
Abstract
Objective:
Studies suggest acupuncture improves cancer-related symptoms; however, it is unclear whether patient characteristics predict pain response. This study determined acupuncture’s effect on cancer-related pain and identified variables associated with pain response.
Methods:
A retrospective chart review included adult patients with cancer referred to palliative medicine and received acupuncture for pain management. Paired t tests compared differences in pain scores from pre- to postacupuncture. Clinically meaningful pain improvement was defined as ≥2-point reduction in pain score. Logistic regression was used to evaluate associations between patient characteristics and pain improvement.
Results:
One hundred seventy acupuncture treatments from 68 individual patients were studied. Significant reductions in mean pain scores were observed after the first treatment (−1.9 ± 1.8; P < .001) and across all treatments (−1.7 ± 1.9; P < .001). Multivariable analysis demonstrated clinically meaningful pain improvement with higher baseline pain scores (odds ratio [OR]: 1.79, 95% confidence interval [CI]: 1.44-2.22; P < .001) and stage III/IV disease (OR: 3.23, 95% CI: 1.11-9.40; P < .001). There were significant improvements in anxiety, depression, drowsiness, dyspnea, fatigue, nausea, and well-being after the first treatment and across all treatments (P < .001).
Conclusions:
Acupuncture improved cancer-related pain and other symptoms. Those with higher baseline pain scores and advanced disease were more likely to achieve significant pain reduction. Improved depression and fatigue were closely related to pain reduction. Further studies are needed to confirm pain response variables, establish durability, and develop a personalized approach to acupuncture.
Introduction
Pain is one of the most prevalent and burdensome symptoms affecting patients with cancer. Cancer and/or anticancer treatments such as surgery, chemotherapy, and radiation cause significant acute and chronic pain. In addition, pain is influenced by physiological, psychological, and behavioral factors. An estimated 50% of patients with cancer (and 75% with advanced disease) experience pain. Further, chronic pain develops in more than 40% of survivors. 1
Cancer-related pain treatment often includes opioid analgesics; however, up to 2 of 3 have inadequate pain relief and/or opioid-related adverse events. 2 Excessive opioid doses may increase abuse/addiction, accidental overdose, and/or respiratory depression. 3 The fear of opioid abuse/addiction and toxicity deters some from prescribing opioids and reduces patient compliance. Nonpharmacologic interventions such as acupuncture may be safer approaches to cancer-related pain.
Acupuncture is a traditional Chinese medicine technique that inserts thin needles into the skin at specific points for an analgesic response. 4 These are based on Western medical style, the location of the disease and/or pain (ie, local or distal) and symptoms. Local and distal points are based on their distance from disease site. Distal points are far from pain sites and target internal organs. 5 Acupuncture analgesia mechanisms are complex; some physiological effects are evident. It releases endogenous opioids in the brain-stem, limbic, and subcortical structures. 6 Needle insertion induces both local and peripheral changes (through axon reflexes). It also stimulates connective tissue, releases adenosine at the needle site, and increases local blood flow. 6
Randomized controlled trials suggest acupuncture reduces chronic neuropathic and postoperative pain in patients with cancer. 7 -9 One systematic review found insufficient evidence of efficacy for cancer pain. 10 Another concluded that acupuncture plus drug therapy significantly improved pain compared to drug therapy alone. 11 Overall, data suggest acupuncture is safe and may provide clinically meaningful pain and symptom improvements when used in addition to standard of care. 12 It is unknown whether any patient characteristics predict postacupuncture pain response. Because of this we assessed acupuncture’s effectiveness for cancer-related pain, identified patient characteristics associated with pain response, and determined its effect on other concurrent cancer-related symptoms in palliative medicine outpatients.
Methods
Study Design
The primary objective was to assess acupuncture effectiveness for cancer-related pain in patients with active cancer or a history of cancer (no current evidence of disease) and to investigate any association between patient characteristics and pain improvement postacupuncture. The secondary objective was to evaluate effects on anxiety, appetite, depression, drowsiness, dyspnea, fatigue, nausea, and well-being. The STRICTA (Standards for Reporting Interventions in Clinical Trials of Acupuncture) guidelines were followed. 13
Patient Population
Medical charts for all patients referred to the Levine Cancer Institute Section of Palliative Medicine who received acupuncture for pain between May 01, 2013, and December 31, 2015, were reviewed retrospectively. Laboratory and radiological investigations and scans were reviewed by the responsible physician before acupuncture. Patient demographics and disease characteristics at their first acupuncture treatment were collected for each patient.
The study was done in a naturalistic clinical practice setting, with a representative range of ambulatory patients with cancer having pain. Eligibility criteria included age ≥18 years old with any stage disease (or a history of cancer) who received acupuncture for pain and had completed the Edmonton Symptom Assessment Scale (ESAS) immediately before and after each treatment. Those with thrombocytopenia (platelets <50 000/mm3), bleeding disorders, supratherapeutic international normalized ratio ≥3, or neutropenia (absolute neutrophil count <1000/mm3) were ineligible. The ESAS screening at every visit was standard of care. This observational data collection study was approved by the institutional review board of Chesapeake and informed consent waived.
Acupuncture Treatment
All treatments were administered by a single palliative medicine physician (MD; author C.A.E.) certified in medical acupuncture, including a 300-credit hour course from the Helms Medical Institute. C.A.E. had over 3 years of certified medical acupuncture experience before the study. In addition to acupuncture, patients continued standard medical and supportive care, including medication management and psychosocial support. The frequency and number of treatments were determined by both the provider and the patient, sometimes limited by the patient’s transportation, prognosis, and transition to hospice care. Point selection was individualized for each patient based upon their specific conditions and symptoms (eg, anxiety, nausea, neuropathy). Local points were selected based on Western medical style and myofascial trigger points and distant ones on the channels theory of traditional Chinese medicine. The mean number of points per treatment was 13, with the most common being GV 24.5 and bilateral points LR 3, LI 4, SP 6, KI 3, ST 36, and BL 60.
Disposable, sterile, stainless steel, filiform needles (Seirin L type 0.2 mm diameter/40 mm length and J15 type 0.16 mm diameter/15 mm length) were used. Skin was swabbed with an alcohol pad beforehand. Needles were inserted 0.25 to 0.50 inches deep under the skin without further manipulation. No electrical stimulation was used. After insertion, needles were retained for a median of 28 minutes (range: 15-40 minutes). Patients were in a private clinic room throughout the procedure.
Assessment Tool
The ESAS is a validated assessment tool of numerical rating scales for the presence and severity of 9 common cancer symptoms: anxiety, appetite, depression, drowsiness, dyspnea, fatigue, nausea, pain, and well-being. Scores range from 0 to 10; 0 indicates no symptom and 10 a severe symptom. Each patient completed ESAS immediately before and after (within about 5 minutes) each acupuncture treatment (self-reported), and scores were collected by a clinic nurse.
Statistical Analysis
Descriptive statistics summarized patient characteristics and treatment outcomes. Differences in ESAS scores from pre- to posttreatment were calculated for all patients at each treatment. Clinically, meaningful pain improvement was defined as a reduction in at least 2 points from pre- to postacupuncture score. Paired t tests compared the differences in pre- to posttreatment ESAS scores at the first treatment. A variance component model evaluated ESAS score differences across all treatments. A generalized McNemar’s test compared pain subgroup changes based on severity (no pain, mild, moderate, or severe) from pre- to postacupuncture at the first and across all treatments. Univariate and multivariate logistic regression analyses of the primary end point (across all treatments) determined the association between clinically meaningful pain improvement and patient characteristics. These included number of acupuncture treatments, pain characteristics (neuropathic or nociceptive), baseline pain score (continuous variable), age (continuous variable), gender, race, stage, and primary tumor type. An overdispersion parameter accounted for repeated measures with multiple acupuncture treatments.
Univariate and multivariable logistic regression modeled the probability of clinically meaningful pain improvement with reduction in the other 8 ESAS symptoms. Pre- to postacupuncture benefit determined whether the probability of pain response was associated with other lower ESAS scores. Covariates in the models were quantitative reductions (ie, improvement) in each score.
Results
Demographic and disease characteristics for 68 adult patients with cancer are in Table 1. The median number of acupuncture treatments was 2 (range: 1-13); 81% had 1 to 3 and 19% ≥4. Table 2 summarizes the characteristics of 170 total acupuncture sessions among the 68 patients. The most common indications were neuropathic pain (58%), anxiety (38%), and back/neck pain (34%). The most frequent symptoms overall (ESAS score ≥1) were pain (92%), fatigue (87%), and decreased well-being (86%).
Baseline Patient Demographics.
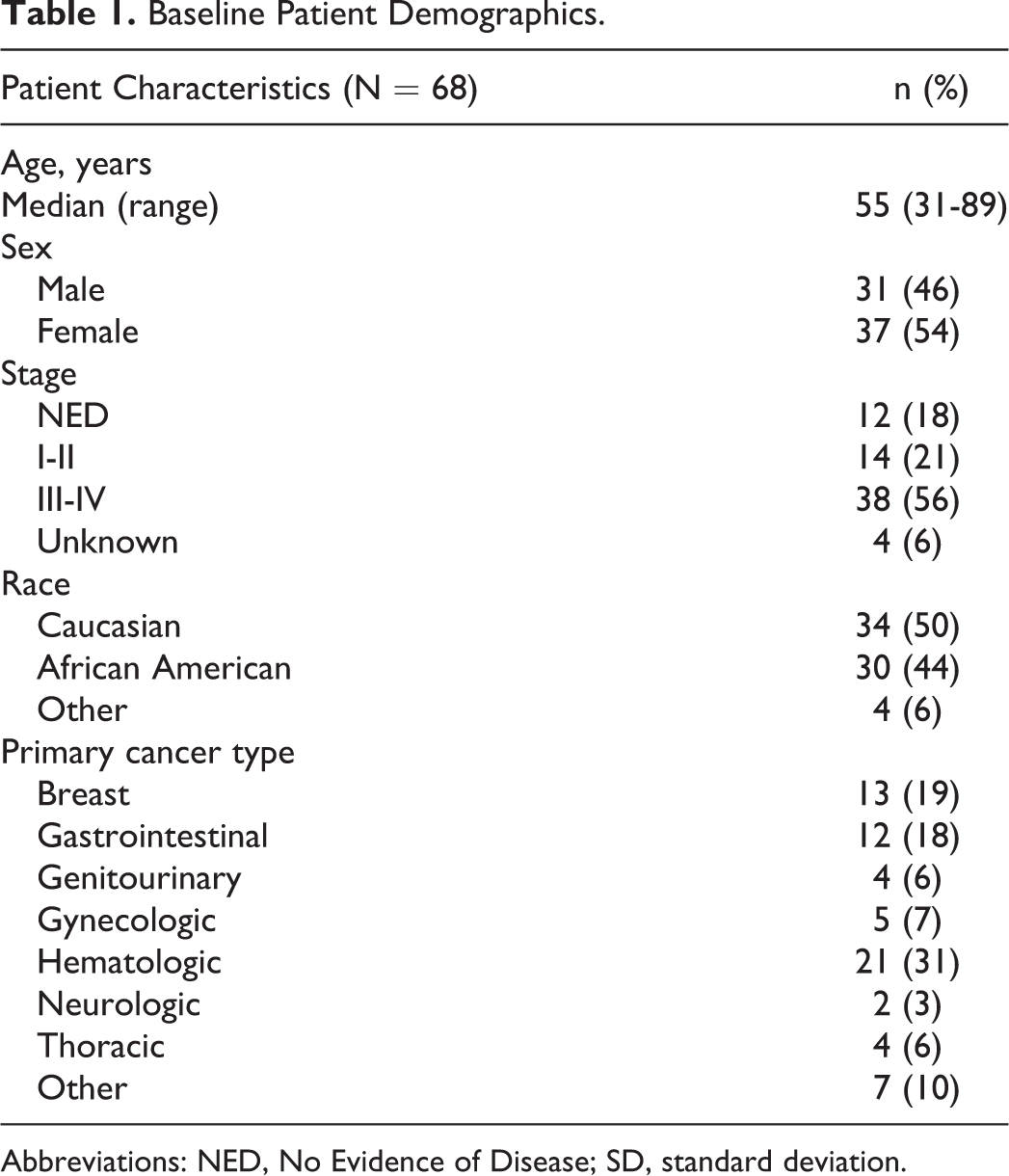
Abbreviations: NED, No Evidence of Disease; SD, standard deviation.
Indication for Acupuncture.a
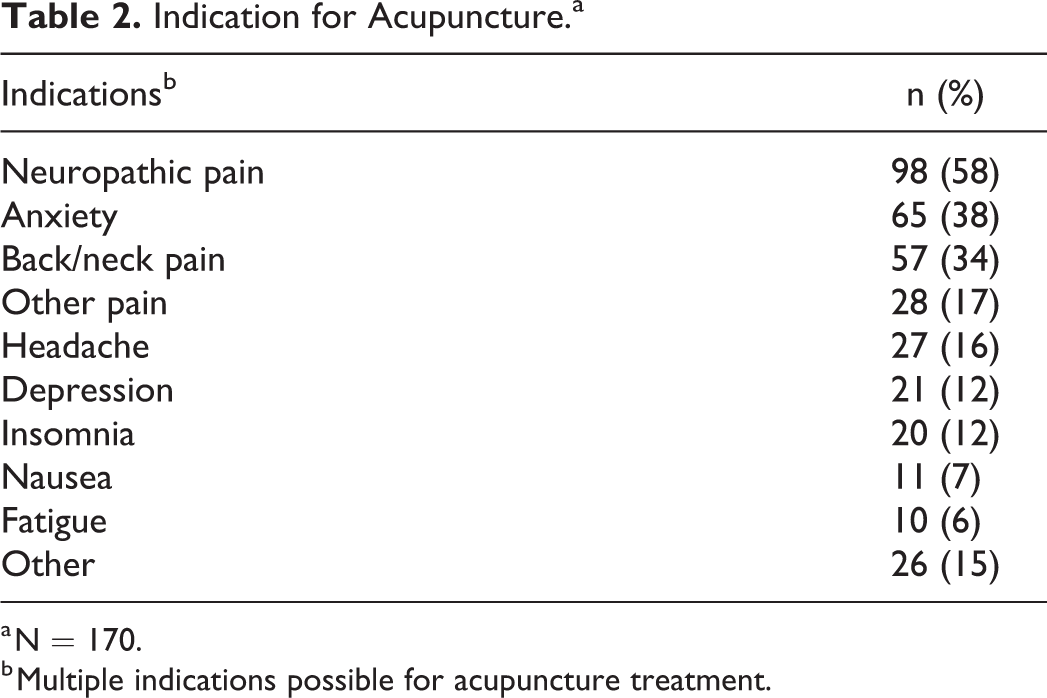
a N = 170.
b Multiple indications possible for acupuncture treatment.
Pain
Acupuncture resulted in statistically significant improvements (see Table 3) after the first and across all treatments (all P < .001). Clinically meaningful improvement (≥2-point decrease) was reported in 35 (51%) after the first and in 77 (45%) after all treatments. Importantly, the proportion with no or mild pain significantly increased after acupuncture, and those with moderate or severe pain significantly decreased (all P < .001).
Pain Score and Severity Pre- and Postacupuncture.
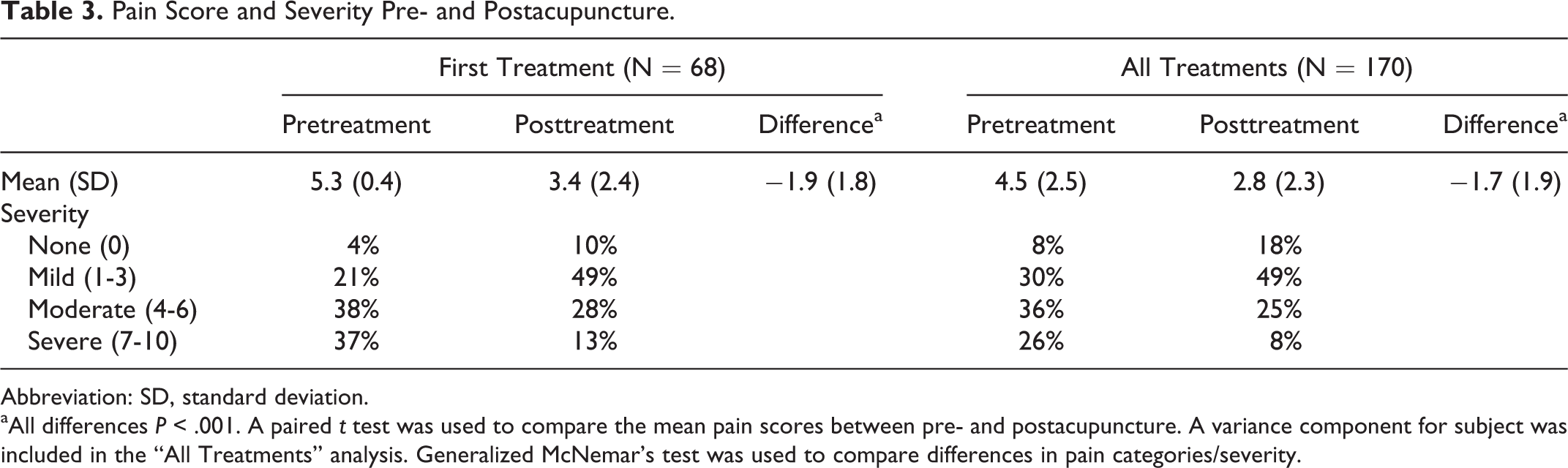
Abbreviation: SD, standard deviation.
aAll differences P < .001. A paired t test was used to compare the mean pain scores between pre- and postacupuncture. A variance component for subject was included in the “All Treatments” analysis. Generalized McNemar’s test was used to compare differences in pain categories/severity.
Critical factors associated with pain improvement
Results of the univariate and multivariable logistic regression analysis across all treatments (N = 170) are in Table 4. Univariate analysis demonstrated that disease stage was significantly associated with clinically meaningful reduction (P = .003). The percentage with pain reduction was 16%, 11%, and 73% for those with no disease, stage I-II, and stage III-IV, respectively. However, rates between those with no disease and active disease showed no significant difference (P = .54). Persons with higher baseline pain had greater odds of clinically meaningful improvement. Neuropathic pain had lower odds of clinically meaningful reduction than those without (P = .01). Those who had more treatments (≥ 4) had smaller odds of clinically meaningful benefit (P = .03). A trend was noted for less benefit with older age (P = .06) but gender, race, and tumor type were not significantly associated with lower pain.
Clinical Factors Associated With Pain Improvement After All Treatments.a
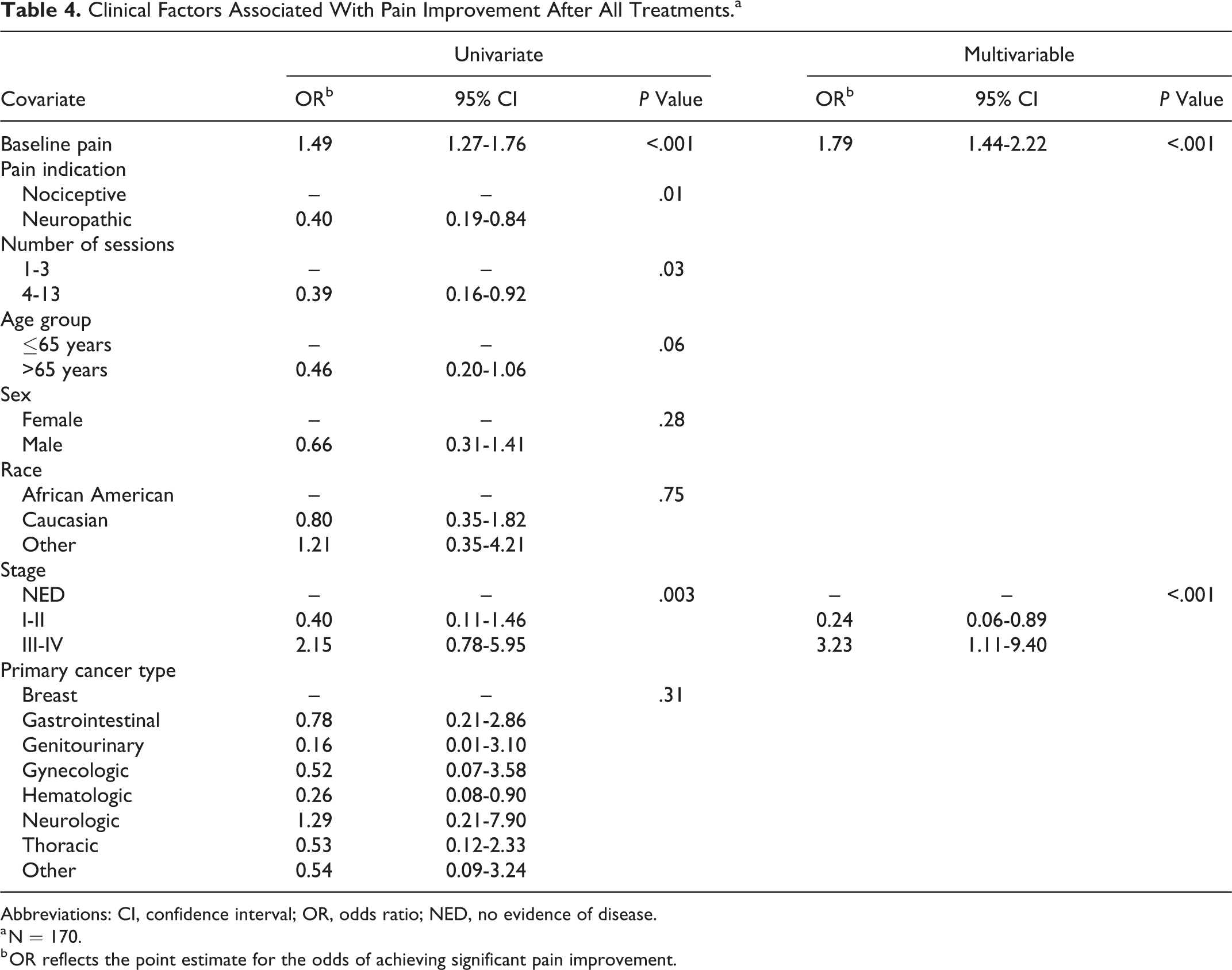
Abbreviations: CI, confidence interval; OR, odds ratio; NED, no evidence of disease.
a N = 170.
b OR reflects the point estimate for the odds of achieving significant pain improvement.
In multivariable analysis, higher baseline pain remained significantly associated with better odds of improvement. Additionally, those with stage I-II disease had less response than those with no disease but those with stage III-IV disease had higher odds of improvement than those with no disease.
Effects of Acupuncture on Other Symptoms
Table 5 summarizes the difference in ESAS scores for symptoms other than pain. There was a statistically significant (P < .001) improvement in anxiety, depression, drowsiness, dyspnea, fatigue, nausea, and well-being after the first and across all treatments.
Effects of Acupuncture on Other Symptoms.
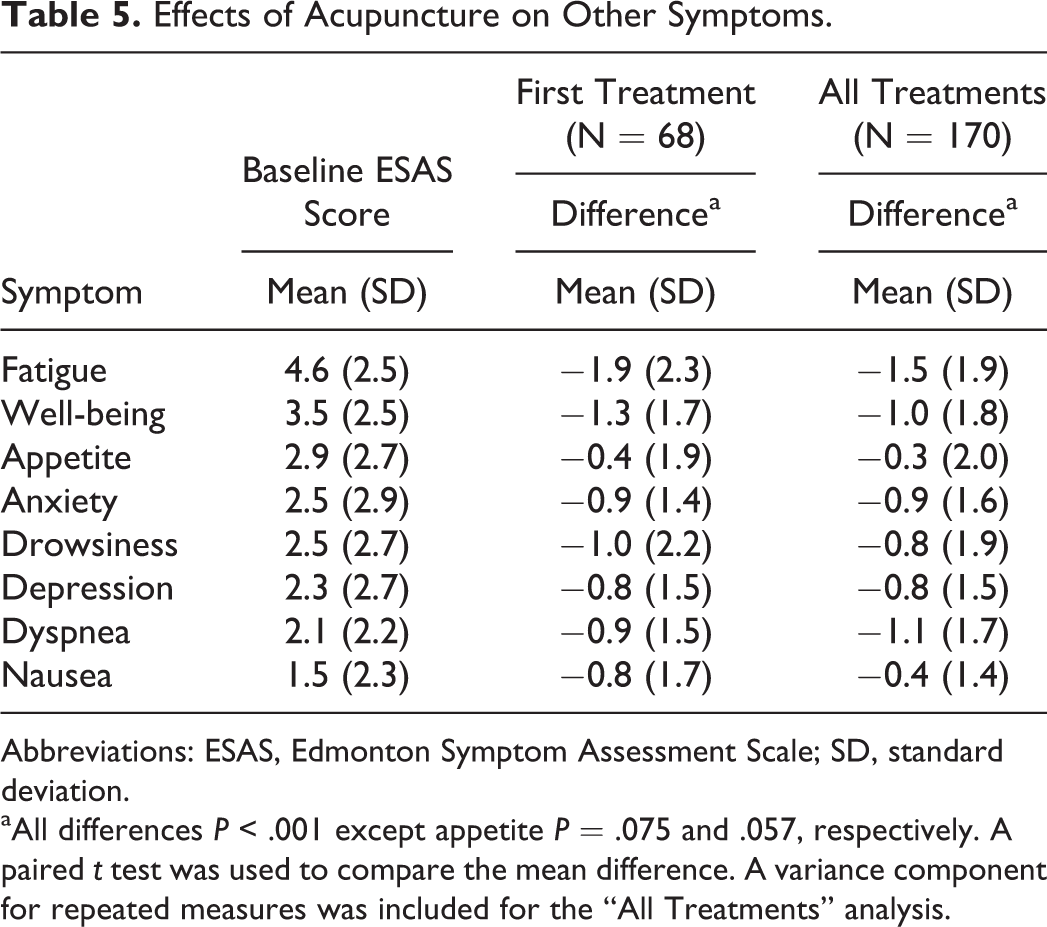
Abbreviations: ESAS, Edmonton Symptom Assessment Scale; SD, standard deviation.
aAll differences P < .001 except appetite P = .075 and .057, respectively. A paired t test was used to compare the mean difference. A variance component for repeated measures was included for the “All Treatments” analysis.
Next, we assessed whether quantitative improvements in each symptom were associated with clinically meaningful pain improvement. Univariate analysis across all treatments (N = 170) demonstrated reduction in 7 of the 8 symptoms and was significantly associated with clinically meaningful (≥2 point) pain improvement—the only exception was appetite (Table 6). Among the 7 symptoms, the magnitude of association was highly consistent; the odds ratios ranged from 1.24 to 1.55 (higher odds of pain benefit with reduction in each individual symptom). In the multivariable analysis, only 2 symptoms were independently associated with pain improvement: depression and fatigue (P = .003).
Association Between Improvement in Other Symptoms and Pain.
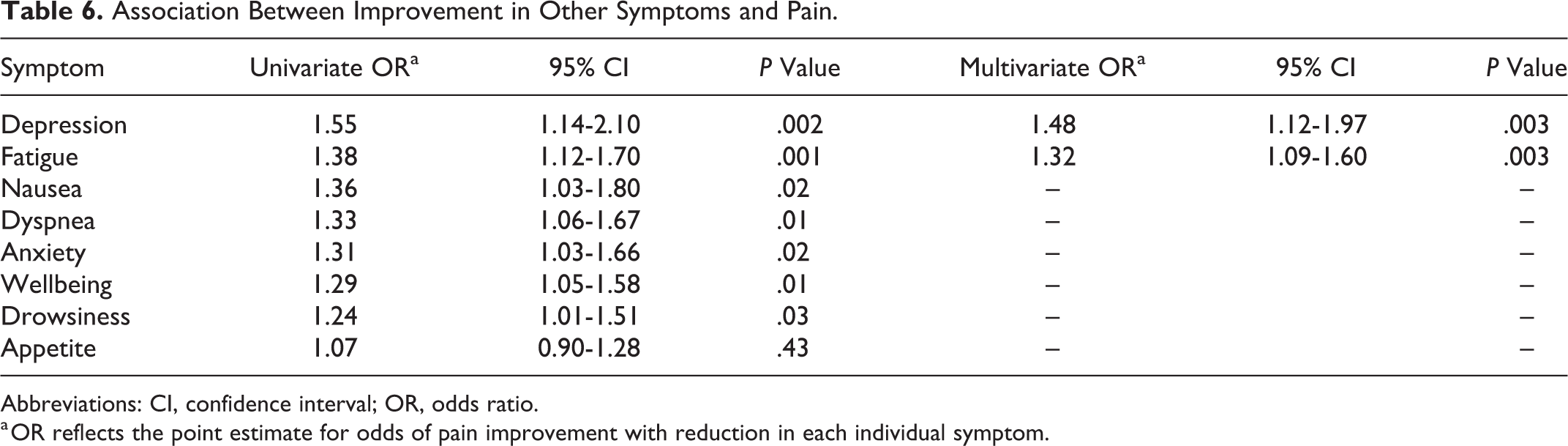
Abbreviations: CI, confidence interval; OR, odds ratio.
a OR reflects the point estimate for odds of pain improvement with reduction in each individual symptom.
Discussion
This study supported acupuncture effectiveness as part of a multidisciplinary approach to improve cancer-related pain and symptoms. There were significant benefits in pain scores immediately after the first treatment and across all treatments. Clinically, meaningful pain reduction was significantly associated with higher baseline pain and more advanced disease stage. Further, there were positive changes in anxiety, depression, drowsiness, dyspnea, fatigue, nausea, and well-being. Improvements in fatigue and depression scores also correlated with significant pain reductions.
Acupuncture effectiveness has been noted in other cancer pain studies. A randomized study in aromatase inhibitor-associated pain in breast cancer reported significant improvements for worst pain, pain severity, pain-related interference, and physical well-being in the acupuncture group (n = 20) compared with sham acupuncture (n = 18). 14 Another randomized 226 early patients with breast cancer on aromatase inhibitors and found more (58%) experienced clinically meaningful pain improvement (≥2-point reduction) than sham acupuncture (33%). 15 In postoperative pain, the combination of acupuncture, massage, and standard of care (n = 93) was associated with significant pain and depression improvements compared to standard of care alone (n = 45). 9 Auricular acupuncture for neuropathic cancer pain significantly improved pain intensity scores in the acupuncture group (n = 29) compared to sham needles (n = 30) or sham ear seeds (n =31), 7 suggesting targeted acupuncture is effective.
Univariate analyses identified pain improvement was associated with higher baseline pain scores, pain type (nociceptive), later disease stage, and total number of acupuncture treatments. Although pain type and number of treatments were not retained in the final multivariable model, they could be important and should be investigated further in larger studies. The potential loss of acupuncture effect over time in those who received multiple treatments could be due to exhaustion of endogenous opioids or trafficking of opioid receptors, similar to opioid tolerance mechanisms. The proposed mechanisms of neuropathic pain, including sensory axonal damage and reduced amplitude of sensory nerve action potential, 16 suggest this pain type may be responsive to acupuncture; however, this was not evident in our results potentially due to downregulation of mu receptors or induction of receptor tolerance. 17,18
Multivariable analysis demonstrated that those with greater baseline pain severity were more likely to achieve clinically meaningful reduction. This may be because those with lower baseline pain scores have a more restricted range for clinically meaningful improvement. 19 There appeared to be no pain improvement difference between persons with no disease versus active disease. Those with advanced disease were more likely to achieve clinically meaningful pain reduction than stage I-II or no disease. Although advanced and metastatic disease was associated with increased cancer-related pain, there was no significant correlation between baseline pain and disease stage. Nonetheless, it is possible that in advanced disease severe pain might benefit more from acupuncture, similar to the higher likelihood of pain improvement with greater baseline pain.
In addition to improved pain, anxiety, depression, drowsiness, dyspnea, fatigue, nausea, and well-being also improved. Similarly, a study of 25 patients observed statistically significant improvements in anxiety, fatigue, pain severity, and pain interference after acupuncture. 20 Another study in 32 patients with cancer reported significantly less anxiety, depression, fatigue, and pain after acupuncture. 21 In 26 palliative care patients, acupuncture significantly improved anxiety, depression, dyspnea, nausea, pain, tiredness, and well-being. 22 These data, like our findings, support acupuncture not just for pain but for multiple cancer symptoms.
There was a high degree of coherence between reductions in anxiety, depression, dyspnea, nausea, tiredness, and well-being scores with pain improvement. This suggested that acupuncture pain “responders” improved in more than one symptom. There was a high symptom collinearity as the multivariable model demonstrated that improvement in 2 symptoms (depression and fatigue) was independently associated with pain reduction. This suggests that acupuncture may be effective for multiple symptoms simultaneously, particularly depression, fatigue, and pain. The associated reduction in these symptoms may be direct or indirect and prior studies suggest a symptom cluster exist. 23,24 Meta-analyses from randomized trials have also demonstrated that acupuncture may improve cancer-related fatigue. 25,26
Limitations to the study included lack of a control arm or comparator due to the study’s retrospective nature and potential for placebo response. Additionally, disease progression data during acupuncture and concomitant opioid/adjuvant therapies were not available. Concomitant pain medications may have confounded the pain scores. The ESAS does not directly characterize the type, nature, or location of pain. Additionally, symptom scores were assessed immediately after acupuncture, and the duration of effect unknown, a common limitation of many acupuncture studies. One study suggested that longer acupuncture duration provides more sustainable analgesia, but the duration is unknown. 27 Finally, the relatively small sample size and population heterogeneity may limit generalizability to other oncology and nononcology populations. Focused prospective studies based on tumor characteristics and/or presenting symptoms may improve generalizability to specific populations most likely to benefit. This was a real-world analysis of cancer outpatients receiving acupuncture as part of a multidisciplinary palliative medicine approach to cancer-related pain and other symptoms. High-quality medical acupuncture certificate programs are available for palliative medicine physicians and may broaden the scope of nonpharmacological management of cancer-related symptoms. Future studies with comprehensive patient-reported outcomes should evaluate pain characteristics likely to benefit from acupuncture, durability, and any opioid-sparing effect.
Conclusions
Acupuncture was effective in reducing cancer-related pain and other symptoms, including anxiety, depression, drowsiness, dyspnea, fatigue, nausea, and improving well-being. Higher baseline pain score and more advanced disease were significant predictors of clinically meaningful pain benefit and may help to further individualize acupuncture therapy. Improved depression and fatigue were closely related to pain reduction. Future studies of acupuncture in cancer should evaluate patient characteristics associated with symptom improvement, response durability, acute versus chronic cancer pain, and any opioid-sparing effect.
Footnotes
Authors’ Note
K.R.M. and J.N.P. contributed equally to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.