
Abstract
Introduction:
Lung cancer is a leading cause of morbidity and mortality worldwide. Patients with lung cancer may experience a plethora of symptoms, which can be debilitating and affect their quality of life. Palliative care input to manage their physical and psychological well-being is a crucial component of their oncological care. The benefit of early palliative care input has been shown in patients with non-small cell lung cancer; however, data pertaining to patients with small-cell lung cancer are scarce. Nevertheless, early palliative care input is recommended by several national and international guidelines. Thus, we aimed to assess the time to palliative care referrals in patients diagnosed with small-cell lung cancer in an Irish tertiary hospital and to determine what impact this had on overall survival.
Methods:
We performed a retrospective, single-center audit of all patients diagnosed with extensive stage small-cell lung cancer over a 6-year period in an Irish tertiary hospital.
Results:
Overall, 91 patients were identified. Median age at diagnosis was 66 years (range: 38-83 years). The median Eastern Cooperative Oncology Group Performance Status at diagnosis was 1 (range: 0-3); 24 (26%) patients had multiple sites of distant metastasis at diagnosis; 45 (49.5%) patients were alive at 6 months, and 15 (16.5%) patients were alive at 12 months. One hundred percent of patients received palliative care input in our center over the course of their care. In the patients alive at 6 months after diagnosis, there was no survival advantage in those receiving palliative care within 1 month (P = .002, odd ratio: 0.23, 95% confidence interval: 0.09-0.59).
Conclusion:
Palliative care treatment is a critical aspect in the oncological treatment of all patients diagnosed with advanced cancer, and this study highlights good compliance with existing national guidelines. Further research focusing on quality-of-life issues with the use of questionnaires to assess physical and psychological symptoms should be performed to further understand the impact of palliative care in these patients.
Introduction
Lung cancer is the leading cause of cancer-related morbidity and mortality worldwide, responsible for 1.6 million deaths annually. 1,2 Its death rate exceeds that of the 3 most common cancers (colorectal, breast, and prostate). 2,3 In Ireland, lung cancer is responsible for approximately 11% of all invasive cancers excluding nonmelanoma skin cancer and represents the fourth most common cause of malignancy in Ireland after prostate, breast, and colorectal cancers. 4 The most recent data from Ireland state that lung cancer is responsible for 18% of cancer deaths in women and 22% of cancer deaths in men during the period 2010 to 2013. 4
The 2 main histological subtypes in lung cancer are non-small cell lung cancer (NSCLC), responsible for 80% to 85% of cases, and small-cell lung cancer (SCLC), representing approximately 10% to 15% of cases. 2,5,6 Small-cell lung cancer is a highly aggressive malignancy, characterized by a rapid doubling time, a high growth fraction, and early dissemination of disease. Despite being a relatively chemotherapy- and radiation-sensitive disease, recurrence and eventual chemoresistance are frequent. 7 -11 Thus, prognosis in these patients remains extremely poor, with a median survival of 10 to 12 months from diagnosis. In contrast to the progress being made in NSCLC, there has been very little development in chemotherapeutic options for SCLC since the introduction of a platinum–etoposide doublet as a standard of care almost 4 decades ago, corresponding to little improvement in overall survival. 9 -11
The poor prognosis observed in these patients is also compounded by other factors such as advanced age at diagnosis, with more than half of these cases are diagnosed in people older than 65 years. Furthermore, diagnosis is often made at a late stage, with up to 70% of patients with SCLC presenting with extensive stage (ES), or advanced, disease. 5,9 Smoking is a major risk factor; thus, other comorbidities such as hypertension, coronary artery disease, and chronic obstructive pulmonary disease are frequently observed in these patients. Subsequently, a large proportion of patients, approximately 60%, are not fit for any form of treatment at the time of diagnosis. 5,12 Increasing symptom burden and resulting impairment in quality of life (QOL) throughout the course of this life-threatening illness often create great distress for both the patient and their caregivers. Given the plethora of physical and psychological symptoms that these patients may experience, multidisciplinary input is encouraged to optimize patient outcomes.
The emergence of palliative care (PC) as an adjunct in the care of patients with cancer has expanded in recent years. 13 -17 According to the World Health Organization, PC aims to improve the QOL of patients and their families facing the multitude of issues surrounding this life-altering diagnosis, through “the prevention and alleviation of suffering, by means of early identification and impeccable assessment and treatment of pain and other physical, psychosocial and spiritual problems.” 18(p94)
Early PC input to aid in the management of these symptoms as well as maintaining patients’ psychological well-being is a crucial part of their oncological care. Recent studies have shown that early implementation of PC and discussion of the patients’ goals and preferences earlier in the course of disease can lead to improved symptom control and reduced distress and limit hospitalizations and aid in the decision-making with regard to the delivery of care. 13,17,19 These studies, however, center around patients with NSCLC, and data with regard to the benefit of PC in patients with SCLC are limited. Nevertheless, clinical guidelines from the American Society of Clinical Oncology (ASCO) now recommend that PC be integrated into standard oncologic care. 20,21
Most cancer centers now have well-established PC services; however, these remain underutilized. Defining the ideal time for PC intervention is often both disease- and patient-specific, and traditionally input is not sought until the disease is at an advanced stage, when the patients are hospitalized, or when patients have uncontrolled symptoms. The National Clinical Programme for Palliative Care now recommends referral at diagnosis for a basic needs assessment in all patients diagnosed with a life-limiting condition. 22
Thus, the primary objective of this audit was to evaluate the time to PC referrals in patients diagnosed with ES SCLC in our cancer center and determine what impact, if any, this had on overall survival.
Methods
We performed a retrospective, single-center audit of all patients diagnosed with ES SCLC over a 6-year period (January 2010 to December 2016) in an Irish tertiary hospital (University Hospital Limerick). Patients were identified using the hospitals’ inpatient enquiry database. Ethical approval from the hospital ethics committee was obtained prior to data collection. Clinical data were collected from patients’ medical records, hospital pathology, and imaging reports. The data were merged into a single database and deidentified by assigning unique patient identifiers to protect patient confidentiality. Clinical parameters included in the database were age at diagnosis, smoking status, and Eastern Cooperative Oncology Group (ECOG) Performance Status (PS; with 0 indicating that the patient is asymptomatic, 1 that the patient is symptomatic but fully ambulatory, 2 that the patient is symptomatic and in bed less than 50% of the day, and 3 capable of only limited self-care, confined to bed or chair more than 50% of the day). 23 In addition to clinical symptoms, sites of metastases, serum albumin at diagnosis as an indicator of nutritional status, number of lines of chemotherapy, total number of hospitalizations, time to PC referral from initial diagnosis, and time to recurrence/death were also recorded.
Statistical analyses were performed with the use of SPSS software, version 24.0 (SPSS). Descriptive statistics were used to estimate the frequencies, means, medians, and standard deviations or interquartile ranges (IQRs) of the study variables. Differences between study groups in baseline characteristics and clinical outcomes were assessed with the use of 2-sided Fisher exact tests and multivariate linear regression analyses. A logistic regression model was formed to identify predictive variables that may impact overall survival. Cox regression survival analysis was used to assess the effect of PC on survival.
Results
A total of 115 patients with a diagnosis of SCLC over a 6-year period were identified; 24 patients were diagnosed with limited stage disease and were excluded from the analysis, and 91 patients were diagnosed with ES disease at diagnosis. Baseline characteristics are shown in Table 1 (n = 91). Of these patients, 56% were male (n = 51), while 44% were female (n = 40). Median age at diagnosis was 66 years (range: 38-83 years). Sixty-nine percent (63/91) were active smokers and 16% (15/91) were ex-smokers. Two patients had no history of smoking. The smoking status of 11 patients was unknown. The median ECOG PS at diagnosis was 1 (range: 0-3). Twelve percent (11/91) of patients presented with an ECOG PS of 0, while 51% (46/91) had a PS of 1. Thirteen percent (12/91) had an ECOG PS of 2 and 24% (22/91) had a PS of 3. Sixty-six percent (60/91) of patients had distant metastatic disease at diagnosis. The most common sites were liver (34% [31/91]), bone (27% [25/91]), adrenal glands (26% [24/91]), and brain (15% [14/91]). Twenty-six percent (24/91) of patients had multiple sites of distant metastasis at diagnosis. Median serum albumin at diagnosis was 33 g/L (range: 19-44 g/L). Fifty-four percent (49/91) of patients had a low serum albumin level (<35 g/L) at diagnosis, while 43% (39/91) had a normal albumin level (35-50 g/L). The serum albumin level in 3 patients was unknown (3%).
Patient Demographics in Patients Diagnosed With Extensive Stage Lung Cancer.
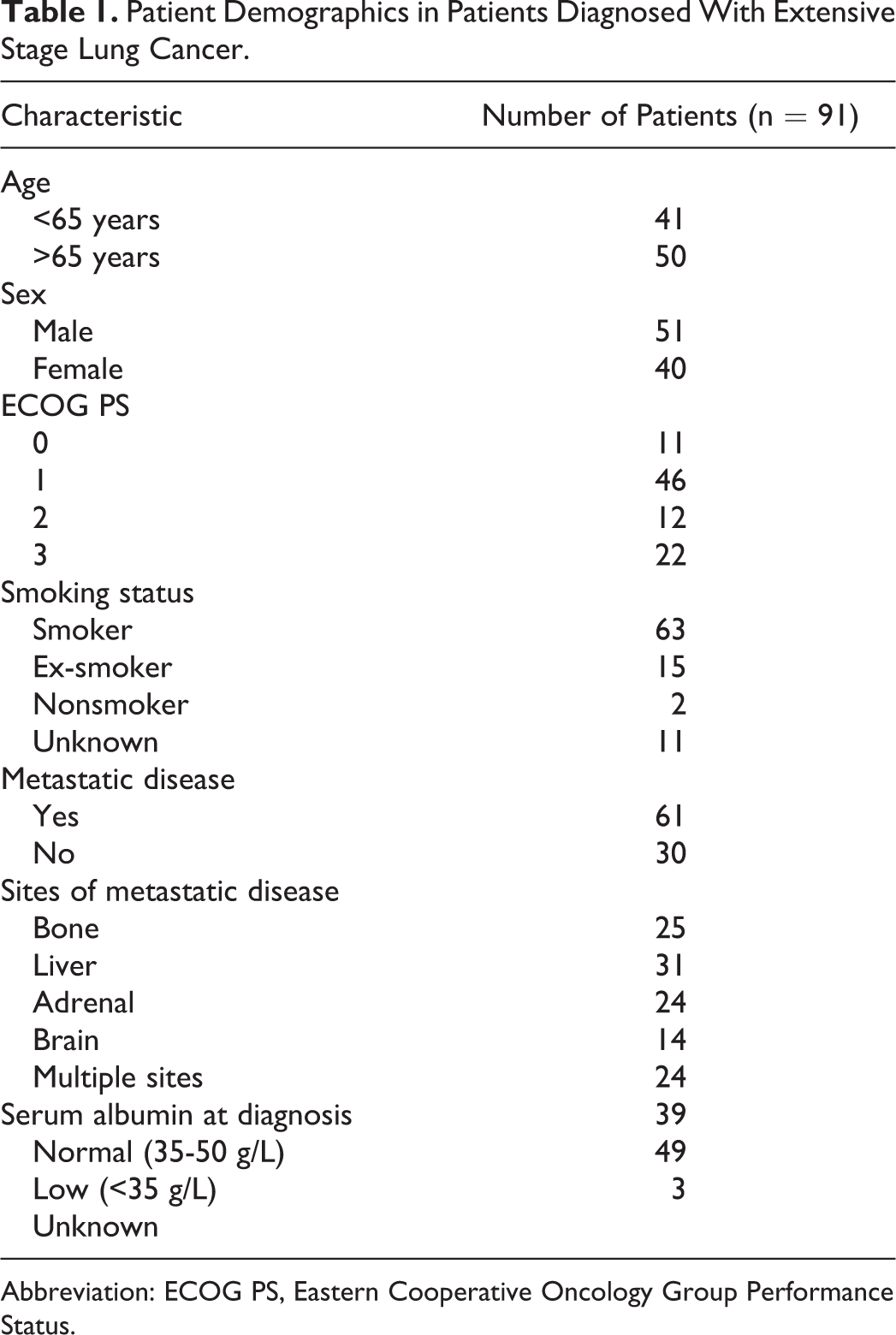
Abbreviation: ECOG PS, Eastern Cooperative Oncology Group Performance Status.
Cough was the most common presenting complaint, reported in 36% (33/91) of patients (Figure 1). Thirty-one percent (28/91) complained of shortness of breath (28/91) and 22% reported weight loss (20/91). Other symptoms at diagnosis included chest pain (14/91), lower respiratory tract infections (13/91), hemoptysis (6/91), and back pain (6/91). Diagnosis in 5 patients was incidental. Complications observed after diagnosis included superior vena cava obstruction (13/91), syndrome of inappropriate antidiuretic hormone production (11/91), spinal cord compression (6/91), neutropenic sepsis (5/91), seizures (3/91), and non-ST-segment elevated myocardial infarction (1 patient; Figure 2).

Presenting complaints at diagnosis.
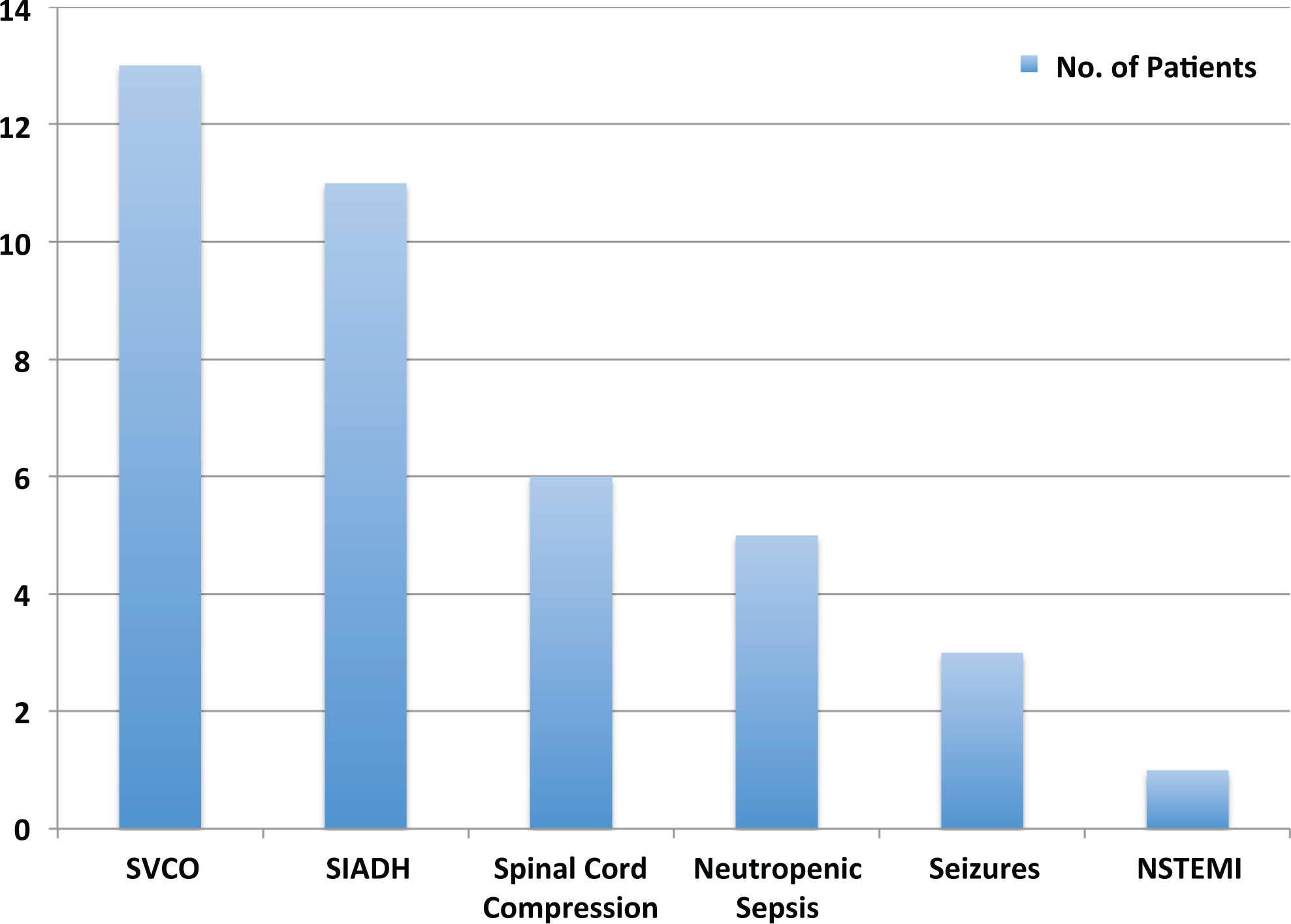
Complications at diagnosis and during treatment.
Seventy-three percent (66/91) of patients were fit for chemotherapy. Twenty-seven percent (25/91) of patients did not receive chemotherapy due to a poor PS or patient preference. Cisplatin/etoposide (27/66 patients) and carboplatin/etoposide (30/66 patients) were the most common regimens used. Nine patients were treated with single-agent carboplatin. Thirty-eight of these patients had a radiological response to treatment (58%), with 12 patients radiologically progressing after treatment (18%). Sixteen patients clinically progressed or died prior to their restaging scan. Of the 38 responders, 27 proceeded to prophylactic cranial irradiation (PCI) (71%). Of these 27 patients, 20 (74%) progressed radiologically, with an average progression-free survival of 5.4 months. Eight (40%) patients were fit for second-line treatment, with 4 receiving Cyclophosphamide, Doxorubicin and Vincristine (CAV) (4/8) and 4 receiving a platinum rechallenge (4/8). Seven patients received palliative radiotherapy.
The vital status of 88 patients was recorded at the time of data cutoff. Three were diagnosed within 6 months of data cutoff and were excluded. Forty-five (49.5%) patients were alive at 6 months and 15 (16.5%) patients were alive at 12 months. Median number of hospitalizations from time of diagnosis was 1 (IQR: 0-1). Median time to progression was 5 months (IQR: 1.25-6.0 months), and median overall survival was 4 months (IQR: 2-11 months).
One hundred percent of patients received a PC referral. Median time to PC referral was 1 month (IQR: 1-3 months). Sixty-four percent (58/91) of patients were referred for PC input within 1 month of diagnosis, and 67 (73.6%) patients were referred to PC within 3 months (Figure 3).
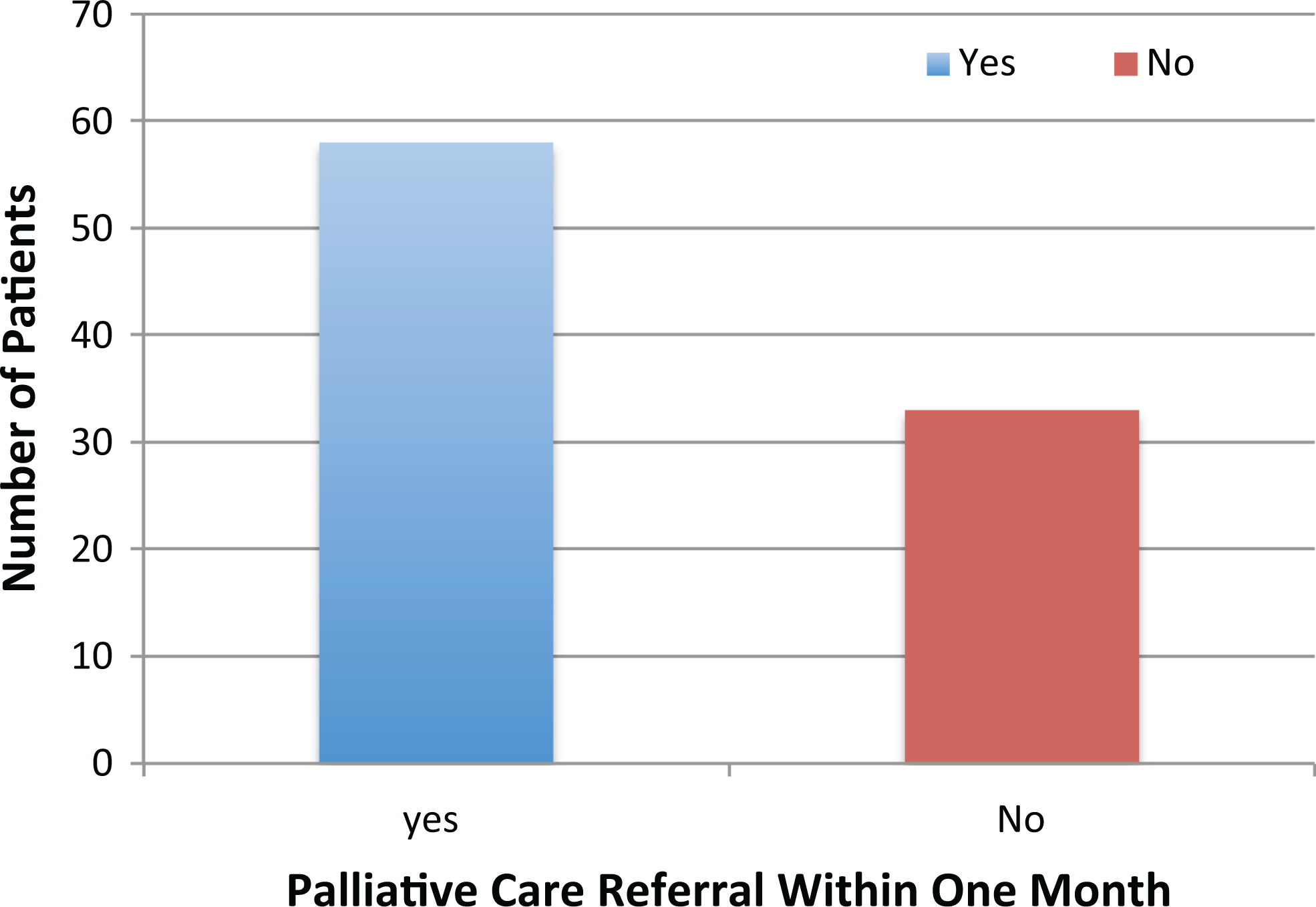
Number of patients receiving palliative care within 1 month of diagnosis.
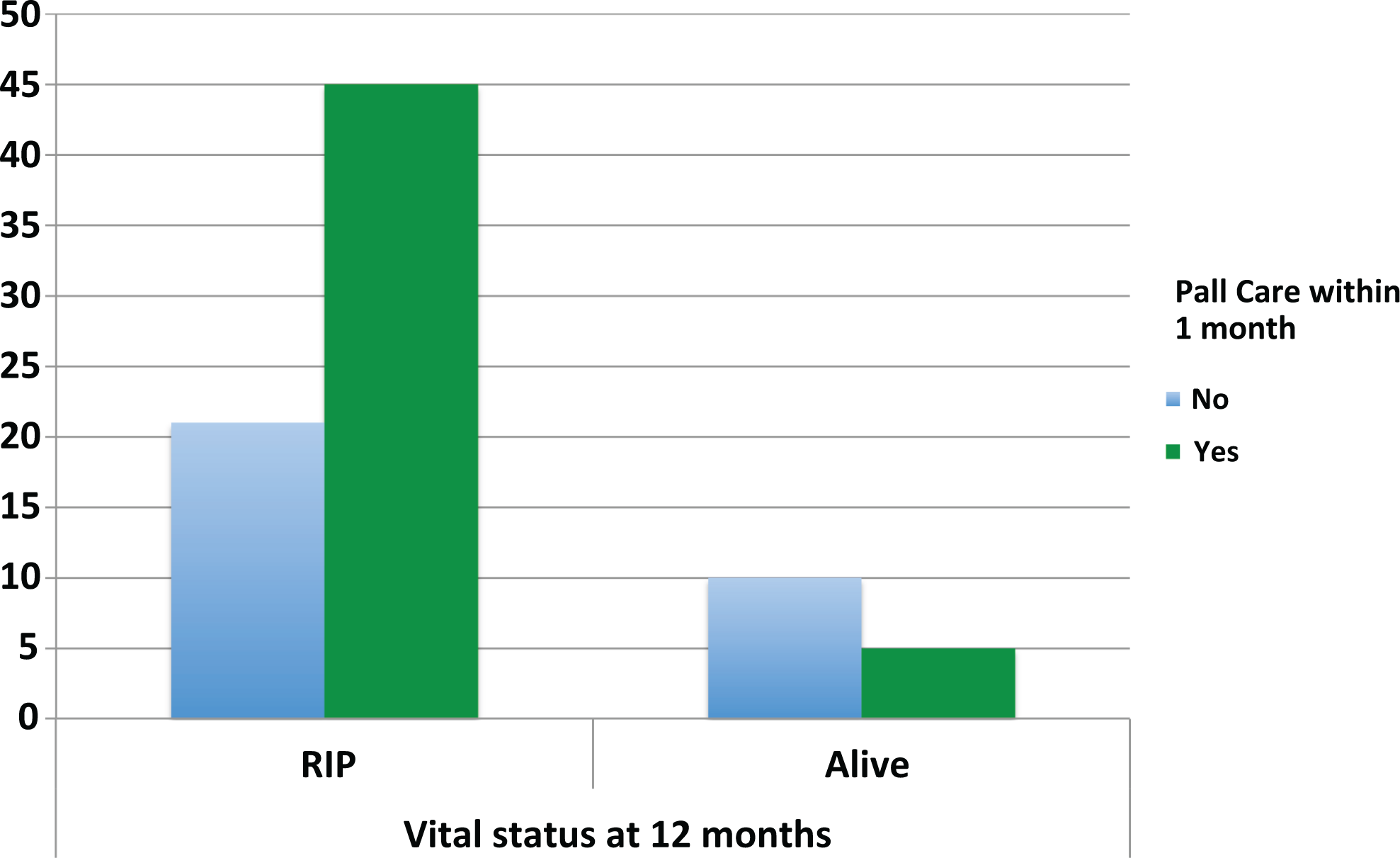
Forty-five (51%) patients were alive at 6 months. Of these patients, 47% (21/45) had received a PC referral within 1 month of diagnosis (Figure 4). Of the 43 patients who had died within 6 months of diagnosis, 34 (79%) patients received a PC referral within 1 month. There was no survival advantage observed in those receiving PC within 1 month (P = .002, odds ratio [OR] = 0.23, 95% confidence interval [95% CI] = 0.09-0.59). At 12 months, 10% (15/81) of patients were alive (Figure 5). Ten patients were excluded as they were diagnosed within 12 months of data cutoff. In total, 62% (50/81) had received a PC referral within 1 month. Of those receiving early PC (within 1 month), only 5 (10%) were alive at 12 months. Again there was no survival advantage observed in those receiving early PC input (P = .018). Ten patients who did not have PC within 1 month of diagnosis were still alive at 12 months.

Number of patients receiving palliative care within 1 month of diagnosis alive at 6 months (n = 88). No survival advantage was seen in those receiving palliative care within 1 month (P = .002, odds ratio [OR] = 0.23, 95% confidence interval [95% CI] = 0.09-0.59).
Number of patients receiving palliative care within 1 month of diagnosis alive at 12 months (n = 81). No survival advantage was seen in those receiving palliative care within 1 month (P = .018).
Time to hospitalization after chemotherapy was found to be a predictive variable in patients alive at 12 months (OR = 2.49, 95% CI = 1.03-6.04, P = .043), as was time to progression (OR = 2.84, 95% CI = 1.01-8.02, P = .049). Serum albumin was identified as an independent predictive variable in those patients alive at 12 months (OR = 1.08, 95% CI = 1.03-1.12, P = .001; Figure 6).
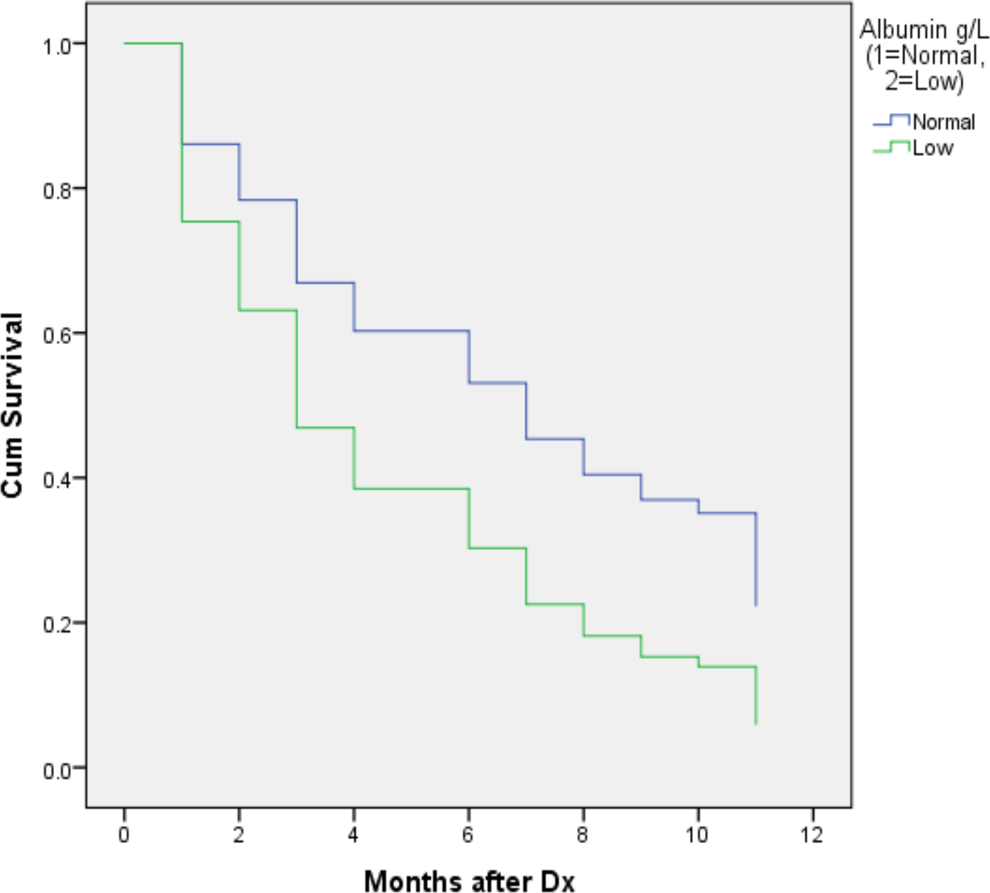
Cox regression survival analysis demonstrating normal serum albumin as an independent predictor of survival (odds ratio [OR] = 1.89, 95% confidence interval [95% CI] = 1.11-3.21, P = .02).
Discussion
In the current study, 91 (79%) patients were diagnosed with ES disease and 24 (26%) patients had multiple sites of metastatic disease at diagnosis. The median age at diagnosis was 66 years, and 78 patients were either active smokers or had a history of smoking. Thirty-four (37%) patients had an ECOG PS of ≥ 2, while 25 (27%) patients were not fit for chemotherapy at diagnosis. These characteristics reflect a fragile population, with likely comorbidities and the potential for significant symptomatology during the course of their disease.
This study highlights good compliance with existing national guidelines with regards to PC referrals. The Palliative Care Needs Assessment Guidance was prepared by the National Clinical Programme for Palliative Care Working Group in 2014 with the aim of providing all patients with life-limiting conditions the best possible QOL. 22 One hundred percent of patients included in this analysis received a PC referral. Sixty-four percent (58/91) of these patients were referred to PC within 1 month of diagnosis, while 73.6% (67/91) of patients were referred within 3 months. The median time to PC referral was 1 month (range = 1-22 months).
These early referrals were facilitated by the attendance of the PC team at our weekly multidisciplinary meetings, where newly diagnosed patients are discussed. In addition, PC advanced nurse practitioners (ANPs), while not formally allocated to oncology clinics, are often readily available for consults if needed. A basic needs assessment may be performed and follow-up appointments may then be made either to return to the specialized PC clinic for consultant review or follow-up in the community. The benefit of embedding PC ANPs into oncology clinics is an area of active research, and many early studies have shown it to be well received by patients, facilitating early PC input and improving end-of-life care. 24 -26
Typically, PC is not sought until the disease is at an advanced stage requiring hospitalization or if the patient has uncontrolled symptoms that severely impair their QOL. 27,28 Previous studies have suggested that late referrals to PC are inadequate to alter the quality and delivery of care provided to patients with cancer; thus, several organizations such as the ASCO, National Comprehensive Cancer Network, and European Society of Medical Oncology have issued clinical opinions recommending the use of PC earlier in the course of disease. 19,29 -32
The importance of early PC and the impetus for the development of these guidelines have been provided by several randomized trials that have provided evidence that patients who received early PC input had improved QOL, reduced intensive care unit admissions, increased time spent at home, longer stay in hospice, and lower overall cost of care and health-care use. 33 -35 One of the most notable studies in recent years was performed by Temel et al, who evaluated the impact of the introduction of PC in patients with NSCLC at the time of diagnosis on changes in QOL after 12 weeks of treatment. 36 Improved QOL was reported in those receiving early PC input, compared with those receiving standard care only. Furthermore, fewer depressive symptoms were observed in the PC group. Perhaps, the most striking finding, however, was overall survival. Despite patients in the PC group receiving less aggressive care at the end of life, their median survival was longer (11.6 vs 8.9 months, P = .02). 36 This suggests that early PC, by controlling symptoms and improving QOL, can translate into a survival advantage without the use of aggressive medical care. However, the current study failed to show a survival benefit when PC was sought early. In the patients alive at 6 months after diagnosis, there was no survival advantage in those receiving PC within 1 month (P = .002, OR = .23, 95% CI = 0.09-0.59). This may be limited by the fact that the more symptomatic, or less well patients, are referred earlier. A large proportion of patients (37%) had a poor ECOG PS (≥2) at diagnosis (34/91) and 66% (60/91) had distant metastasis.
Debilitating symptoms such as cough (33/91), shortness of breath (28/91), weight loss (20/91), chest pain (14/91), hemoptysis (6/91), and back pain (6/91) reported in our patients can severely limit daily activities, cause hospitalizations, and significantly impair QOL, which can subsequently result in severe psychological implications. Depression is common in patients with lung cancer, with an incidence rate of 15% to 44% in newly diagnosed patients with NSCLC. 13,37 It has been shown that psychological distress is more frequently observed in patients with lung cancer, when compared to patients with other solid malignancies. 13
An early emphasis on addressing these issues can not only improve QOL but it has also has been shown to improve patient understanding of their disease and their ability to voice their own preferences, avoiding aggressive end-of-life care and ultimately resulting in increased satisfaction with their care. This approach can dramatically reduce depression and anxiety in both patients and their caregivers. 19,20,38 -40
Another aspect of the analysis that favors multidisciplinary input was the measurement of serum albumin at diagnosis as an indicator of nutritional status. With a median serum albumin of 33 g/L (range: 19-44 g/L), these patients are undernourished and require dietary input early to optimize their condition prior to starting systemic treatment. Twenty-two percent of patients complained of weight loss at diagnosis and 49 (54%) of 91 patients had a low serum albumin level (<35 g/L) at diagnosis. Serum albumin levels have already been shown to be an independent predictor of survival in patients with metastatic NSCLC, and the Royal Marsden Hospital score uses serum albumin along with serum lactate dehydrogenase and sites of metastasis in a prognostic model when screening patients for phase 1 clinical trials. 41,42 Thus, early dietetic input may also improve PS and subsequently impact patient outcomes.
Limitations of the study deserve mention. It was a retrospective study performed at a single, tertiary care site with a small number of patients. Patients with features of more advanced disease such as poorer PS, distant metastases, and increasing symptom burden were more likely to receive earlier PC referrals, thus impacting on overall survival. This also created a referral bias, resulting in the unusual finding of a statistically significant survival disadvantage in those receiving early PC input.
In conclusion, PC treatment is a critical aspect in the oncological treatment of patients with lung cancer. These patients are particularly vulnerable to increased symptom burden and reduced QOL, and early implementation of PC in patients with NSCLC has been shown to have a meaningful impact. More research is required to assess needs of patients with SCLC and investigate how they differ from their NSCLC counterparts.
Although compliance to national guidelines with regard to PC referrals in our center was good, there is still room for improvement. Further research focusing on QOL issues with the use of questionnaires to assess physical and psychological symptoms should be performed to further determine the impact of PC in these patients. Increased awareness of these benefits is fundamental in ensuring optimal patient outcomes and patient satisfaction with their oncological care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.