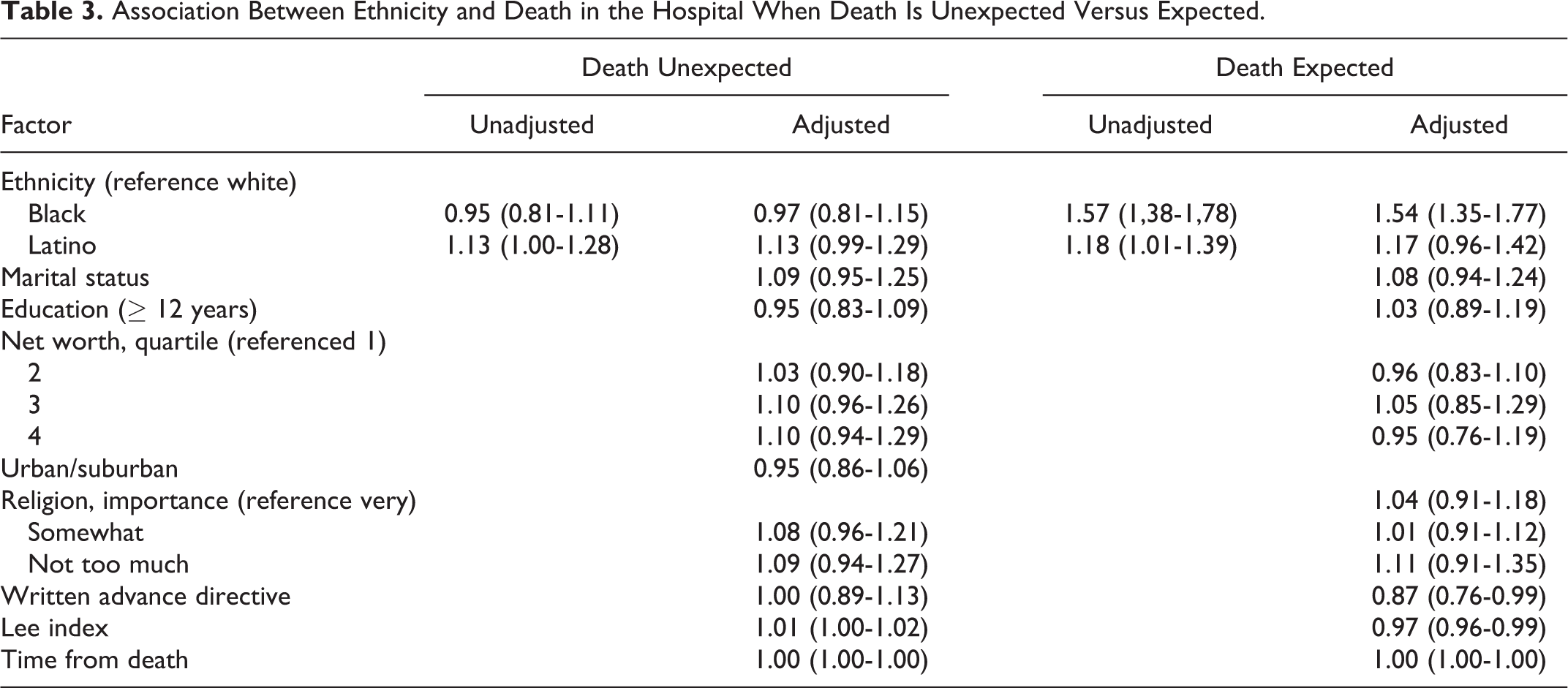
The relationship between race/ethnicity and death in the hospital was tested by calculating the relative risk (RR) of death in the hospital between racial/ethnic groups (Table 2). Unadjusted Poisson regression showed that blacks and Latinos were significantly more likely to die in the hospital than were whites (blacks: RR = 1.25, P < .001; Latinos: RR = 1.17, P = .001). Adjusting for potential confounders attenuated but did not fully explain the relationship (blacks: RR = 1.23, P = .001; Latinos: RR = 1.14, P = .009). Next, we included expectation of death as an effect modifier and found that expectation of death changed the relationship between death in the hospital and race/ethnicity (Table 3). When death was unexpected, hospital death was not significantly different for blacks and Latinos compare to whites (blacks: RR = 0.97, P = .70; Latinos: RR = 1.13, P = .07). When death was expected, race/ethnicity was a significant predictor of hospital deaths for blacks, but not for Latinos (blacks: RR = 1.54, P < .001; Latinos: RR = 1.17, P = .11). We also looked at the interaction term by examining predicted probabilities for each racial/ethnic group (Figure 1; interaction P value < .001). The predicted probability of death in the hospital did not change significantly among blacks based on expectation of death (47% when death was expected vs 45% when death was not expected). For Latinos and whites, in contrast, the likelihood of dying in a hospital differed significantly according to expectation of death (whites: 30% when death was expected vs 49% when death was not expected; Latinos: 37% when death was expected vs 54% when death was not expected).
Association Between Ethnicity, Expectation of Death, and Death in the Hospital.
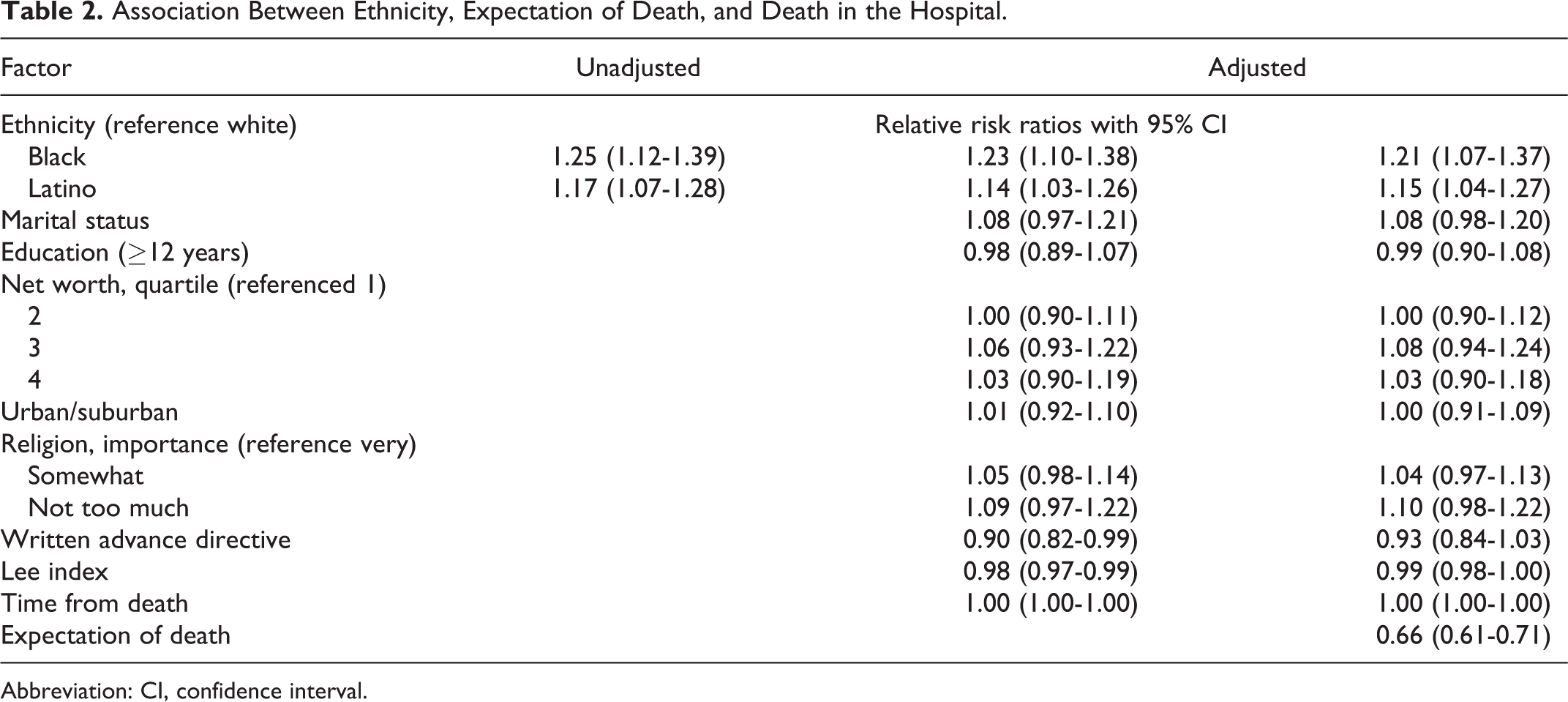
Abbreviation: CI, confidence interval.
Association Between Ethnicity and Death in the Hospital When Death Is Unexpected Versus Expected.
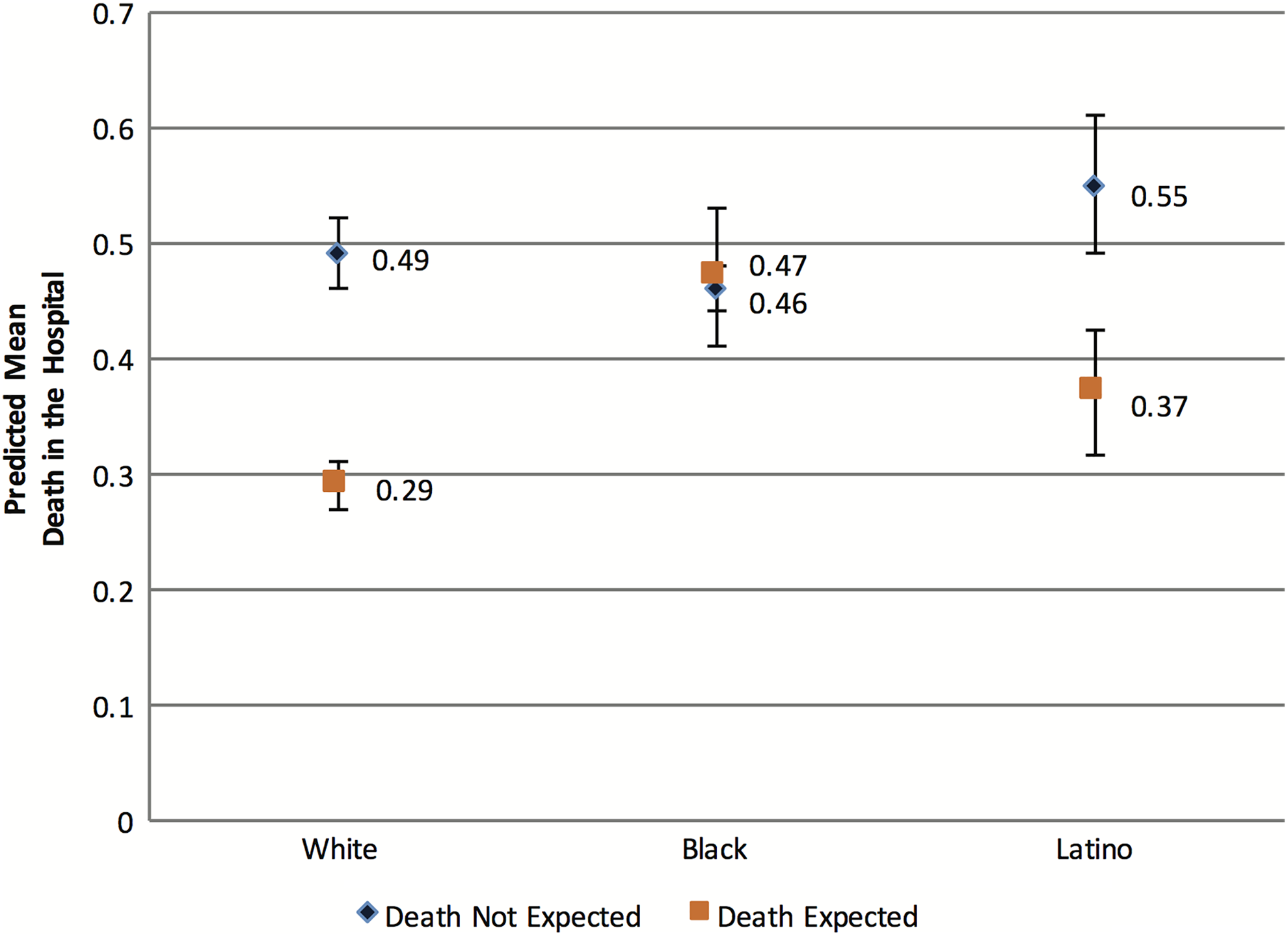
Adjusted predicted probabilities of death in the hospital and race/ethnicity. Including the expectation of death as an effect modifier in the relationship between ethnicity and death in the hospital found a statistically significant difference between whites, blacks, and Latinos. Whites and Latinos were more likely to die in the hospital when death was not expected compared to when death was expected. However, expectation of death had no effect on death in the hospital among blacks.
Discussion
To our knowledge, this is the first study to examine the role of expectation of death on patient outcomes at the end of life. In a nationally representative sample of older adults in the United States, we confirmed previous findings that the expectation of death among family of older adult decedents was associated with the race/ethnicity of the decedent. 14,15 Compared to whites, black and Latino families were significantly more likely to report that death was not expected, and the decedent was more likely to die in a hospital. More importantly, we also found that the expectation of death had a different effect within racial/ethnic groups. There was a significant decrease in the predicted probability of hospital deaths for whites and Latinos, but not for blacks. In addition, when death was expected, compared to whites, the RR of dying in the hospital was not significantly different for Latinos, but was significantly different for blacks. There were major differences between race/ethnic groups in some variables, especially income and education; however, when controlling for race/ethnicity, these variables were not significant predictors of death in the hospital. Our findings bring new and important insights into the care of older adults at the end of life.
Although hospital deaths can be appropriate, we chose death in the hospital as our primary outcome because older adults across racial/ethnic groups prefer home as the place of death. 2 Previous research demonstrates there is significant racial and ethnic disparity for death in the hospital and that hospital deaths are associated with lower quality of life for those with serious illness. 5,19 Our findings that the expectation of death is a strong predictor of death outside the hospital only among whites and Latinos and not blacks have not been noted by other researchers. This suggests that efforts to increase prognostic awareness among whites and Latinos may minimize unnecessary deaths in the hospital for those near the end of life. For blacks, our findings suggest other factors are involved that are not captured in our analysis.
Although the relationship of expectation of death and death in the hospital was different among racial and ethnic groups, discussing prognosis with all patients is important beyond preventing deaths in the hospital. Prognosis discussions help older patients make better and more informed health-care choices, 20 and across racial/ethnic groups, older adults are receptive to and see value in having prognostic discussions. 21 The issue may lie with how well older adults are prepared for these discussions and if the discussions are held in a way sensitive to the individual’s unique racial or ethnic perspective. The secondary nature of this analysis and the design of the HRS limit our ability to explore what other factors may be at play; however, existing literature suggest potential areas that merit more in-depth research.
Discussing the racial and ethnic differences we found must be done with care, as tremendous variability exists within these groups, but looking at racial/ethnic differences is still valuable. Acknowledging and addressing unique racial and ethnic norms is important and appears to change outcomes, particularly for sensitive issues such as end-of-life care. 22
Blacks as a whole are more likely to value religion, believe in miracles, and see end-of-life issues as in God’s hands—beliefs that have been associated with lower prognostic awareness and higher intensity care at the end of life. However, when clinicians are willing to support patients’ spiritual needs, black patients are more willing to forgo interventions that would lead to hospitalizations and to accept hospice. 23 Latinos also value religion but generally view discussions regarding death and dying as taboo, particularly when the patient is actively involved. 24 A primary focus on death may lead to a rejection of end-of-life discussions and recommendations because such talk is considered harmful to the patient.
By being sensitive to racial and ethnic norms and the language used during patient–clinician interactions, clinicians can enhance communication in a way that may lead to a wider range of care decisions. Interventions targeted to specific racial and ethnic groups, including church-based programs, have shown great promise in increasing the completion of advance directives and the acceptance of hospice and palliative care services. 25,26
Communicating prognosis effectively requires a good patient–clinician relationship. However, such relationships are not always present among patients from nonwhite communities and impact the nature of care received. 27 Perceived discrimination may be a factor here. Perceived discrimination has a negative impact on patient–clinician relationships, influencing both the nature of patient–clinician communication and patients’ receptiveness to recommendations. 28 Perceived discrimination is also associated with underutilization of health-care services, 28 which further hinders the development of good relationships. Thus, a cycle may be created that leads to racial/ethnic differences in hospital death. Significant to our findings, the historical experience of discrimination has been markedly different for blacks and Latinos and may help explain why expectation of death had no effect on death in the hospital among blacks. 29,30
By identifying potential factors that lie beneath our findings, we have identified important areas that need further research, including how different racial and ethnic norms influence the communication and understanding of prognosis, the impact of targeted interventions, and how the different experiences of discrimination influence patient–clinician relationships. Understanding these factors will help clinicians better appreciate the complex ways in which race and ethnicity play out in the clinical setting. Identifying racially and ethnically sensitive approaches to communication regarding end-of-life care may have a greater effect on reducing hospital deaths.
Expectation of death has limitations as a variable. We are unable to determine what “the death was expected” meant to the surviving family member, that is, were they referring to an imminent death or a prolonged dying process. Likewise, we are unable to determine whether surviving family members’ and participants’ expectations of death were similar, as patient–family agreement may be low and can impact end-of-life choices. 31 In addition, surrogates use many factors when forming their beliefs about prognosis, of which the clinician’s input is only one. 32 The HRS does not allow us to examine the quality of the patient–clinician relationship, and this relationship may play a much larger role than race/ethnicity alone. Recall bias may have affected our findings, though we controlled for the time from death until the family member was interviewed. Despite these limitations, we utilized a large, nationally representative sample that enables a degree of generalizability that smaller studies cannot provide. Further, as one of the first studies to look at the relationship of expectation of death and racial/ethnic differences in location of death, we have been able to propose important questions for future research and clinical practice.
Future research is needed to better understand the mechanisms that underlie racial and ethnic differences that exist in end-of-life care, including within-group variation. Qualitative research lends itself well to this aim and would provide a depth of understanding that is not possible with large databases. Prospective studies are needed to more clearly illuminate the relationship between race/ethnicity, expectation of death, and care received at the end of life. Used jointly, quantitative and qualitative studies will form a better picture of the phenomenon that can then inform additional research and clinical practice.
Conclusion
We found that the expectation of death did not fully account for death in the hospital and has a stronger role among whites and Latinos than black Americans. Consequently, communicating prognosis by itself is unlikely to address racial/ethnic disparities of care at the end of life. Clinicians need to account for racial/ethnic factors that influence their patients and families and tailor communication accordingly.
Footnotes
Acknowledgments
Rafael D. Romo is a Hospice and Palliative Nurses Association Research Scholar.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was received from the National Institute on Aging [grant number 1K23AG040772] and the American Federation for Aging Research. The work was also supported with resources and facilities at the San Francisco Veterans Affairs Medical Center.