
Abstract
Background:
Although most children at end of life have commercial insurance, little is known about their demographic and clinical characteristics, what care they are receiving, and how much it costs.
Objectives:
To describe commercially insured children who enrolled in hospice care during their last year of life and to examine differences across age-groups.
Methods:
A retrospective cohort study was conducted using 2005 to 2014 data from the MarketScan Commercial Claims and Encounters database from Truven Health Analytics. Variables were created for demographics, health, utilization, and spending. Analyses included χ2 and analysis of variance tests of differences.
Results:
Among the 17 062 children who utilized hospice, 49% had a preferred provider organization (PPO). Hospice length of stay averaged less than 5 days. Over 80% of children visited their primary care physician. Eight percent had hospital readmissions, and 38% had emergency department (ED) visits. Average expenditures were US$3686 per month or US$44 232 annually. The most common condition for children less than 1 year was cardiovascular (21.96%). Neuromuscular conditions were the most frequent (7.89%) in children aged 1 to 5 years, while malignancies (10.53% and 11.32%, respectively) were prevalent in ages 6 to 14 and 15 to 17. Children less than 1 year had the highest frequency of hospital readmissions (16.25%) with the lowest ED visits (28.67%) while incurring the highest expenses (US$11 211/month).
Conclusions:
The findings suggest that commercially insured children, who enroll in hospice, have flexible coverage with a PPO. Hospital readmissions and ED visits were relatively low for a population who was seriously ill. There were significant age-group differences.
Keywords
As medical technology advances the care of children with serious illness, over 100 children still die each day with life-limiting health conditions. 1 Pediatric hospice care is one approach to offering interdisciplinary team care for children with the guiding philosophy to improve quality of life for children with a prognosis of 6 months to live or less. 2,3 It provides holistic, family-centered care that is tailored to meet the needs of each child and family. 3 Pediatric hospice care is often provided in the home, hospital, or dedicated facility. 4 Access to pediatric hospice care can offer families a layer of support, as they navigate end-of-life care for their child. 5 The benefits of hospice care for children and families include improved symptom management. 6 However, very few children access hospice. Recent reports found that approximately 10% of seriously ill children utilize this important care model. 7
What is known about children who enroll in hospice care is predominantly focused on those children with public insurance such as Medicaid. 8 Emerging evidence suggests that pediatric Medicaid beneficiaries have significant health problems, including multiple comorbidities. 9,10 The care they receive at end of life is often fragmented with high rates of hospital readmissions and emergency visits, while seldom utilizing hospice care. 11,12 Additionally, their end-of-life care is incredibly resource intensive and costly. 7 However, little is known about children in commercial insurance, and more than half of children have this coverage. 13 Although commercial insurance databases have been around since the mid-1990s, commercially insured children have not been the focus of previous research. Thus, knowledge about commercially insured patients enrolled in hospice care—their demographic and clinical characteristics, what care they are receiving, and how much it costs–has eluded hospice and palliative care clinicians. Recently, databases such as the MarketScan Commercial Claims and Encounters database have improved access to data on commercially insured children and have enabled research to begin examining these unique populations. Given the importance of health insurance in the delivery and cost of care, improving knowledge of commercially insured children who enrolled in hospice care will inform clinical practice for those caring for children at end of life.
This study was guided by the Andersen Behavioral Healthcare Utilization model. 14 The Andersen Model posits that an individual’s use of health care services and costs of those services are a function of an individual’s predisposition to use services (predisposing factors), factors that support or impede use (enabling factors) as well as their need for health care (need factors). 15 For this study, commercially insured children may be predisposed to use health care services based on demographics. Evidence suggests that a child’s age, sex, and place of residence influence utilization of end-of-life care including hospice utilization, primary care visits, hospital admission, and emergency department (ED) visits. 9,16 –18 Enablers such as type of insurance have also been related to end-of-life care for children, 9,12,13,16 while the health of the child has been shown to be a critical driver of utilization and costs of care. 7,9,16 Thus, this framework suggests that predisposing, enabling, and need factors are potential considerations when examining health utilization and spending among commercially insured children at end of life.
The current study sought to describe the characteristics of commercially insured children who enrolled in hospice care during their last year of life. A secondary aim was to conduct a preliminary examination of the differences in child characteristics across age-groups. Drawing from the literature, demographics, health, utilization, and spending variables were utilized to understand the profile of some of the sickest children in our health care system. Improving our knowledge of these children is critical for pediatric hospice and palliative care clinicians who are on the frontline of delivering care and educating children and families. Study findings are discussed in terms of clinical practice implications.
Methods
Design and Sample
In this retrospective cohort study of administrative billing data, children at end of life were identified based on their enrollment in hospice care. Since the date of death was not available in the database, a proxy definition was used to designate mortality. Hospice claims activity as a proxy for defining death has been used extensively in end-of-life research. 19 –22 For this study, end of life was defined as the 12 months prior to the date of the last hospice claim. Children were included in the sample if they were aged 0 to 17 years, were enrolled in a commercial insurance plan during any part of the year, and had hospice claims between January 1, 2005, and December 31, 2014. If the child was in the database for multiple years, only the last year of life was used for this study. All outliers were individually examined and excluded. After applying the inclusion and exclusion criteria, the final sample was 17 062 commercially insured children who enrolled in hospice care in their last year of life. Institutional Review Board approval for this study was obtained from the Pennsylvania State University, College of Medicine.
Data Source
To generate information on commercially insured children at end of life, data from the 2005 to 2014 Marketscan Commercial Claims and Encounters database (Truven Health Analytics, an IBM Company) were used. The Commercial Claims and Encounter files include national, individual-level claims data from active employees, early retirees, COBRA continues, and dependents who were insured by employer-sponsored plans. 23 These longitudinal records included patient demographics, health information, inpatient and outpatient services, and cost of care. Marketscan is one of the few commercial insurance claims databases available for health care research and has been used widely to examine health and health care delivery. It is considered representative of the US health population concerning health coverage. 1,24 All database records were deidentified and fully compliant with US patient confidentiality requirements, including the Health Insurance Portability and Accountability Act of 1996. Quality standards for the MarketScan research databases are maintained by Truven Health Analytics, an IBM Company.
Measures
Separate groups of study variables were created a priori based on the Andersen Model for demographics, health characteristics, health care utilization, and health care spending. 7,9,16 Demographics included age, sex, insurance type, region, and metropolitan area. Age was categorized as <1 year, 1 to 5 years, 6 to 14 years, and 15 to 17 years. Sex was operationalized as male or female. Insurance type was the type of commercial insurance plan that covered the child’s health care. It was categorized as preferred provider organization (PPO), point of service plan (POS), health maintenance organization (HMO), comprehensive, and exclusive provider organization (EPO). Region where the child resided was categorized as Northeast, Midwest, South, and West based on the US Census Bureau classification. The measure of metropolitan area was a binary variable of rural or urban residence of the child based on whether the child lived in a Metropolitan Statistical Area.
The health characteristics included complex chronic conditions (CCCs) and multiple CCCs. Complex chronic conditions were categorized into 9-organ system-based CCC types: neuromuscular, malignancy, congenital/genetic, cardiovascular, metabolic, hematologic/immunologic, respiratory, renal, and gastrointestinal. 25,26 The categories in the analysis were derived from International Classification of Disease (ICD), ICD-9/10 codes and were not mutually exclusive. The definition of CCCs is that a condition lasts at least 1 year, is severe enough to necessitate subspecialty pediatric care, and bears the highest risk of mortality out of all chronic conditions in childhood. 25,26 Multiple CCCs were operationalized as the number of CCCs (0-4+).
Several variables describing health care utilization were created: hospice use, hospice length of stay, primary care visit, hospital readmissions, and ED visit. Hospice use was the frequency of hospice enrollment during 2005 to 2009 and 2010 to 2014. Hospice length of stay was defined as the number of days the child was enrolled in hospice care or the length of stay. Primary care visit was whether or not the child used primary care in the last year of life. Hospital readmissions were whether or not a child had 3 or more hospital admissions during the last year. Whether or not the child used the emergency department was the measure of ED visit.
A group of monthly spending measures were created for this study. Expenditures were the monthly sum of commercial insurance payments to health care providers in the child’s last year of life. Coinsurance, copayment, and deductible were the monthly sums of coinsurance, copay, and deductible payments, respectively. All spending amounts were adjusted to 2014 US dollars and to minimize the influence of outliers.
Data Analysis
Using pooled cross-sectional data, the analysis plan included generating descriptive statistics on demographics, health, utilization, and spending for all children in the sample. For the analysis, the children were stratified by age (<1 year, 1 to 5 years, 6 to 14 years, and 15 to 17 years). The Pearson χ2 test for differences in proportions was used to provide comparisons between the pediatric age groups. Analysis of variance was used to compare mean hospice length of stay across the age-groups. The results are presented in the form of univariate distributions and means. The data analysis for this study was generated using SAS software (Copyright 2013 SAS Institute Inc.). SAS and all other SAS Institute Inc products are registered trademarks or trademarks of SAS Institute Inc, Cary, North Carolina.
Results
The demographic characteristics of the children are presented in Table 1. Overall, the children were evenly divided between males and females. Preferred provider organization type of commercial insurance was the most common (48.94%), while EPO was the least common (0.49%). Children generally resided in the South (49.43%) and in urban areas (90.92%). Across the age-groups, males were more common in <1 year (52.08%), 1 to 5 years (58.89%), and 6 to 14 years (50.89%). A majority of children were females in the 15 to 17 year (55.71%) age group. The PPO was the most frequent type of commercial insurance for children <1 year (43.87%), 6 to 14 years (51.70%), and 15 to 17 years (57.33%); whereas POS type was the most frequent for children 1 to 5 years (49.97%). The South was the most common region for all age-groups along with urban residence.
Demographics of Commercially Insured Children at End of Life (N = 17 062).
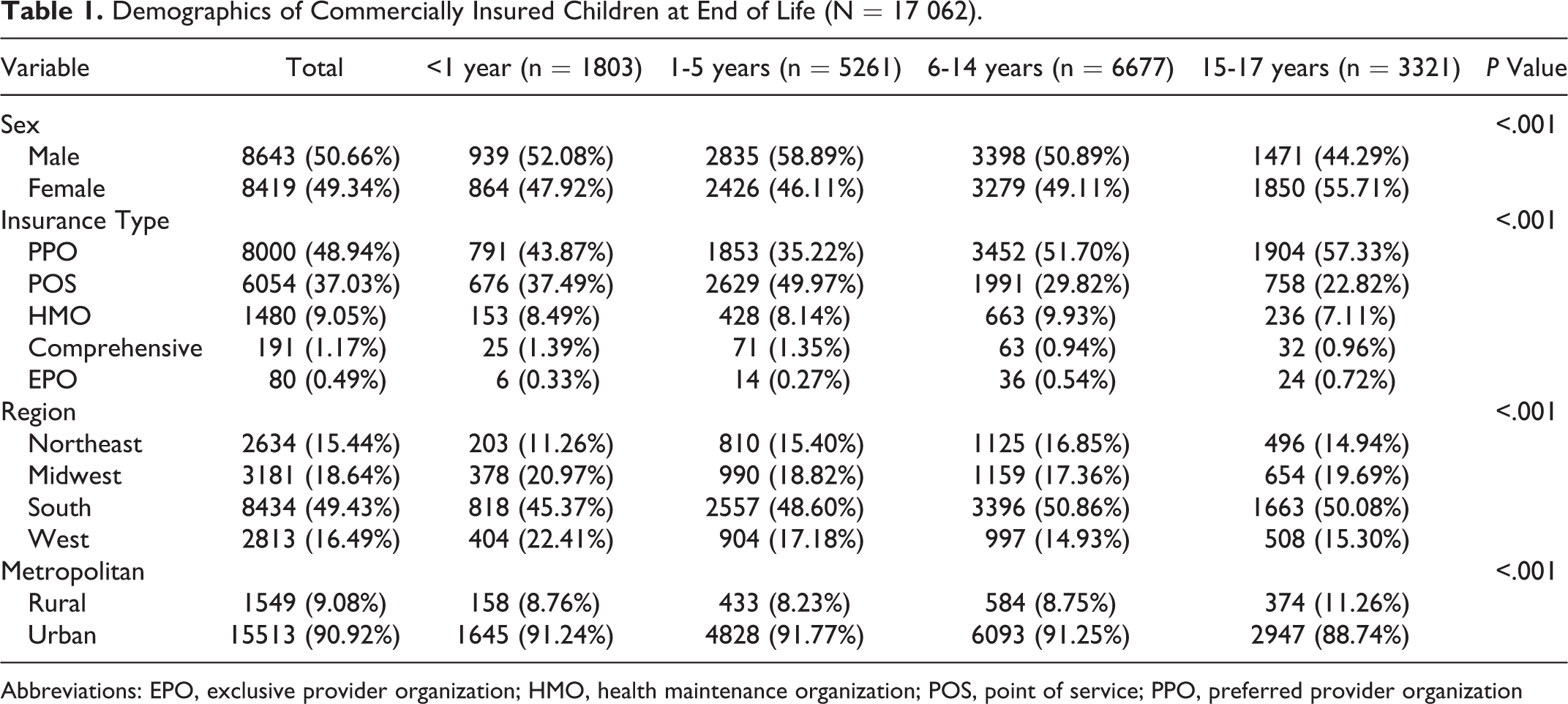
Abbreviations: EPO, exclusive provider organization; HMO, health maintenance organization; POS, point of service; PPO, preferred provider organization
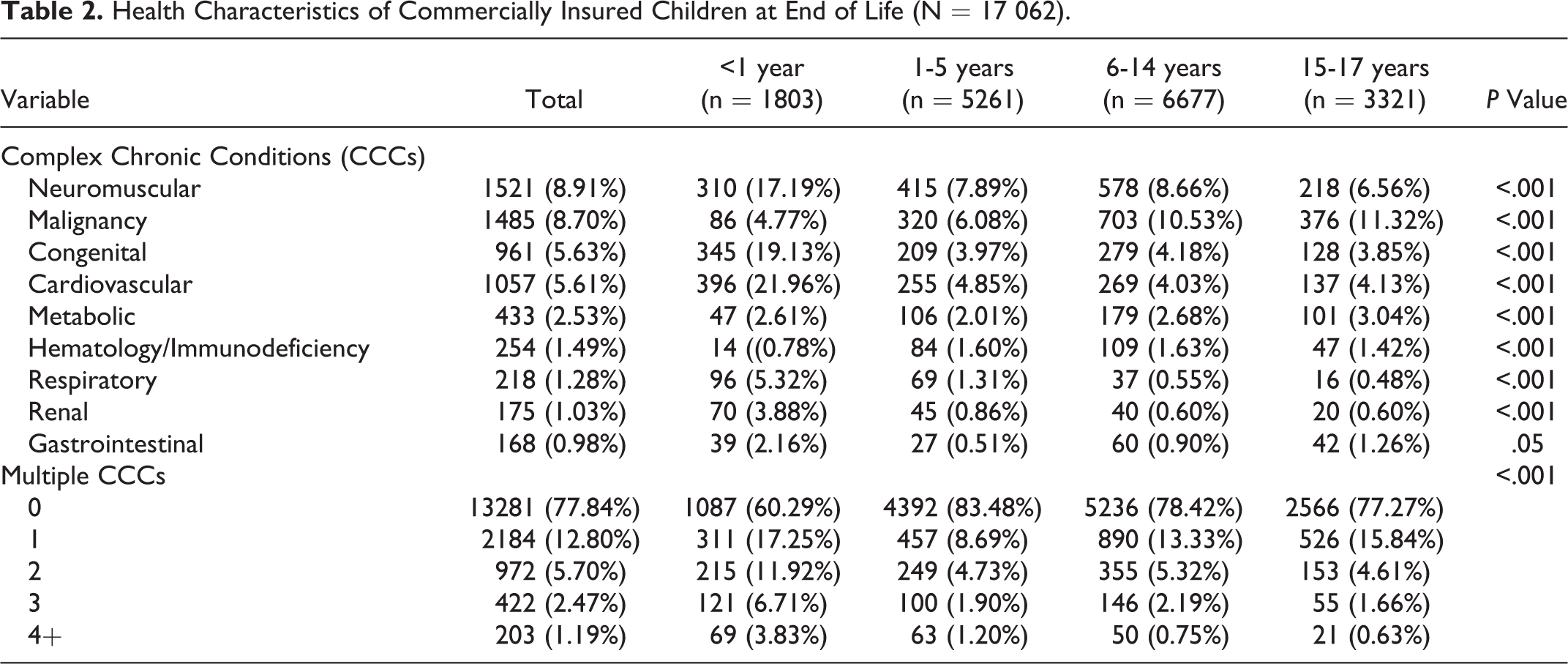
The health characteristics of the children are displayed in Table 2. Among all children in the sample, the most common CCC was neuromuscular problems (8.91%), followed by malignancies (8.70%). The least common was gastrointestinal conditions (0.98%). Less than a quarter of the children (22.16%) had one or more CCC. The frequency and patterns of clinical conditions varied by age-group. In the less than 1-year age-group, cardiovascular conditions were the most common (21.96%) CCC. Among 1 to 5-year-olds, neuromuscular conditions were the most frequent (7.89%), and among both children aged 6 to 14 years and adolescents aged 15 to 17 years, malignancies represented the most common health problem (10.53% and 11.32%, respectively). More than a third of infants <1 year had 1 or more CCC, compared to children aged 1 to 5 years with 17% and children aged 6 to 17 years with approximately 20%.
Health Characteristics of Commercially Insured Children at End of Life (N = 17 062).
Health care utilization data are listed in Table 3. For the entire sample, a majority (75.19%) of children were enrolled in hospice during 2010 to 2014. The mean hospice length of stay was 4.47 days. Most children (81.44%) had a primary care visit in their last year of life. A small percentage (8.06%) had 3 or more hospital admissions, while over a third used the emergency department at least once. There were significant differences across the age-groups on health care utilization. The average length of hospice stay ranged from 5 days for infants <1 year to 3.71 days for adolescents 15 to 17 years. Primary care visits were most common (87.50%) among children 15 to 17 years and least common among those less than 1 year (59.57%). Infants <1 year had the highest frequency of hospital readmissions (16.25%) with the lowest ED visits (28.67%), while children 1 to 5 years had the lowest hospital readmissions (6.98%) and the most frequent emergency department utilization (43.25%).
Health-Care Utilization of Commercially Insured Children at End of Life. (N = 17062)
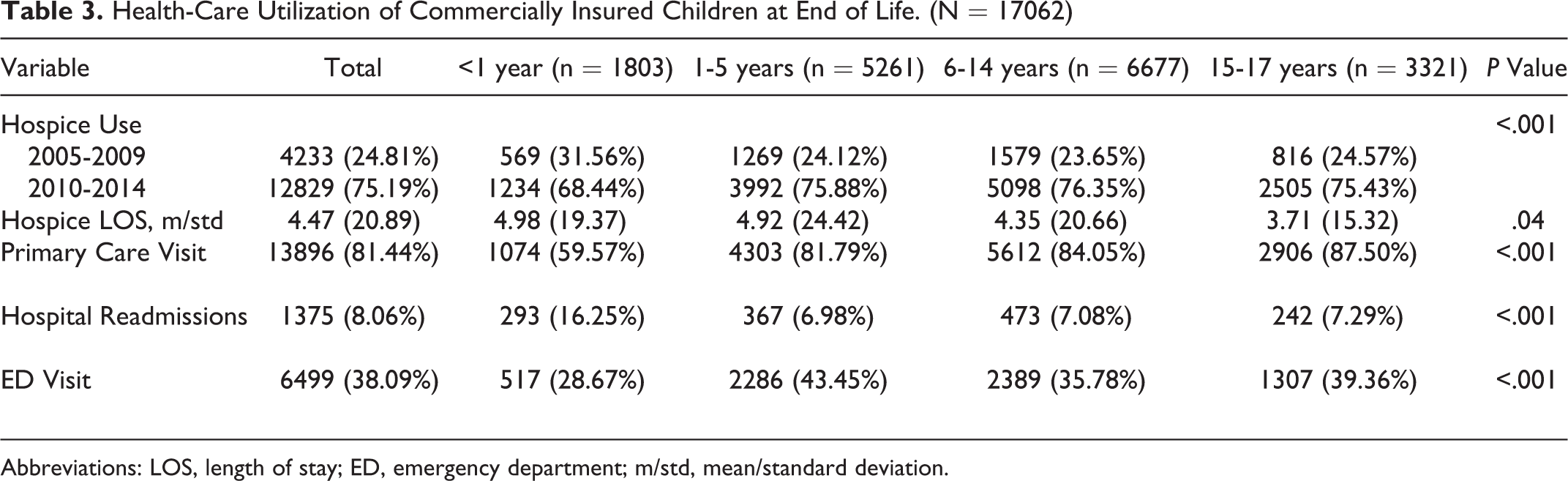
Abbreviations: LOS, length of stay; ED, emergency department; m/std, mean/standard deviation.
Table 4 contains information on the health care spending for children in the study. Average health care expenditure for commercially insured children was US$3686 per month or US$44232 annually. Coinsurance averaged US$72.00 monthly. Monthly copayments were on average US$17.00 and deductibles US$50.00. Infants <1 year consistently had the highest expenses compared to other children in the study. Coinsurance payments were over 3 times higher than the other children at US$193.00/month. Their average monthly expenditures were almost 4 times higher than the other age-groups. Their copayments (US$22.00/monthly) and deductibles (US$12.00/monthly) were the highest.
Health-Care Spending by Commercially Insured Children at End of Life (N = 17062).

Discussion
The primary goal of this research was to generate a profile of the demographic, health, utilization, and spending characteristics of commercially insured children who enrolled in hospice care at end of life. The study also sought to compare differences in characteristics across pediatric age-groups.
The findings from the study suggest that children, who enroll in hospice at end of life, have relatively flexible insurance coverage. Almost half of the children in the study were covered by a PPO. Although prior research has shown that commercial insurance is the most common type of insurance carried by children enrolled in hospice at end of life, 13 this is the first study to explore the different types of commercial insurance plans that these children participate in. The PPOs are currently the most common plan offered among US employers and have features that make them appropriate for children at end of life. 27 The PPOs offer flexibility. Participants in a PPO can choose from a large network of health care providers. Unlike an HMO or other plan types, the PPO allows participants to go outside the network for care and does not require a referral. 27 For children at end of life, the flexibility to seek out-of-network care, such as from a gastroenterologist, without a referral reduces administrative complications for parents, as they often must navigate the complex web of multiple providers for their children. These plans are designed for participants who utilize health care regularly and want to see specialists without getting a referral. 27 The PPOs often have a high deductible and premium, but for families of children at end of life that cost may be offset by the increased flexibility.
The health characteristics of children in the sample, especially the multiple CCC results, merit further investigation. It was surprising that between 60% and 83% of children in the study did not present with any CCC. The CCC classification system was developed in 2000 using diagnostic codes from children who died in the acute-care setting and has been used widely in pediatric end-of-life research. 25,26,28 –30 It is possible that diagnostic codes have changed in 18 years. Although the classification system has been refreshed from ICD-9 to ICD-10, 25 it might be time to revisit the validity of CCC codes against current diagnostic codes of children at end of life. Furthermore, the CCCs were originally developed in an acute-care setting, and this study was conducted among children enrolled in hospice. 26 It is possible that the diagnoses are different between those children who die in the hospital versus hospice. Future inquiry into the reliability of the CCC classification system should include testing in different settings.
The health care utilization findings were expected with children at end of life, who enrolled in hospice care. Children in this study averaged less than 5 days in hospice. This result was consistent with prior studies that examined hospice utilization among Medicaid beneficiaries, 9,16 including adolescents, 31 and those with intellectual disability. 32 Additionally, the finding that a majority of study participants visited their primary care physician in the last year of life was similar to the results of Lindley and Nageswaren 17 who found among Medicaid beneficiaries that over 60% of children had at least 1 visit to their primary care provider. It was interesting to note that rates of hospital readmissions and ED visits were relatively low for a population who was seriously ill. In studies among children who died while enrolled in Medicaid, the percentage of hospital readmissions ranged from 21% to 29% and ED utilization ranged from 52% to 72%. 11,12 Overall, these utilization findings suggest that pediatric patients at end of life are maintaining a relationship with their primary care physicians. Although the data did not allow for an investigation into case management for these children, it would be interesting to examine whether or not primary care physicians are actively managing intensive health care utilizations such as multiple hospital admissions and ED visits, as children prepare to enroll in hospice care. 11 Future research is clearly warranted.
The results highlighted the significant variation across the age-groups, with infants <1 year consistently exhibiting different health patterns and higher rates of health care utilization and spending compared to older children. Children <1 year, who enrolled in hospice, had a different pattern of health with cardiovascular and congenital diagnoses while experiencing the most CCCs. These infants had higher hospice length of stays combined with a high frequency of hospital readmission, when compared to older children. Care for infants was also the most expensive of all the age-groups. Others have drawn similar conclusions among this age-group at end of life. 7,18,33 One possible reason for the increase in days of hospice enrollment may reflect new end-of-life care delivery models for infants. Perinatal hospice and palliative care is an option for families who discover during pregnancy that their infant has a life-limiting condition but choose to continue the pregnancy. 34 Increased parental knowledge of perinatal hospice and palliative care may contribute to advanced care planning with earlier enrollment in hospice care. Research exploring the relationship between parental knowledge and hospice enrollment may provide critical evidence on mechanisms to improve hospice utilization for all children.
The study has several limitations inherent to research using administrative claims data because these data are collected for reimbursement rather than research purposes. First, some measures were not available in the claims data such as race/ethnicity. Thus, the study results, while interesting, may need to be interpreted with caution. Second, the data set included the last calendar year of life and did not include a comprehensive claims history. Third, the utilization and spending data may have been truncated for some children because the study data were date limited. Thus, hospice length of stay, for example, may be underreported. Finally, the study was conducted with commercial insurance data among children enrolled in hospice, which limits generalizability of the findings to other pediatric decedents.
Despite these limitations, the study has implications for hospice and palliative care clinicians caring for commercially insured children at end of life. The study found that there was a significant increase in hospice use from 2010 to 2014 (75%) compared to 2005 to 2009 (25%). From a policy perspective, section 2302 of the Affordable Care Act (Concurrent Care for Children) was enacted in 2010, and this provision allowed children to receive hospice care and ‘curative’ care simultaneously among Medicaid and Children’s Health Insurance Program (CHIP) enrollees. 35,36 Although Concurrent Care for Children was not mandated for commercially insured patients, the legislative intent of section 2302 was that there would be spillover for those covered by commercial health insurance. 35,37 To date, commercial insurance companies have not embraced concurrent care as a standard covered practice; however, anecdotal evidence suggests that nurses and other clinicians have been successful in requesting concurrent care for commercially insured pediatric patients on a case-by-case basis at end of life. Thus, hospice and palliative care clinicians caring for commercially insured children should be empowered to contact commercial insurance companies and request concurrent hospice and curative care for their patients.
Conclusions
In summary, the goal of the study was to describe the demographic, health, utilization, and spending characteristics of commercially insured children, who enrolled in hospice care at end of life, while comparing differences in characteristics across pediatric age-groups. Using data from a national, administrative database of commercial insurance claims, the findings from the study suggest that children have relatively flexible insurance coverage with a PPO. The results revealed that hospital readmissions and ED visits were relatively low for a population who was seriously ill. In addition, the results highlighted the significant variation across the age-groups, with infants <1 year consistently exhibiting different health patterns and higher rates of health care utilization and spending compared to older children. Given the current policy environment of Concurrent Care for Children, these findings have important clinical implications for hospice and palliative care clinicians.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jessica Keim-Malpass, PhD, RN is funded as a Translational Health Institute of Virginia Scholar.