
Abstract
Purpose:
The purpose of the study was to evaluate the impact on pain management by multidisciplinary palliative care team (mPCT) and the team pharmacist.
Methods:
Patients who were admitted to palliative care unit (PCU) for at least 7 days between April 2014 and December 2015 were included. The mPCT consisted of a physician, a pharmacist, nurses, and non-clinical support staff. The team was on charge of pain management of patients who were admitted to PCU. Pain intensity was assessed at 3 time points in each patient; 1 week before PCU admission (day −7), on the day of admission (day 0), and 1 week after admission (day 7) using 0 to 10 numerical rating scale (NRS). Analgesic use was evaluated with 6 categories based on National Comprehensive Cancer Network and Korean pain management guidelines. Pain intensity and analgesic use appropriateness were compared at day −7, day 0, and day 7 for the patients who were admitted to the PCU.
Results:
Pain intensity decreased significantly on day 7 of PCU admission compared to it on day 0 (NRS: 4.05 vs 2.66, P < .001). A significant negative correlation was found between pain intensity and the proper use of analgesics (r = –0.407; P < .001, r = –0.309; P = .001, r = –0.241; P = .009, on day −7, day 0, day 7, respectively).
Conclusion:
The mPCT contributed to the reduction of inappropriate use of analgesics and improved pain control. Pharmacist intervention appeared to have improved pain control in patients under palliative care. Each team member’s role should be individualized and developed further.
Introduction
The majority of cancer patients suffer from pain at some point in their illness, and more severe pain is experienced at the advanced or terminal stage. 1,2 It is well known that pain is a main contributor to a patient’s quality of life, especially at the later stages of cancer. 3 One study reported that pain intensity decreased more in the palliative care setting compared with the general oncology ward setting due to the use of specific pain management programs. 4 Considering individual differences in pain perception, multifaceted assessment and treatment strategies are critical to achieve effective pain management and to ease the suffering of patients in pain. In this regard, several practice guidelines recommend a multidisciplinary team approach to palliative care. 5,6 Pharmacological interventions guided by palliative pharmacists have shown beneficial outcomes in terms of shortening duration of hospitalization, the interval between admission and the initial palliative care consultation, and the time from the initial consultation to discharge or death. 7 Additionally, as the most important method of pain management is pharmacotherapy, 8 several studies have investigated and suggested the role of pharmacists in solving problems related to pharmacotherapy. 9 -12 In Korea, most palliative care units are housed in major hospitals to effectively provide specialized professional services for patients who have pain that is refractory to more conventional interventions. However, effective pharmacotherapy is often limited by formulary restrictions, off-label uses, improper administration routes, and inadequate opioid dosages. Our multidisciplinary palliative care team (mPCT) runs a palliative care program in which the team pharmacist is primarily responsible for optimizing pharmacological interventions and support measures. Therefore, the purpose of this study was to evaluate the impact on pain management by mPCT and the team pharmacist.
Methods
Study Design
Study patients were at least 18 years of age and were hospitalized in the palliative care unit (PCU) for 7 days or more at the after being transferred from the wards, emergency center, or outpatient clinics due to worsening of oncologic pain. Demographic and clinical information collected for the study included age, gender, primary tumor sites, presence of renal and hepatic diseases, Eastern Cooperative Oncology Group (ECOG) performance status, 13,14 and chemotherapy component drugs for the period between April 2014 and December 2015. Study data were collected retrospectively using medical records.
Study Setting
The mPCT consisted of physicians, nurses, a pharmacist, and non-clinical support staff, including a team manager, a chaplain, art therapists, social workers, a volunteer manager, and a bereavement counselor. The team members participated in medical rounds twice a week for assessing pain severity and related symptoms. Additional rounds were held as needed to discuss the progress of disease, to coordinate treatment, and to plan discharge.
Pain Assessment
Patient-reported pain intensity was recorded for 24 hours 7 days before PCU admission (day −7), on the PCU admission day (day 0), and 7 days after the PCU admission (day 7). If no pain scores were available for any of these days, the closest record from the day was used. A numerical rating scale (NRS) was used to assess pain, ranging from 0 for no pain to 10 for the most severe pain.
The mPCT and the Team Pharmacist
The team pharmacist was responsible for recommending medications and evaluating the use of analgesics. The validation and intervention of analgesic prescriptions were performed based on the type and severity of pain, dose, routes, and schedule (around-the-clock or as-needed). Any contraindications, drug interactions, and adverse effects were also assessed. Furthermore, the mPCT pharmacist provided patient counseling for nonadherent patients and up-to-date education for staff training on evidence-based treatment with new analgesics.
Analgesic Use Evaluation
Analgesic use is assessed in 6 categories by The Korean Cancer Pain Management Guidelines and the National Comprehensive Cancer Network (NCCN) guidelines. 15,16 The 6 measures were (1) drug selection based on the type and severity of the pain; (2) dosage for chronic pain; (3) for breakthrough pain; (4) reassessing each patient’s pain to adjust the pain medication to meet the patient-specific goals for comfort, function, and safety; (5) analgesic use that reflects renal or hepatic function; and (6) monitoring adverse effects. Our criterion for the appropriateness of analgesic use was whether administration of each medication followed the 6 categories of recommendations or not. The appropriateness of analgesics was met when medication was used in compliance with all the 6 criteria. If any of the recommendations was not fulfilled, medication use was considered inappropriate, and assessments for each recommendation were conservative. The Institutional Review Board of the Yonsei University Health System approved the study protocol.
Statistical Analysis
Data were analyzed using descriptive statistics. The appropriateness of analgesics was calculated using a generalized estimation equation. Changes in pain intensity over time were analyzed using a mixed model. The correlation of pain intensity scores and appropriateness of analgesic use was analyzed using a point-biserial correlation with IBM SPSS Statistics for Windows, version 24.0 (IBM Corporation, Armonk, New York).
Results
Analgesic Use Before and After PCU Admission
Data were analyzed for 107 patients with 117 prescriptions (49 males, mean age 58 years; Table 1). For chronic pain, the most frequently prescribed medications before PCU admission were fentanyl transdermal patches (36.1%), followed by morphine intravenous infusions (IVIs), (29.9%) and oxycodone controlled-release (CR) tablets (23.7%; Table 2). However, the rate of morphine IVI use increased significantly after admission to the PCU (29.9% on day −7, then 49.1% and 44.5% on day 0 and day 7, respectively; P < .001), and morphine IVI became the most frequently used analgesic formulation, followed by fentanyl patches (37.8%) and oxycodone CR (14.3%; Table 2). For breakthrough pain, morphine intravenous push (IVP) and oxycodone immediate-release (IR) tablets were commonly used before PCU admission (on day −7), with the rate of morphine IVP administration increasing (33.6%, 58.4%, 50.8% on day −7, day 0, and day 7, respectively; P < .001) and the rate of oxycodone IR tablets administration decreasing (32.8%, 29.2%, 25.4% on day −7, day 0, and day 7, respectively; P = .633; Table 2). The rate of fentanyl transmucosal tablet administration increased significantly over time (12.1%, 8.0%, 19.2% on day −7, day 0, and day 7, respectively; P = .002), whereas administration of tramadol IVP (10.3%, 1.8%, and 1.5% on day −7, day 0, and day 7, respectively; P < .001) and meperidine intramuscular injection (IM; 3.5%, 0%, and 0% on day −7, day 0, and day 7, respectively; P = .036) significantly decreased after PCU admission (Table 2).
Patient Characteristics.a
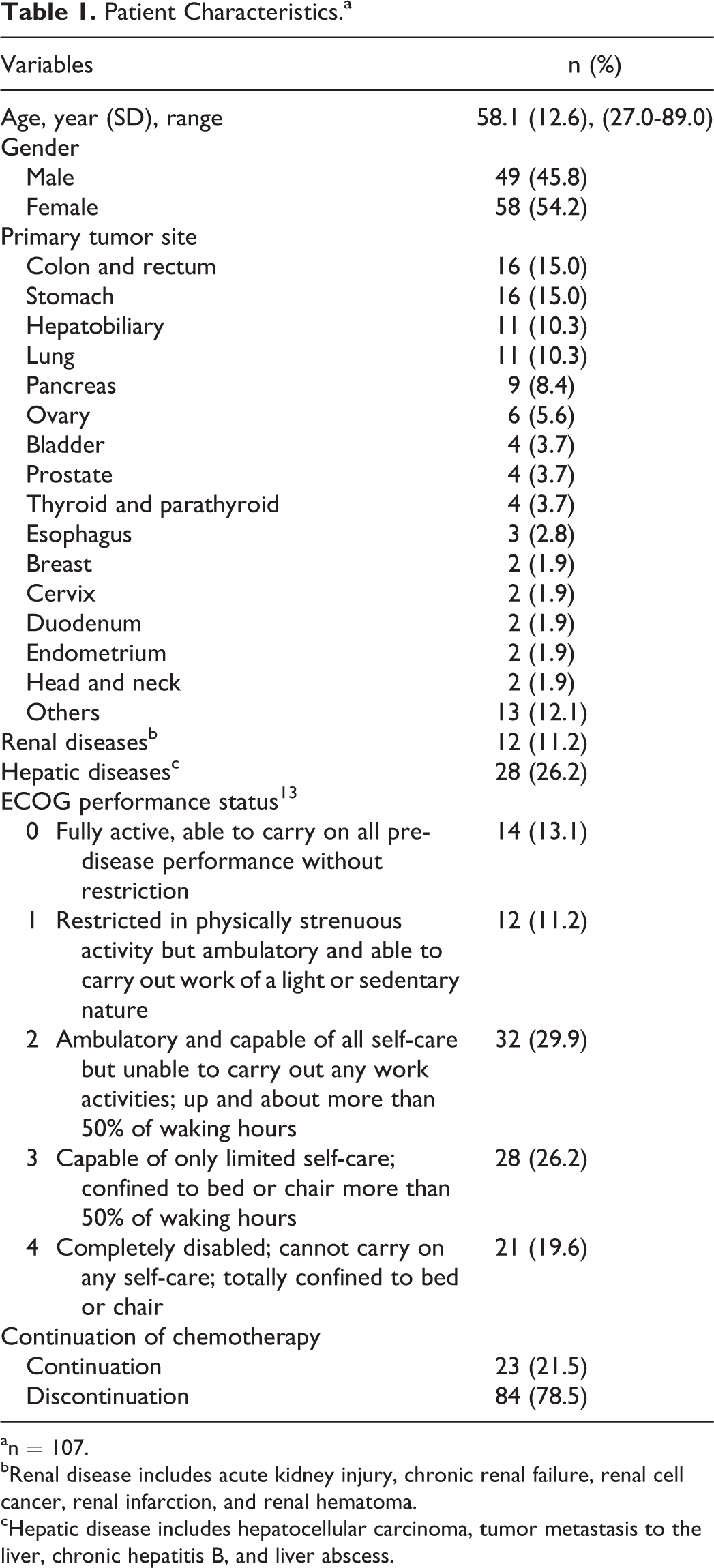
an = 107.
bRenal disease includes acute kidney injury, chronic renal failure, renal cell cancer, renal infarction, and renal hematoma.
cHepatic disease includes hepatocellular carcinoma, tumor metastasis to the liver, chronic hepatitis B, and liver abscess.
Usage of Analgesics.a
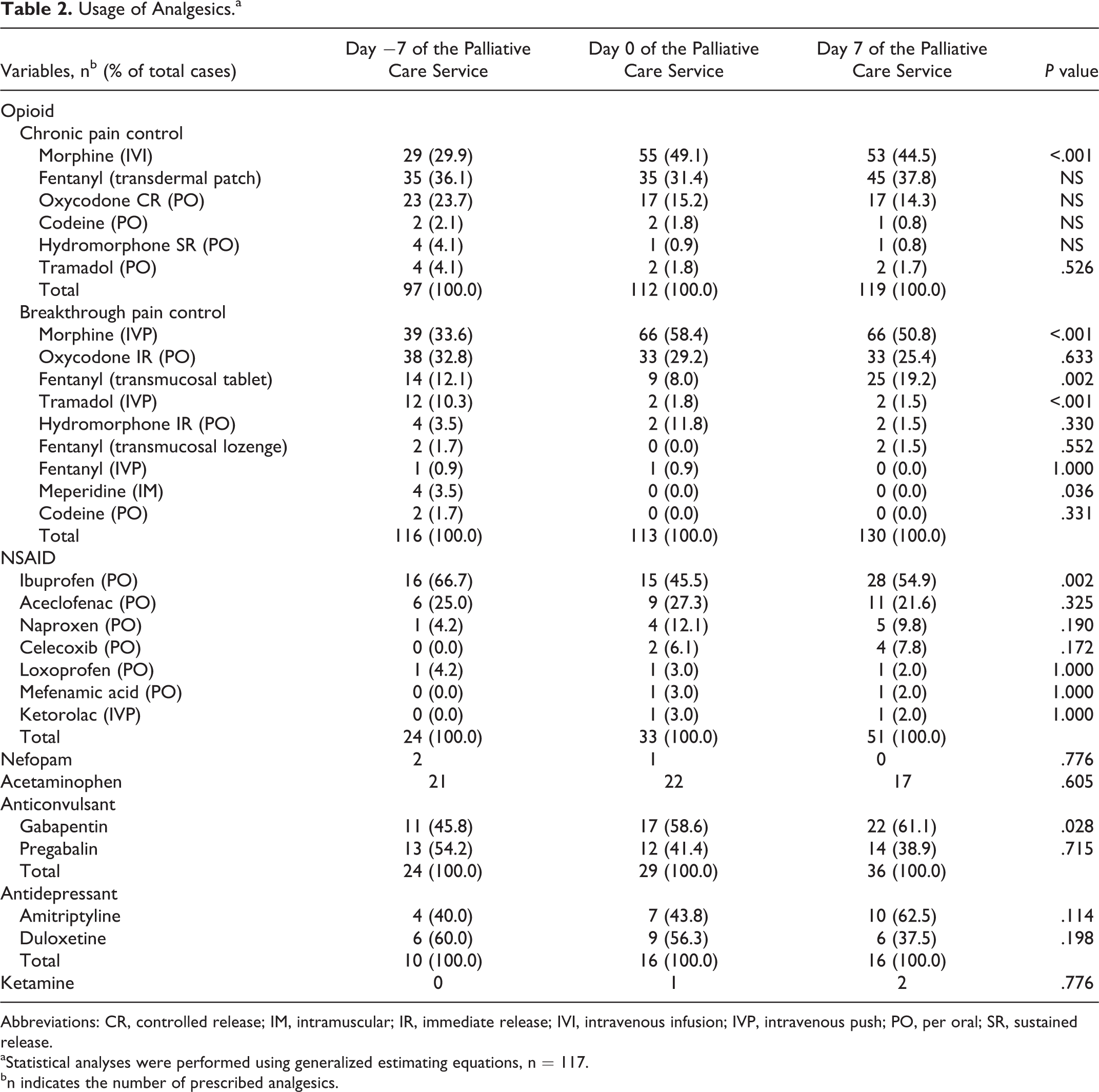
Abbreviations: CR, controlled release; IM, intramuscular; IR, immediate release; IVI, intravenous infusion; IVP, intravenous push; PO, per oral; SR, sustained release.
aStatistical analyses were performed using generalized estimating equations, n = 117.
bn indicates the number of prescribed analgesics.
Non-opioid analgesics prescribed for our study patients included acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), nefopam, gabapentin, pregabalin, amitriptyline, duloxetine, and ketamine (Table 2). In this study, nonopioid analgesics have been often used as an adjunct to opioid administration. Ibuprofen was the most frequently administered nonopioid, and its rate of administration was significantly different before and after PCU admission (66.7%, 45.5%, and 54.9% on day −7, day 0, and day 7, respectively; P = .002; Table 2). The rate of Gabapentin administration significantly increased after PCU admission (45.8%, 58.6%, and 61.1% on day −7, day 0, and day 7, respectively; P = .028), but other adjuvant analgesics did not show significant changes (Table 2).
Analgesic Use and Pain Control
The mean self-rated NRS pain score was 3.16 on day −7, 4.05 on day 0, and 2.66 on day 7, indicating that, for most patients, pain was most severe on the day of PCU admission (P < .001, Figure 1). Among the 117 prescriptions, the appropriateness of analgesic use based on guidelines 14,15 improved over time (35.0%, 34.2%, and 75.2% on day −7, day 0, and day 7, respectively; P < .001; Figure 1, Table 3). Interestingly, the appropriateness of opioid prescriptions significantly improved over time (35.9%, 35.9%, and 76.9%, on day −7, day 0, and day 7, respectively; P < .001), but the appropriateness of NSAID use remained consistent at about 90% (Table 3). Moreover, a significant negative correlation was found between pain intensity and appropriate use of analgesics (r = –0.407, P < .001 on day −7; r = –0.309, P = .001 on day 0; r = –0.241, P = .009 on day 7; Figure 1).

Percentage of appropriate analgesic use and mean pain intensity (n = 117). For the 117 cases, appropriate analgesic use is shown by a blue bar graph () and expressed in terms of percentage on the left axis. The percentage of appropriate analgesic use at each time point showed significant differences (P < .001). The mean pain intensity score is shown by black diamonds and solid lines ( ), expressed as NRS score on the right axis. The difference in pain intensity was also significant (P < .001). There was a significant negative correlation between appropriate analgesia and pain intensity (r = −0.407, P < .001 for day −7, r = −0.309, P = .001 for day 0, r = −0.241, P = .009 for day 7).
), expressed as NRS score on the right axis. The difference in pain intensity was also significant (P < .001). There was a significant negative correlation between appropriate analgesia and pain intensity (r = −0.407, P < .001 for day −7, r = −0.309, P = .001 for day 0, r = −0.241, P = .009 for day 7).
Appropriateness of Analgesics use.a
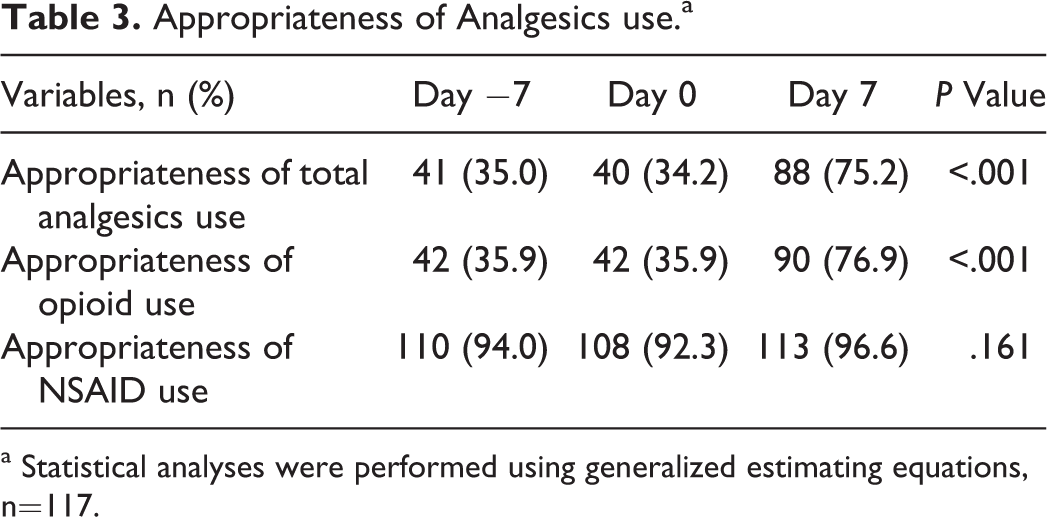
a Statistical analyses were performed using generalized estimating equations, n=117.
Appropriateness of Analgesic Use
The appropriateness of analgesic doses (for chronic pain: 87.2%, 80.3%, and 95.7% on day −7, day 0, and day 7, respectively; P = .003; for breakthrough pain: 88.9%, 88.9%, and 96.6% on day −7, day 0, and day 7, respectively; P = .049) and the rate of reassessment of each patient’s pain to adjust the medication for breakthrough pain (63.2%, 68.4%, 91.5% on day −7, day 0, day 7, P < .001) both significantly improved over time (Table 4). There was also a significant improvement in the monitoring of side effects and prophylactic use over time (65.0%, 65.8%, and 86.3% on day −7, day 0, and day 7, respectively; P < .001; Table 4).
Appropriate use of Analgesics Evaluated Using 6 Categories Based on the Korean Cancer Pain Management Guideline and the National Comprehensive Cancer Network Guideline.a
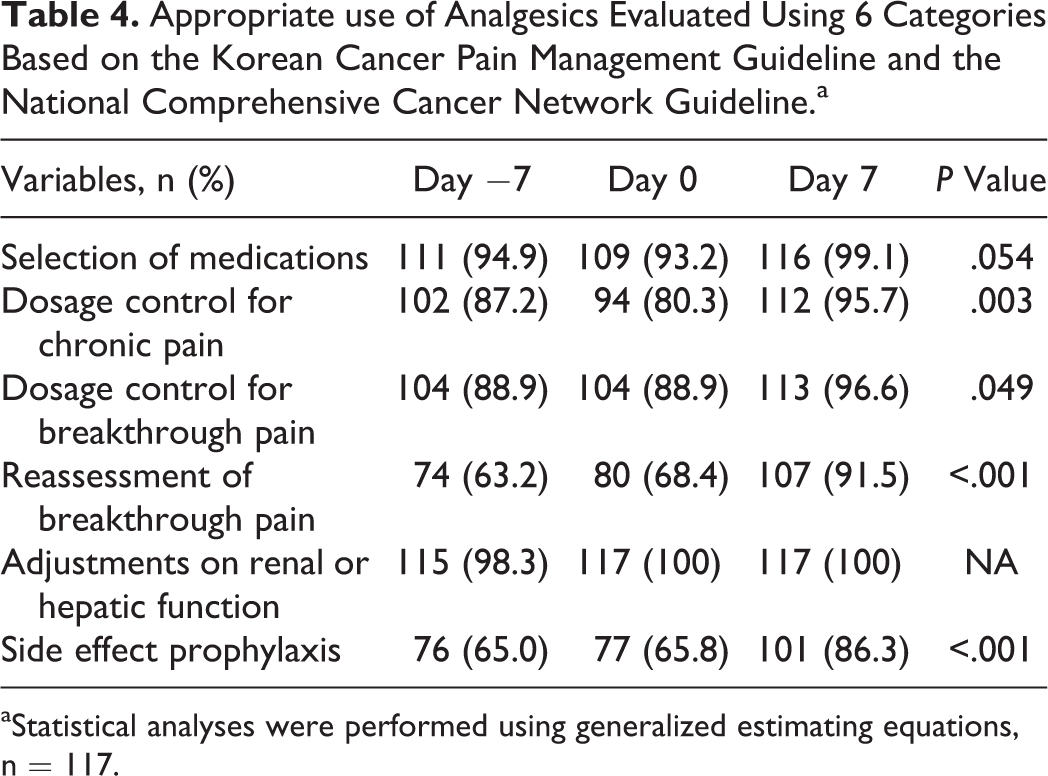
aStatistical analyses were performed using generalized estimating equations, n = 117.
The most common problem associated with opioid administration was inappropriate doses for both chronic and breakthrough pain (for chronic pain: 6.8%, 12.0%, and 2.6% on day −7, day 0, and day 7, respectively; P = .021; for breakthrough pain: 11.1%, 11.1%, and 3.4% on day −7, day 0, and day 7, respectively; P = .049; Table 5). The rate of inappropriate reassessment of pain after opioid administration for breakthrough pain was also alarmingly high but improved over time (27.4%, 27.4% and 8.5% on day −7, day 0, day 7, respectively; P < .001; Table 5). Other problems included failure to prescribe analgesics for breakthrough pain (10.3%, 5.1%, and 0% on day −7, day 0, and day 7, respectively; P = .001) and failure to prescribe prophylaxis for constipation (34.2%, 31.6%, and 12.0% on day −7, day 0, and day 7, respectively; P < .001; Table 5). Inappropriate NSAID use was observed in the contexts of stomach upset, renal dosing adjustments, duplication, and mild pain. However, there were no significant changes in NSAID from −7, to day 0, to day 7 (P = .161; Table 3).
Inappropriate Use of Opioids.a
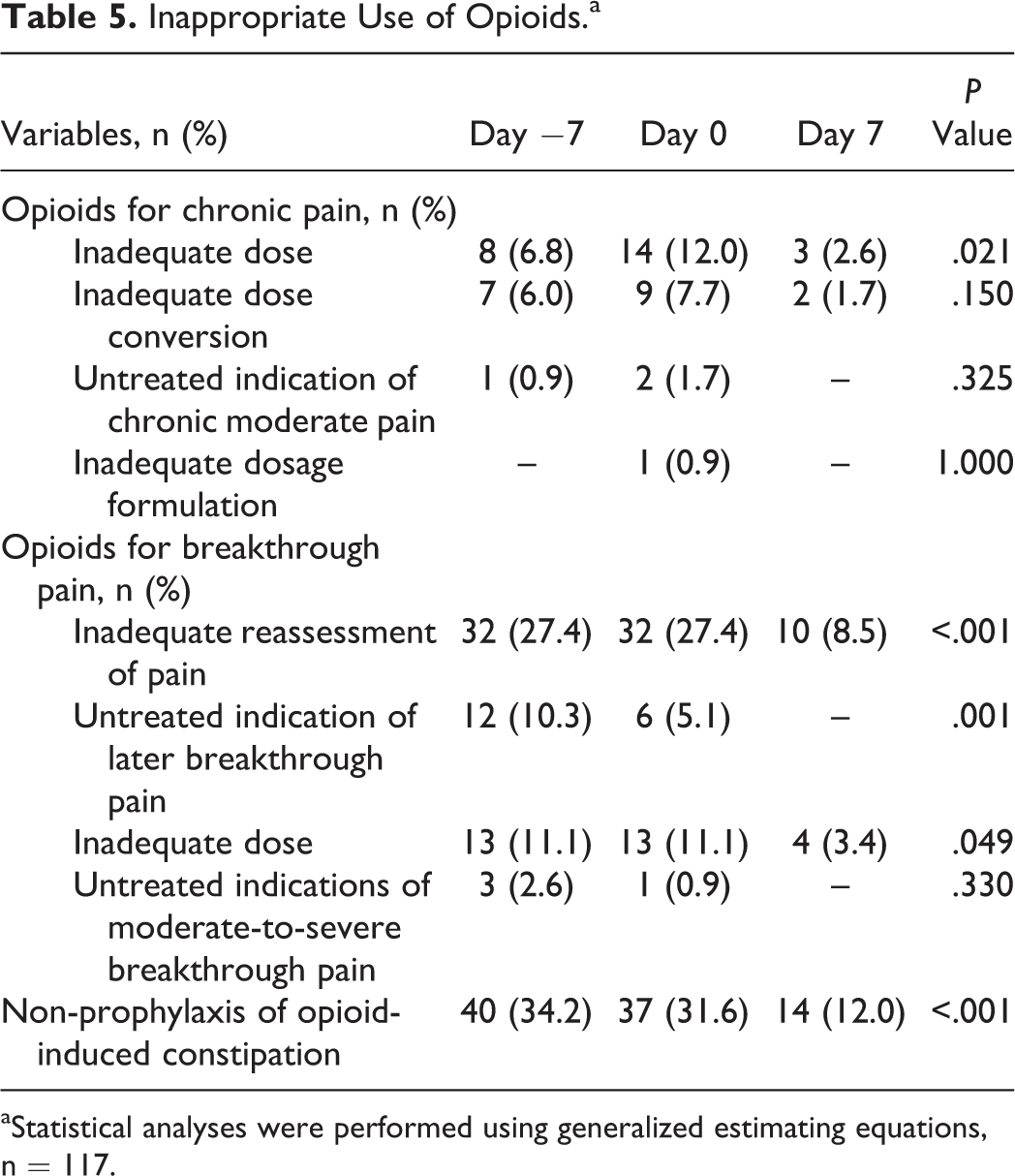
aStatistical analyses were performed using generalized estimating equations, n = 117.
Discussion
Our mPCT has a leading role in alleviating pain and relieving symptoms for PCU patients. We confirmed that the appropriateness of analgesic use increased significantly and that the mean pain intensity decreased significantly by day 7. The decline of pain intensity may be attributable to the multidisciplinary interventions implemented by the palliative care team, an explanation previously supported by Peng et al and Ise et al 17,18 Moreover, because pharmacological treatment is a major contributor to cancer pain management, emphasis should be placed on the inclusion of a team pharmacist in the mPCT. Considering patients’ clinical characteristics and the attributes of each analgesic agent, the pharmacist’s involvement in medication prescription decisions could improve pain control and prevent inappropriate analgesic use.
We assessed the appropriateness of analgesic prescriptions using the NCCN guidelines and the Korean Cancer Pain Management Guidelines. The Pain Management Index (PMI) was used previously as a tool to assess the appropriateness of cancer pain management. 19,20 However, the PMI is based solely on the World Health Organization analgesic ladder, which is a stepwise approach to the use of analgesics, sequentially from none to non-opioids, to weak opioids, and to strong opioids. 21,22 Thus, the analgesic ladder and PMI are too simplistic to assess the efficacy of analgesics for pain control among cancer patients who have already been exposed to high-intensity analgesics. Russell et al. assessed several methods of evaluating cancer pain management, including the PMI. Although there was a significant change in the control of pain on a population level, the PMI was not sensitive enough to detect the change. They concluded that there was a limitation to the application of PMI measurements for assessing cancer pain management, and a dynamic method of assessing changes in prescriptions and pain levels over time should be developed. 23 The official pain management guidelines include recommendations for selecting analgesics, doses for chronic pain and breakthrough pain, reassessment of breakthrough pain, renal or hepatic dosing adjustments, and side effect prophylaxis. Accordingly, this study analyzed the appropriateness of analgesic use based on the recommendations provided by these standard guidelines rather than being guided by the PMI.
The Joint Commission published recommendations for practitioner training and respecting patient rights to pain management in addition to recommendations for assessing and managing pain. 24 Including pharmacists in mPCTs improves the likelihood of fulfilling such recommendations. As ours has done, mPCT pharmacists should offer consistent and diverse services related to the use of analgesics for both therapeutic (for the patients) and educational purposes (for the patients and other mPCT members), which improve both current and future pain management efforts. Pharmacist should also monitor medication use and actively prevent adverse reactions. Overall, the team pharmacist serves as a medication specialist assessing individual pain intensity to adjust opioids and nonopioids prescriptions to minimize the frequency of inadequate prescriptions. For example, meperidine use significantly decreased over time in our study, which contributed to clinical improvements, given that long-term use of meperidine is associated with adverse effects on the central nervous system caused by drug metabolites. 25
The main activities of the mPCT pharmacists were included in the study but were not limited to the following: (1) to review prescriptions and their appropriateness according to NCCN guidelines and the Korean Cancer Pain Management Guidelines, (2) to assess pain intensity using the NRS, (3) to adjust analgesics based on daily pain intensity and the severity of the related symptoms, (4) to counsel patients with specific requests or compliance problems, (5) to provide drug information, (6) to work closely with other healthcare professionals to facilitate medication-related issues, (7) to recommend medication substitutions, (8) to document interventions, and (9) to deliver training for the team members.
We investigated and analyzed based on the chart review and found that the common reasons for the inappropriate use of opioids were failure to prescribe prophylaxis for constipation, failure to reassess analgesic efficacy, and failure to adjust prescriptions in a timely manner after the administration of a short-acting opioid for breakthrough pain. It is primarily provider’s responsibility of routine pain assessment and prescribing bowel regimens with narcotics. However, this routine practice can be efficiently applied with the support of nurses and pharmacists as the mPCT efforts. It is well known that timely reassessment of pain after the administration of analgesics increases the safety and effectiveness of pain management. 26 Other reasons for the inappropriate use of opioids included failure to prescribe pain control and inappropriate doses of rapid-acting analgesics for breakthrough or chronic pain. Furthermore, some opioid doses were inadequate for relieving pain before the PCU admission. Overcoming inappropriate analgesic use and improving pain control require in-depth, professional knowledge about medications, including pharmacokinetic and pharmacodynamic properties. Again, this places emphasis on the need for pharmacists as part of mPCTs.
In addition, comparing the appropriateness of each type of analgesics before and after admission to PCU, the results showed that the opioid prescriptions were relatively inappropriate prior to the mPCT involvement and improved significantly after the mPCT involvement, but the NSAID prescriptions continued to be appropriate without significant changes before or after the mPCT involvement. As opioid and NSAID have different pharmacological properties, NSAIDs are administered relatively simple to within the recommended dose due to the ceiling effect and side effects, but opioids have no ceiling effect and require detailed observation of effects and adverse reactions depending on individual patients to be used in an optimal dose. Therefore, it is possible to assume that the interprofessional collaboration between the mPCT and the team pharmacist played a significant role in improving the adequacy of the opioid prescriptions, particularly. It will be necessary to check later whether the degree of interventions of the mPCT or team pharmacist is different depending on the type of analgesics, and whether the differences are related to the overall appropriateness of using analgesics or pain control.
This study had several limitations. First, it was a retrospective study using medical records. Second, the study was conducted with a relatively small sample size. Third, adverse reaction data relied on patient self-reporting. A long-term prospective analysis that demonstrates outcomes and considers each team member’s function and role is warranted in the near future. Nevertheless, the present study confirmed the role of mPCTs and the team pharmacist in improving the pain management of cancer patients by reviewing pain intensity and enhancing the appropriateness of analgesic use.
Conclusion
The mPCT improved the appropriate use of analgesics, which was associated with an overall reduction of pain intensity. The study demonstrated the successful running of a pharmaceutical care service for cancer patients in a PCU in light of the recent global interest in multidisciplinary team pharmacist-mediated healthcare interventions in patient care settings. Therefore, this study confirmed that the appropriateness of analgesics needs to be considered in pain management and that a dedicate pharmacist is needed among mPCT members.
Further analysis of intervention cases of the palliative care team pharmacist and multicenter study of the palliative care team pharmacist’s operation status are expected to develop the role of palliative care team pharmacist and provide more safe and effective pharmaceutical care services in palliative care.
Footnotes
Acknowledgments
We wish to acknowledge the collaborative efforts of the staff members of the Department of Pharmacy, Severance Hospital, Yonsei University Health System and the Palliative Care Center, Yonsei Cancer Center.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.