
Abstract
Experts estimate that over 25 million Americans are in recovery from addiction to alcohol and other drugs. Many will be confronted with a serious progressive illness necessitating palliative care or hospice services. In current literature, substance use disorder has mostly been examined in relation to appropriate symptom assessment and management, opioid risk screening, and controlled substance prescribing practices. However, as hospice and palliative care (HPC) clinicians strive to provide whole person care for the seriously ill, awareness and facilitation of healthy psychosocial–spiritual coping strategies for recovering addicts should enhance such care. One of the more common support mechanisms to support recovery is the 12-step program, based on Alcoholics Anonymous. Twelve-step programs have been shown to provide effective coping strategies, not only to help facilitate ongoing abstinence but also to support other psychosocial–spiritual crises. The HPC providers may help to serve those living with addiction disorders better by assessing not only patient histories of substance use/abuse and other addictive behaviors but by facilitating their ongoing support recovery efforts. Here, we use 2 HPC cases to illustrate the value of 12-step recovery programs in patient support and provide recommendations for enhancing such healthy coping in HPC clinical settings.
Introduction
Media coverage of the current opioid epidemic reminds us that substance use disorder (SUD) remains uncomfortably prevalent in the United States. 1,2 This year, over 20 million Americans will have addiction to alcohol and other drugs, defined by the American Society of Addiction Medicine (ASAM) as “a primary, chronic disease of brain reward, motivation, memory and related circuitry…reflected in an individual pathologically pursuing reward and/or relief by substance use and other behaviors.” 3,4 Of these, some will enter remission or recovery programs; experts conservatively estimate that number to be over 25 million Americans. 5 For most, ongoing abstinence from SUD is a lifelong challenge, often punctuated with intermittent or permanent relapse. 5
Many of these individuals will also have a serious, progressive illness warranting hospice and palliative care (HPC) interventions; in fact, up to 25% of patients receiving hospice care currently have one or more SUDs, either active or in remission. 6,7 To date, most related HPC literature has focused on appropriate symptom assessment and management, opioid risk screening, and controlled substance prescribing practices. 8 –11 For example, patients with a SUD history may report more symptom burden. 9,12
What remains missing, however, is attention to the role of addiction recovery in cultivating healthy psychosocial and/or spiritual coping in the face of adversity, such as a life-threatening illness. The ASAM definition of addiction clarifies that the disease of addiction “leads to characteristic biological, psychological, social, and spiritual manifestations” (emphasis added). 3 Therefore, recovery from an addictive disorder may also involve a person developing a new or renewed sense of spirituality (defined broadly by the International Consensus Conference as “a dynamic and intrinsic aspect of humanity through which persons seek ultimate meaning, purpose, and transcendence, and experience relationship to self, family, others, community, society, nature, and the significant or sacred”). 13,14 Although assessment of SUD has been identified as an important but overlooked element of patient medical history, including across HPC settings, such information almost always neglects to ascertain treatment history whether pharmacologic (eg, naltrexone, disulfiram) or nonpharmacologic (eg, cognitive-behavioral therapy, motivational enhancement therapy, 12-step program). 15 As HPC clinicians strive to provide whole-person care for the seriously ill, awareness and facilitation of healthy spiritual coping strategies for recovering addicts should enhance such care; as recovery lay literature indicates, failure to do so can delay appropriate supportive care to those with advanced illness. 16
Twelve-Step Recovery as a Model of Spiritual Coping
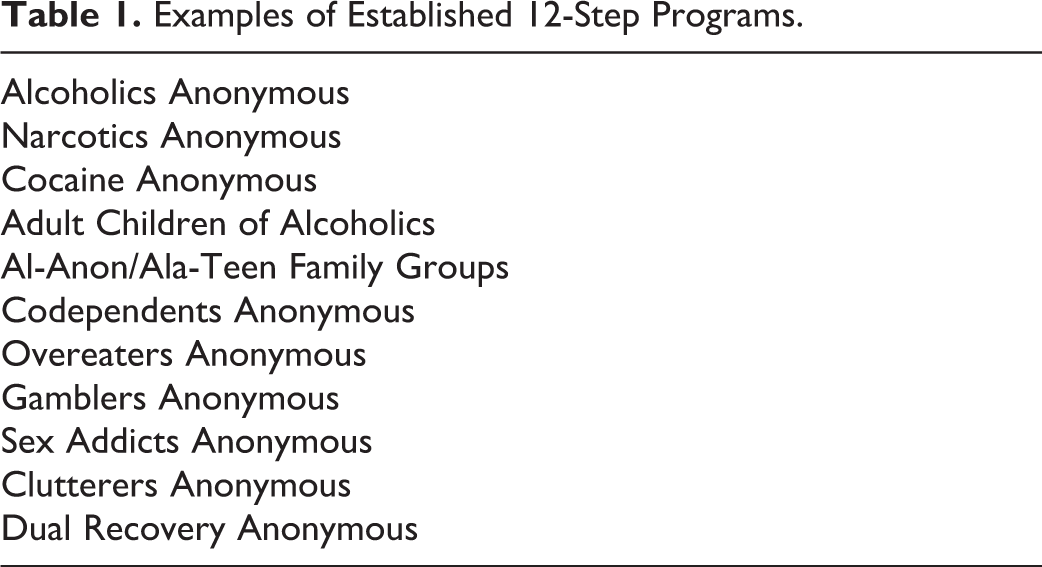
Through the relatively short history of addiction medicine, one of the most successful methods of supporting abstinence is participation in 12-step recovery programs. The first and best-known of these, Alcoholics Anonymous (AA), has grown to an estimated membership of over 2 million worldwide and served as a model for 12-step programs targeting other addictive behaviors (eg, Narcotics Anonymous, Overeaters Anonymous, etc) as well as supporting those affected by addiction (eg, Al-Anon Family Groups, Ala-Teen; Table 1). 17 Many more have been exposed to AA literature and meetings, which many treatment programs urge patients to explore as a way of supporting their recovery.
Examples of Established 12-Step Programs.
Unlike most other pathways to recovery from addiction, a foundational element of 12-step programs is a core belief that active addiction represents a disease of the body, mind, and spirit that can be healed through recovery program-guided spiritual growth. 17,18 As such, for members of AA and other 12-step programs, spiritual practice and support from one’s spiritual community can be a very important part of coping with adversity. For the alcoholic in recovery, adversity can be anything that leads to relapse, including relationship strain, job loss, and of course, life-threatening illness or impending death. Thus, the 12-step framework can promote healthy coping in advanced illness.
Here, we outline psychosocial–spiritual support structures of 12-step recovery programs, concentrating on AA as the original therapeutic model. Acknowledging that 12-step programs are but one effective means to achieve recovery in addiction, we choose this construct as our focus because of its worldwide prevalence and its cornerstone of spiritual growth. Using actual patient cases to ground our discussion, we introduce concepts and language to help HPC clinicians assess and facilitate supportive needs for patients who are engaged in 12-step programs.
Case 1
HL is a 63-year-old Caucasian man who is recently diagnosed with recurrent acute myelogenous leukemia (AML). He lives in a rural community with his wife and dog; his 2 adult children live in the same county. HL is a recovering alcoholic. He has been sober for 14 years. Although initially treated for alcohol addiction in an inpatient program, he became familiar with AA soon after and attributes his sobriety to the 12-step program. He now meets with his AA sponsor weekly and attends meetings at least 3 times a week. He also sponsors 2 recovering alcoholics.
HL now requires an allogeneic bone marrow transplant (BMT) for his AML. For this, he must temporarily move to a university hospital in another part of the state. During his initial visits with the BMT team, a social worker asks about psychosocial–spiritual support systems. HL discloses his sobriety and asks for a list of local AA meetings that he can attend; he discovers there is one meeting each week very close to the hospital. Anticipating the stress of the treatment, HL telephones his AA sponsor daily. When admitted to the hospital, HL brings his copy of the Big Book (the major AA-sponsored text) for frequent reading.
Case 2
MT is a 58-year-old woman with end-stage congestive heart failure. She is also a recovering heroin addict, now abstinent for nearly 4 years. During most of that time, her recovery program has consisted of active involvement in Narcotics Anonymous through regular meeting attendance, sponsorship of several newly recovering addicts, and service work with her local NA chapter by acting as its treasurer. She typically has met with her sponsor twice weekly and in times of stress would speak by phone daily.
MT has been hospitalized 3 times in 6 weeks for her heart failure. She is now unable to care for herself at home and her functional status continues to deteriorate. She has no family engaged in her life. Dyspnea, anxiety, and chronic pain remain her most challenging symptoms. During her most recent hospitalization, she agreed to a hospice care referral. Given her unmanaged symptoms, she is transferred to a local general inpatient hospice facility. She worries about opioid therapies for her symptoms as a potential trigger for relapse. At the inpatient hospice facility, her sponsor is able to visit regularly and brings her Narcotics Anonymous literature to continue to study. Other NA members from her local chapter (her “home group”) take turns visiting as well. They connect her to frequent NA meetings by phone. As MT declines, fellow NA members take turns sitting at her bedside holding vigil, praying with her, and reading to her. After one week, she dies at the inpatient hospice facility.
What Are 12-Step Programs and How Do They Work?
Alcoholics Anonymous can trace its roots to the Oxford Group movement, a Christian evangelical group that supported self-awareness, acknowledgement and examination of character defects, making amends for harm done, and sharing personal experience. 19 After multiple failed attempts, New York stockbroker William Wilson (known in AA history as “Bill W.”) finally achieved sobriety after a spiritual experience with the Oxford Group. Advised that sobriety could be best maintained through delivering service and support to others in recovery, Wilson began meeting regularly with physician and recovering alcoholic Dr Robert Smith (“Dr. Bob”). In 1935, they formed AA. 20 Within several years, their membership had grown to over 100 recovering alcoholics; today AA has an estimated 114 000 member groups worldwide. 17 In order to maintain focus on its primary mission to support those in recovery, AA remains independent and self-supporting, without ties to religious or professional organizations. 18
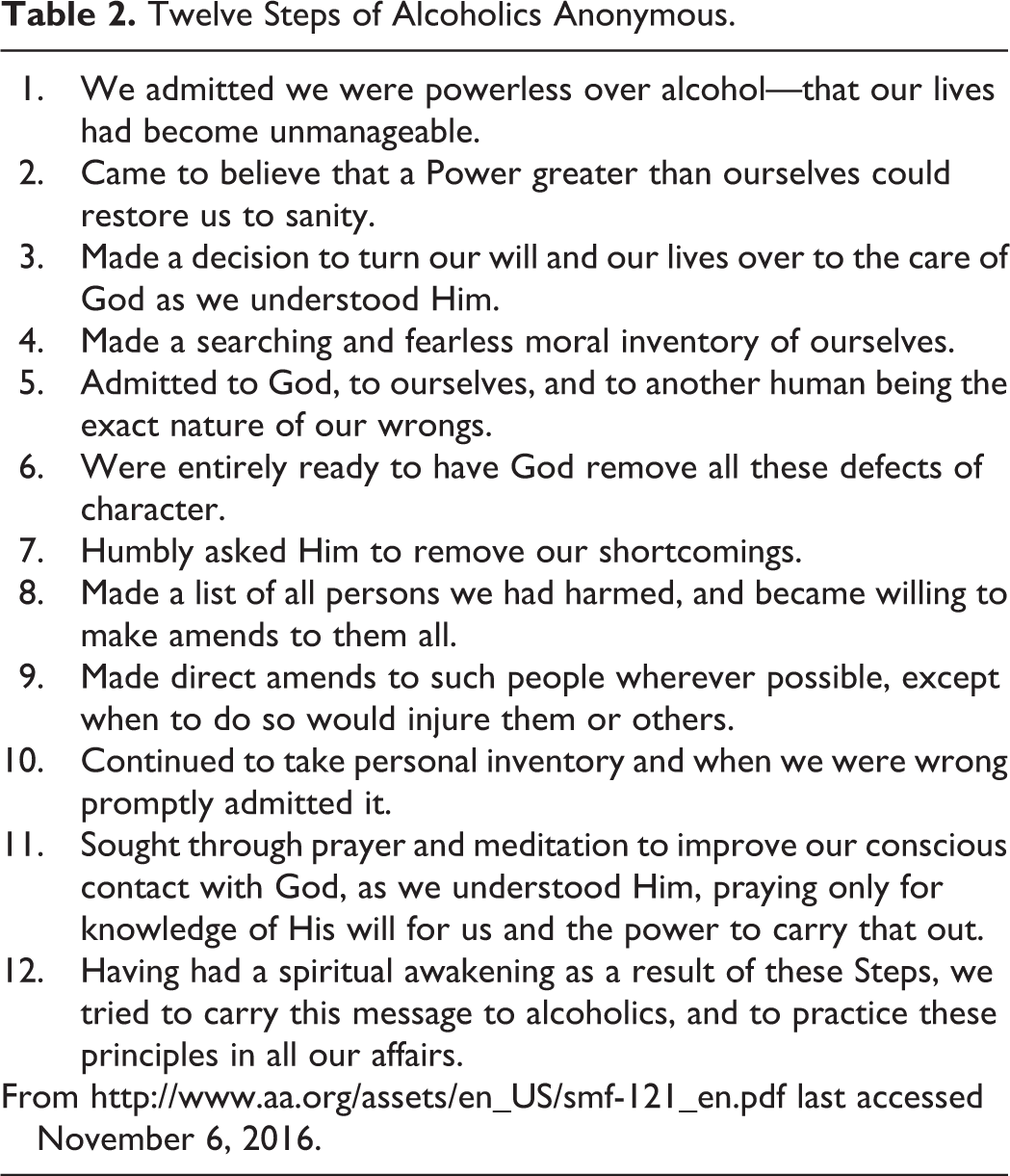
Today, the only requirement to participate is a desire to stop drinking. Meetings can consist of as few as 2 to 3 individuals or as many as dozens or even hundreds of participants. Most meetings are face-to-face, but also can be telephone-based or online. All meetings are free; participants are asked to make a small donation but this is not required. First published in 1938, “Alcoholics Anonymous” (also known as the “Big Book”) serves as the organization’s primary text. Through group meetings, as well as in individual sponsor–sponsee relationships, recovering alcoholics aim to achieve spiritual growth that will support ongoing sobriety by studying the Big Book and by moving through the 12 steps, also known as “working the steps” (Table 2). Alcoholics Anonymous and other 12-step programs also employ a series of “slogans” that can serve as simple reminders of coping strategies (Table 3).
Twelve Steps of Alcoholics Anonymous.
Example Slogans in 12-Step Programs.
Spiritual Growth for Coping With Addiction and Adversity
“Working the steps” aims to promote such spiritual development by awakening positive spiritual states not expressed while actively drinking, and/or fostering a new spiritual identity that is based on self-awareness, humility, making amends for wrongdoings, and sharing experiences of individual growth. Six of the 12 steps directly mention God (or a “higher power”) that remains personal or individualized (“as we understood Him”); they follow a path of spiritual development—acceptance of higher power (step 2), surrender to it (step 3), admission of wrongdoings (step 5), preparation for a higher power’s intervention (step 6), request for that intervention (step 7), and spiritual action to develop a close relationship with one’s higher power (step 11). Studies of 12-step members show some relationships between activity in the recovery program and spiritual and/or religious characteristics. For example, more frequent meeting attendance correlates with higher daily attachment to one’s God/higher power, forgiveness of others, purpose in life, and mystical experiences (step 12). Indeed, for many in recovery, the capacity to cease substance use may seem simply miraculous—note the “spiritual awakening” described in step 12.
Mechanism of behavior change research demonstrates that spiritual change is a vital component of initiating and maintaining recovery for an important minority of recovering addicts; the majority appear to receive the most strength and support from psychosocial connections through a the 12-step community. 21 Note that step 12 also marks the foundation of fellowship principles, where ongoing sobriety is maintained in large part by supporting others in recovery. In fact, studies suggest that engaging in 12-step activities in group settings—not only attending meetings, but service work to the organization, 12-step literature study, and engaging sponsor/sponsee relationships—may promote abstinence even more. 13 Returning to the origins of AA, such active service remains a hallmark of 12-step programs and helps to build the strong spiritual community experienced by both patient cases.
Twelve-Step Awareness in HPC Settings
As part of both medical and psychosocial–spiritual holistic care, HPC providers have a duty to intentionally assess and support ongoing recovery efforts by patients throughout the dynamic course of the advanced illness and by their family members as well. Several simple steps can facilitate this:
Elicit an Addiction Recovery History
Current clinical literature reminds that, in addition to a complete psychosocial–spiritual history, all patients receiving controlled substance pharmacotherapies should be assessed for risk and history of SUD, including alcohol.
21
For individuals who screen positive for SUD history, or for individuals who disclose other forms of addictive behaviors, eliciting a recovery history can provide important information for appropriate support and build therapeutic connections. The same applies to family members of individuals suffering from an addiction. Certainly, effective communication depends on the individual’s willingness to disclose such information, but simple nonjudgmental probing questions can be very effective. For example:
You mention that you have a history of using cocaine but stopped 6 years ago. What prompted you to stop using? What has helped you to keep from using cocaine again?
Your recovery from addiction is important to me and to your care. I know that recovery isn’t easy for anyone. Have you ever participated in a formal recovery program at a treatment center or through a 12-step program like Alcoholics Anonymous?
It’s helpful to learn that you are active in your 12-step program. Can you tell me more about your own specific program? Do you have a sponsor? Do you have a network? Do you attend meetings regularly and if so when? How can our team help support this part of your care?
I understand that your loved one has struggled with drug addiction for some time and that can be hard on family too. Do you have a way that you get support for yourself?
Become Familiar With Local 12-Step Programs
A variety of resources are easily accessible to share with patients and family members (eg, www.aa.org). The HPC teams might also choose to informally connect with one or more local 12-step program chapters in advance of patients needing immediate support, not dissimilar from connecting with a local church congregation or ministry. For patients less mobile or independent, these local chapters may be able to pay visits and/or bring resources to the bedside.
Have 12-Step Recovery Materials on Hand
Particularly relevant to facility-based care settings, making recovery program materials available to 12-step program members is a straightforward way to facilitate such coping. One or more copies of AA, 12-step meeting CD recordings, and information on frequent online or telephone-based meetings can be kept handy on site.
Conclusion
As HPC providers aim to relieve suffering for those with alcohol and other drug addiction disorders and their families/caregivers, attention to the spiritual and social-based recovery process of 12-step programs can help support healthy coping practices, particularly in times of distress. Similar to the importance of clinician attunement to spiritual or cultural needs of those living with a serious progressive illness or at the end of life, HPC providers may help to serve those living with addiction disorders better by assessing not only patient histories of substance use/abuse and other addictive behaviors but by facilitating their ongoing support recovery efforts.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.