
Abstract
Objective:
Polypharmacy (PP) is a burden in elderly patients with cancer pain; however, risk factors for PP remain unclear. The purpose of this study was to investigate the risk factors for PP in this patient population.
Methods:
We retrospectively reviewed the medical charts of patients aged ≥65 years with cancer pain who were treated at Osaka University Hospital between February 2014 and June 2016 according to the World Health Organization 3-step ladder for cancer pain relief. We defined PP as ≥5 medications and conducted exploratory research to examine the association between PP and patient characteristics. Performance status (PS) was estimated according to the Eastern Cooperative Oncology Group system and is categorized as good PS (0-1) and poor PS (2-4).
Results:
We reviewed 206 patients (122 men and 84 women) with a median age of 71 years (range, 65-89 years) and found that 174 patients (84.5%) had PP. In multivariate logistic analysis, PP was significantly associated with an increased number of comorbidities (odds ratio [OR]: 4.93, 95% confidence interval [CI], 2.57-11.42, P < .001), poor PS (OR: 4.50, 95% CI, 1.06-31.68, P = .039), and administration of an anticancer or molecular targeted drug (OR: 2.78, 95% CI, 1.13-7.16, P = .025).
Conclusions:
An increased number of comorbidities, poor PS, and administration of an anticancer or molecular targeted drug were considered risk factors for PP in elderly patients with cancer pain. Sharing these risk factors with medical staff will help reduce the occurrence of problems associated with PP.
Keywords
Introduction
Elderly patients with cancer pain suffer from various distress. The medication burden of patients is one of them. To alleviate the pain and adverse events associated with cancer treatment, these patients often take a number of drugs. Polypharmacy (PP) is a burden in elderly patients with cancer. 1,2 Moreover, the prevalence of PP in elderly patients is a risk factor for adverse drug reactions. 3 Kotlinska-Lemieszek et al 4 conducted a cross-sectional study in patients with PP and found that 2282 patients with advanced cancer with pain treated according to the World Health Organization (WHO) 3-step ladder for cancer pain relief were included. Patients were taking a mean number of 7.8 drugs, and approximately 45% of patients received unnecessary or potentially inappropriate medication (PIM). Furthermore, PP is thought to be associated with increased mortality. 5,6 However, little is known about the criteria for stopping medications in patients using an opioid. It is important to identify risk factors for PP in order to implement the appropriate use of medications. The purpose of this study was to investigate risk factors for PP in elderly patients with cancer pain.
Methods
Participants
We retrospectively reviewed the medical charts of patients aged ≥65 years with cancer pain treated according to the WHO analgesic ladder with step III opioids between February 2014 and June 2016 at Osaka University Hospital. Opioid-treated patients for other symptoms including dyspnea were excluded. Patients whose start time of opioid treatment was unknown were also excluded.
Measures
We defined PP as ≥5 medications and conducted exploratory research to examine the association between PP and patient characteristics. We investigated all drugs taken on the day of starting opioid administration by patients with cancer. To determine risk factors for PP, we investigated sex; age (year); opioids (morphine, oxycodone, fentanyl, tapentadol); concomitant drug; number of medications; PIM; performance status (PS); body mass index (BMI); comorbidities including hypertension, insomnia, diabetes mellitus and hyperlipidemia; number of comorbidities; and administration of an anticancer or molecular targeted drug. The PIM use was categorized based on the Screening Tool of Older People’s Prescription (STOPP)/Screening Tool to Alert to Right Treatment (START) criteria version 2. 7,8 The PS was estimated according to the Eastern Cooperative Oncology Group system and is categorized as good PS (0-1) and poor PS (2-4). Medication class was based on the WHO Guidelines for Anatomic Therapeutic Class Classification and Defined Daily Dose assignment. 9
Statistical Analysis
Continuous data including age, number of comorbidities, and BMI were summarized as the median (range). Univariate and multivariate logistic regression analyses were used to investigate the relationship between patient characteristics and PP. P values <.05 were considered statistically significant. All statistical analyses were performed using JMP 13 software (SAS Institute, Cary, North Carolina).
Results
Baseline Characteristics
In total, 218 patients with cancer pain were administered an opioid. Twelve patients were excluded because the start time of opioid treatment was unknown. Therefore, a total of 206 patients were included in the study. Patient characteristics are shown in Table 1. The median age of the patients was 71 years (range, 65-89 years), and the number of patients who received ≥5 medications was 174 (84.5%) patients. The median number of comorbidities was 1 (range, 0-6). The most prevalent comorbidities were hypertension (35.4%), insomnia (27.7%), diabetes mellitus (17.0%), and hyperlipidemia (13.6%). The most prevalent cancer diagnoses were pancreas (19.9%) and lung (10.7%).
Patient Characteristics.a
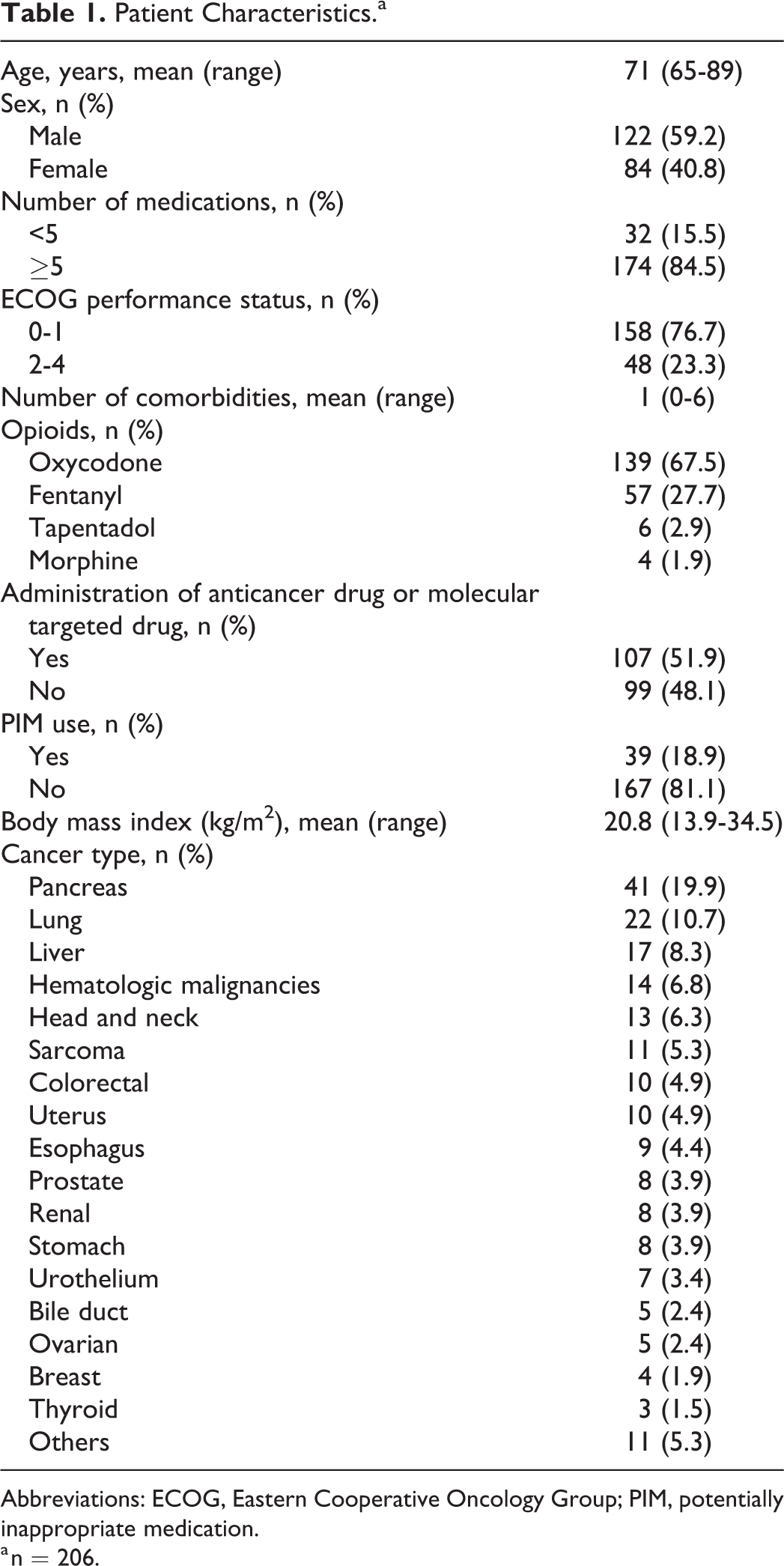
Abbreviations: ECOG, Eastern Cooperative Oncology Group; PIM, potentially inappropriate medication.
a n = 206.
Medications Other Than Step III Opioids
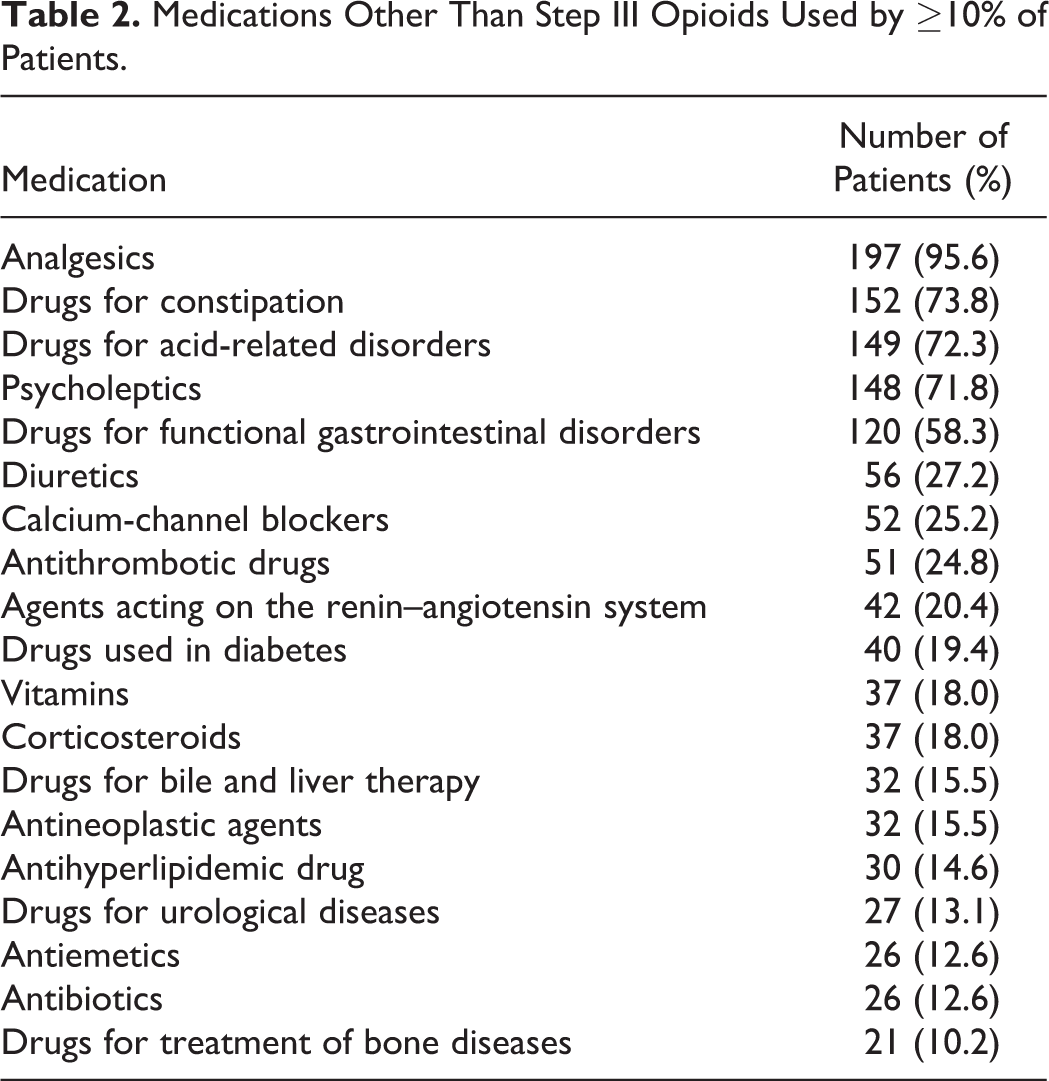
The most common medications other than step III opioid were analgesics (95.6%), drugs for constipation (73.8%), drugs for acid-related disorders (72.3%), and psycholeptics (anxiolytics, hypnotics, antipsychotics, 71.8%; Table 2).
Medications Other Than Step III Opioids Used by ≥10% of Patients.
Potentially Inappropriate Medication Use
The PIM was determined by the STOPP criteria listed in Table 3. A total of 39 (18.9%) patients were prescribed PIMs, of who 13 had duplicate drug class prescription; 6 of these 13 patients were prescribed tramadol and a step III opioid. Seven (3.4%) patients were found to have prolonged use (>1 week) of first-generation antihistamines, and 6 (2.9%) patients were prescribed nonsteroidal anti-inflammatory drugs with warfarin.
Potentially Inappropriate Prescriptions as Determined by STOPP Criteria.
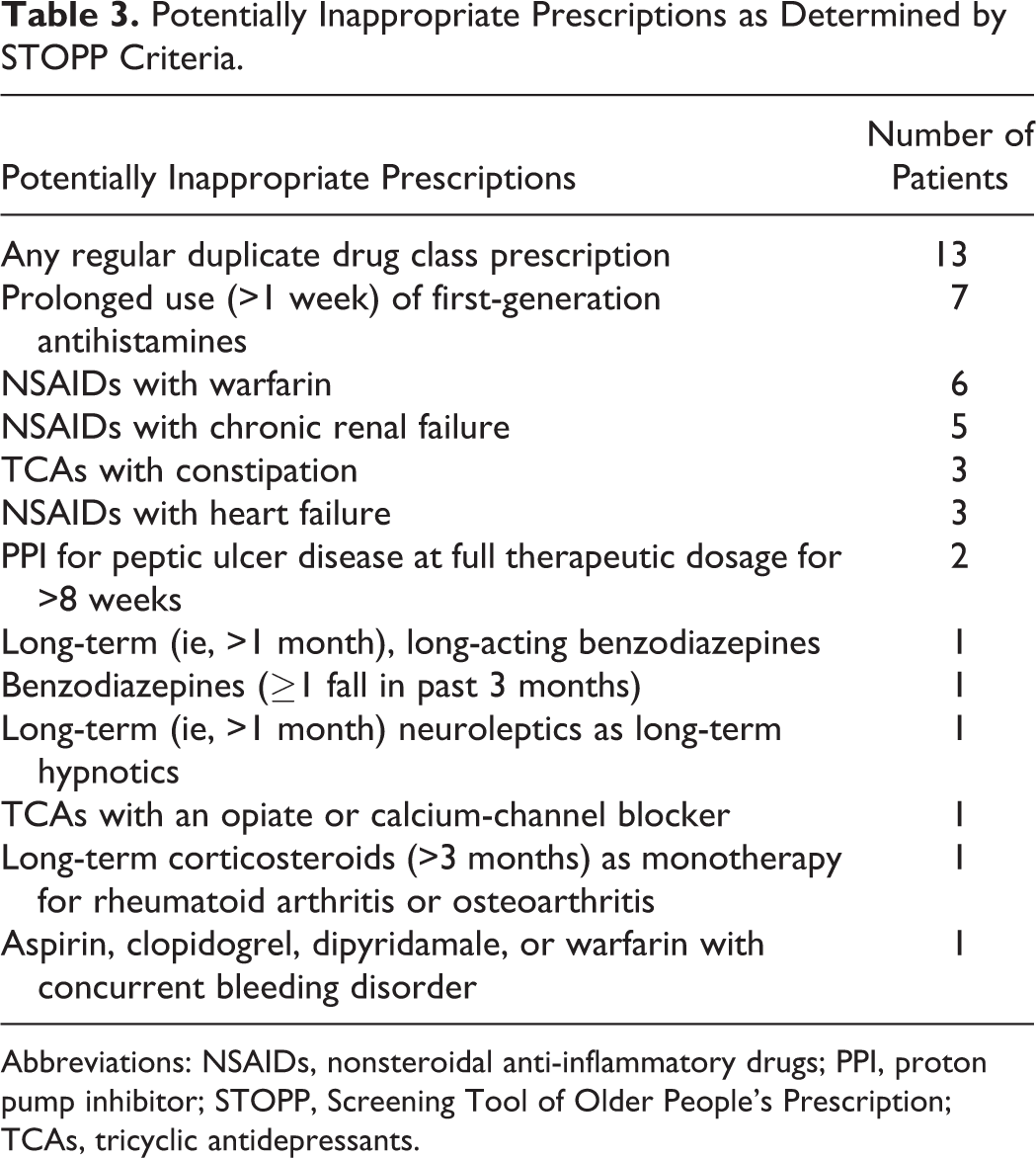
Abbreviations: NSAIDs, nonsteroidal anti-inflammatory drugs; PPI, proton pump inhibitor; STOPP, Screening Tool of Older People’s Prescription; TCAs, tricyclic antidepressants.
Risk Factors for PP
We performed univariate and multivariate logistic regression analyses (Table 4). In the multivariate logistic regression analysis, PP was significantly associated with an increased number of comorbidities (odds ratio [OR]: 4.93, 95% confidence interval [CI], 2.57-11.42, P < .001), poor PS (OR: 4.50, 95% CI, 1.06-31.68, P = .039), and administration of an anticancer or molecular targeted drug (OR: 2.78, 95% CI, 1.13-7.16, P = .025). In the univariate logistic regression analysis, the OR of the number of comorbidities and poor PS was approximately the same as that in the multivariate logistic regression analysis.
Univariate and Multivariate Analysis of Risk Factors for PP (n = 206).
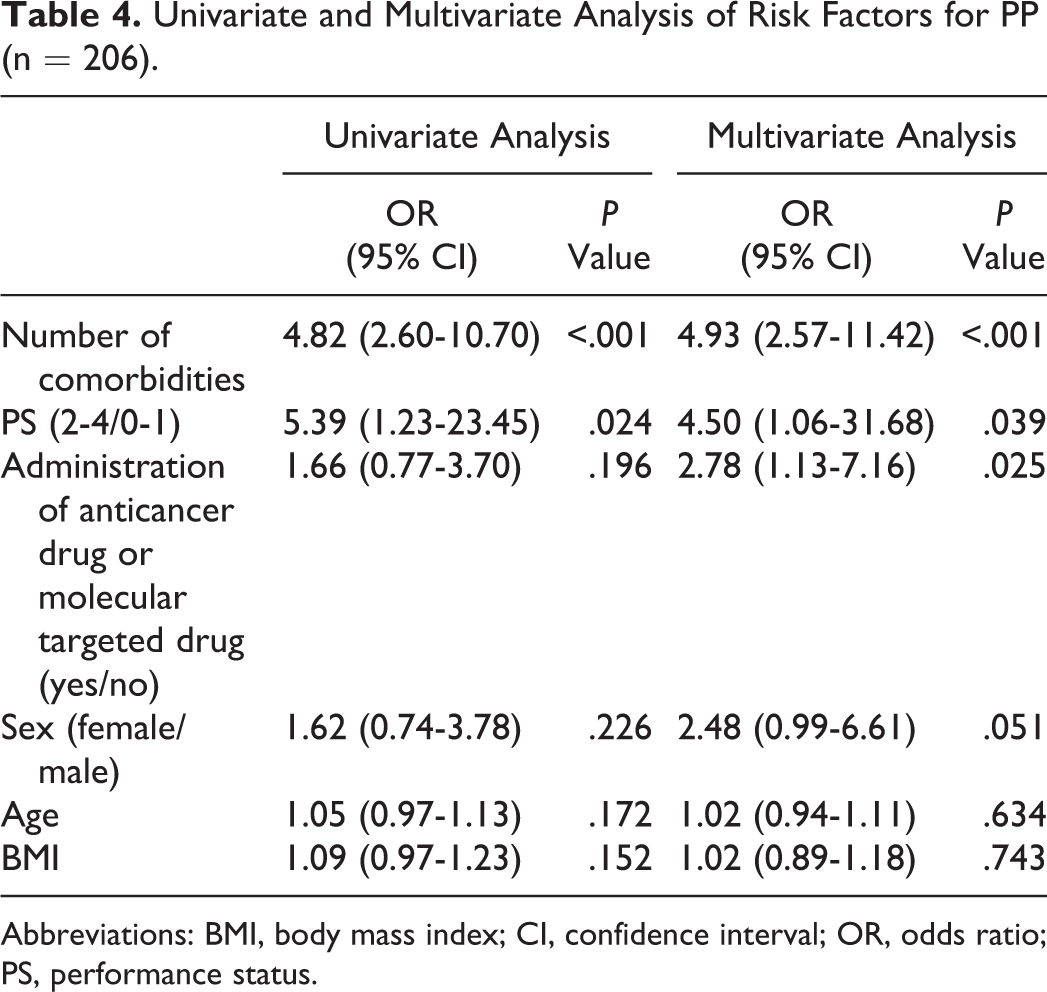
Abbreviations: BMI, body mass index; CI, confidence interval; OR, odds ratio; PS, performance status.
Discussion
This study showed that the increased number of comorbidities, poor PS, and administration of an anticancer or molecular targeted drug were risk factors for PP in elderly patients with cancer pain. In this study, 84.5% of patients received ≥5 medications. Depending on the definition of PP, the prevalence of PP in patients with cancer ranges from 13% to 96%. 10 -16 Turner et al 16 reported the optimal PP cut point that correlates with a variety of adverse events in elderly patients with cancer. The authors suggested that no single PP cut point is optimal for predicting multiple adverse events. However, they also suggested that it is reasonable to use the common PP definition of 5 or more medications for identifying “at-risk” patients for medication review. Other studies have also reported a definition of PP as 5 or more medications. 14,17 -19
In this study, multivariate logistic regression analysis showed that PP was significantly associated with an increased number of comorbidities. Nightingale et al 19 found that elderly patients who took more than 5 medications were significantly more likely to have a greater number of comorbidities. Prithviraj et al 13 also reported that PP was significantly associated with an increased number of comorbidities. An increase in the number of medications used also raises the possibility of increased drug–drug interactions (DDIs) and PIM use. Alkan et al 20 reported that nearly one-third of elderly patients are exposed to severe DDIs and PIMs. Opioids and other analgesics have DDIs, for which the risk of adverse events is sometimes underestimated. Therefore, pharmacists should pay particular attention to the prescription of medications in elderly patients with cancer with multiple comorbidities and should avoid DDIs if possible.
We also found that poor PS was associated with risk of PP. Some reports have shown that poor PS is associated with PP in elderly patients with cancer. 14,19 On the other hand, Kierner et al 15 suggested that the poorer the patient’s condition, the fewer the medications prescribed at 2 specialized wards (oncology and palliative care). The authors reported that patients with a poor PS or with terminal disease had significantly fewer prescribed medications because chemotherapy was frequently used at the oncology ward and rarely used at the palliative ward. Relationship between poor PS and PP is still controversial.
Finally, we found that the administration of an anticancer or molecular targeted drug was another risk factor for PP. Some reports have shown that the administration of an anticancer or molecular targeted drug was the cause of DDIs. 21 -24 Popa et al 25 reported a significant association between potential drug interactions and risk of nonhematological toxicity from chemotherapy in older patients with cancer. However, Maggiore et al 26 reported that adverse events from chemotherapy were not related to PP. It is important to conduct an individualized medicine to each patient because there are some necessary supportive care to relieve the adverse events.
We investigated all drugs taken on the day of starting opioid administration by patients with cancer because earlier confirmation of concurrent administration using STOPP/START criteria was important. Not only opioid administration but also administration of laxatives and prophylactic antiemetic drugs can be the cause of PIM, including duplicate drugs prescription and increase in adverse events. In fact, duplicate drugs administration of metoclopramide and prochlorperazine was conducted by 3 out of 13 patients. Seven patients were found to have prolonged use (>1 week) of first-generation antihistamines. It is possibile that combined use of opioid and first-generation antihistamines increased adverse effects of somnolence. Therefore, we defined PP cut point as 5 or more medications considering some studies 14,16 -19 in order to stop PIM use and minimize the number of medications. Moreover, Whitman et al 27 reported that pharmacist-led deprescribing intervention using geriatric medication screening tools (including STOPP/START criteria) may lead to improved patient outcome and cost-savings. Pharmacists can contribute to deprescribing by conducting earlier confirmation of concurrent administration and considering the need for PIM use.
There were some limitations in this study. First, 6 patients used 2 kinds of opioids, which were categorized as PIM from STOPP/START criteria. Guarald et al 28 published that not only STOPP/START criteria but also Beers criteria 29 were used for defining PIM. LeBlanc et al 30 reported that Beers and other criteria may be difficult to apply in patients with advanced cancer. It is doubtful that duplicate opioid prescription was PIM in this population. However, there are no specific guidelines for defining PIM in the palliative care setting. Therefore, guidelines or appropriate criteria should be developed for PIM in elderly patients with cancer. Second, we could not assess frailty because our study was retrospective. Some reports have shown that frailty in patients with cancer is associated with PP. 14,31 Additional studies are needed to investigate the relationship between frailty and PP in elderly patients with cancer pain. Third, we could not investigate the relationship between PP and adverse outcome in elderly patients with cancer pain. The PP can cause of adverse events. Therefore, a further study is needed to elucidate it.
In conclusion, an increased number of comorbidities, poor PS, and administration of an anticancer or molecular targeted drug were found to be risk factors for PP in elderly patients with cancer pain. The appropriate use of medications can lead to cost benefits and patient safety. However, there are many problems that cannot be solved by pharmacists alone, as current therapies can be very complicated. Therefore, sharing these risk factors with medical staff will help reduce the occurrence of problems associated with PP.
Footnotes
Authors’ Note
Isao Yokota is now affiliated with Department of Biostatistics, Graduate School of Medicine, Hokkaido University, Hokkaido, Japan.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Isao Yokota has received speaker fee from Chugai Pharma CO., Ltd.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.