
Abstract
Research Question:
How does the process of engagement and integration of sources of information outside patient–physician interaction affect how individuals with cancer interpret their treatment experience and prognosis?
Background:
Studies of patient–physician communication of prognosis in oncology highlight areas where misunderstanding occurs: understanding consequences of treatment, likelihood of treatment success, probability of cure, status/progression of illness, and prognosis. Theories proposing mechanisms that underlie this discrepancy cannot account for all instances of misunderstanding, including when complete and direct physician disclosure occurs. Prior research focused on patient–physician communication event(s) and immediate antecedents and consequences. However, less is known about what happens to information once it has been communicated and how a patient’s process to interpret the meaning of their experience affects their understanding of it. Our study explores this question by examining patient communication with sources of information other than treating physicians.
Methodology:
We conducted 10 semi-structured qualitative interviews with individuals diagnosed with 4 types of cancer at different stages. The interviews were analyzed using inductive qualitative analysis.
Results:
Participants in our sample consulted a variety of additional sources to give context and understanding to their communicated prognosis. These were important contributors to how they understood their prognosis and incorporated that understanding. They included family, friends/acquaintances, cancer survivors, support/survivor groups, secondary health-care staff, and relevant informational materials. Different motivations for seeking out these sources were also expressed. Participants expressed a link between their understanding of their prognosis and the variety of outside sources they enlisted for input and support.
Keywords
Background
Previous studies on patient–physician communication in cancer have highlighted that patients and caregivers primarily prefer to receive more (and specific) information about their disease rather than be shielded from it. 1 –6 These findings have articulated several specific areas where misunderstanding, misrepresentation, or limitation of information occurs, 7 such as understanding the disease and consequences of treatment, 8,9 the likelihood of treatment success, 10 patient preferences for care, 11 the probability of cure, 12 the status/progression of illness, 12 and prognosis. 13,14 Significantly, misunderstanding can occur even when doctors provide adequate information. 11,13,15,16
The focus of our article is prognosis communication, augmenting previous studies that have sought out communication approaches that enhance health outcomes, and avoid miscommunication. 2,9,14,17 –19 Utilizing the view of prognosis advocated for by Clayton et al 20,21 , our study explores both (1) likely outcomes of treatment (including time frame for disease progression and survival), and (2) what patients can expect (how treatment will occur, immediate and long-term side effects, and potential future symptoms or effects on functional ability).
Research in prognosis communication is highly nuanced and explores diverse facets, including patient preferences for receiving prognostic information 2,22 –24 ; types of prognostic information physicians communicate to patients 25 ; patient understanding of treatment aims and likely outcomes 26 ; and effects of communication on patient well-being, satisfaction, participation, and the physician–patient relationship. 18,22,27 There are several theories seeking to explain mechanisms underlying the patient–physician understanding discrepancy, including incomplete or unclear disclosure by physicians, 28 the use of euphemisms to communicate “bad” prognosis, 23 and compromised patient understanding due to stress of receiving bad news. 29 However, these theories cannot account for all instances of misunderstanding, including when complete physician disclosure has been observed. 11,13,15,16
Significantly, prognosis communication research has emphasized the patient–physician communication event(s) itself and its immediate antecedents and consequences. 30,31 Yet, little has been done examining what happens to this information once communicated. In addition, limited research evaluates the processes patients undergo to interpret the meaning of their prognosis, especially how that meaning may change when interacting with sources of information other than the communicating physician (eg, nurses 32 ). Understanding may change for the patient after prognostic information is initially communicated. 33,34 Cancer diagnosis is often accompanied by intense feelings of uncertainty, which can hinder effective communication. Patients often seek to mitigate this by turning to individuals other than their treating physician to increase certainty, maintain control, find additional interpretation or information, and facilitate decision-making. 3,17,34 Evidence suggests that this almost exclusive focus on patient–physician communication may be insufficient to fully clarify discrepancies in understanding. 20
Our study seeks to address this research gap by examining prognosis understanding from the patient’s perspective, focusing on sources of information sought out and utilized after the initial communication with a physician. In doing so, we explore how these additional sources can contribute to changes in understanding for a patient as they engage with additional information and integrate it into their understanding of their experience. We seek to map the various sources of information patients engage to understand their cancer experience (and their prognosis in particular) as well as the roles these informational sources play and the importance attributed to them in the process of communicating about and understanding prognosis.
Methods
All participants (n = 10; Table 1) were recruited from a regional cancer center in central Illinois. To be included in the study, participants must have had a definitive diagnosis of cancer (confirmed by referring oncologist) and have completed treatment. No exclusions were made based on type/stage of cancer or length of time since completion of treatment. Participants were recruited by their oncologist during follow-up visits at the medical center and referred to the research team. Upon signing consent forms and confidentially agreements, a research assistant conducted 1 to 2 in-person semi-structured interviews with each participant (Supplemental Appendix 1).
Demographic Characteristics.a
a Table 1 shows the demographic information of the participants
We used inductive analysis to produce a codebook following Braun and Clarke’s approach. 35 First, interviews were recorded, transcribed, and read. Then, initial codes were established. These codes were grouped into common themes, whereupon 2 researchers independently analyzed transcripts and audio-recordings. Themes centered on patient communication regarding their prognosis occurring with their physician and other individuals and informational sources. The researchers then discussed each interview to further refine the codebook and ensure consistency.
Finally, we engaged in member checking by providing participants with a draft of the final article and a personal participant ID number corresponding to those used in the article. This allowed them to see their quotes in context and give feedback about our interpretations. Five of 10 participants responded; 3 gave feedback that resulted in changes.
Results
Our analysis focuses on the different sources of information outside their treating physician(s) that participants enlisted to help them understand their prognosis. We grouped these into 6 different sources of information: health-care staff, family/friends, other survivors, survivorship groups, media sources, and other individuals. During the coding process, we assigned each category a level of importance for each participant based on the role participants felt that it played for them and the significance attributed to it in the interview (Figure 1). We coded each category as: specifically expressed as important by the participant, mentioned as important with no specific details, or not important. This was based on the frequency of reference to a particular source and whether or not participants emphasized it as important in their process of understanding their prognosis.
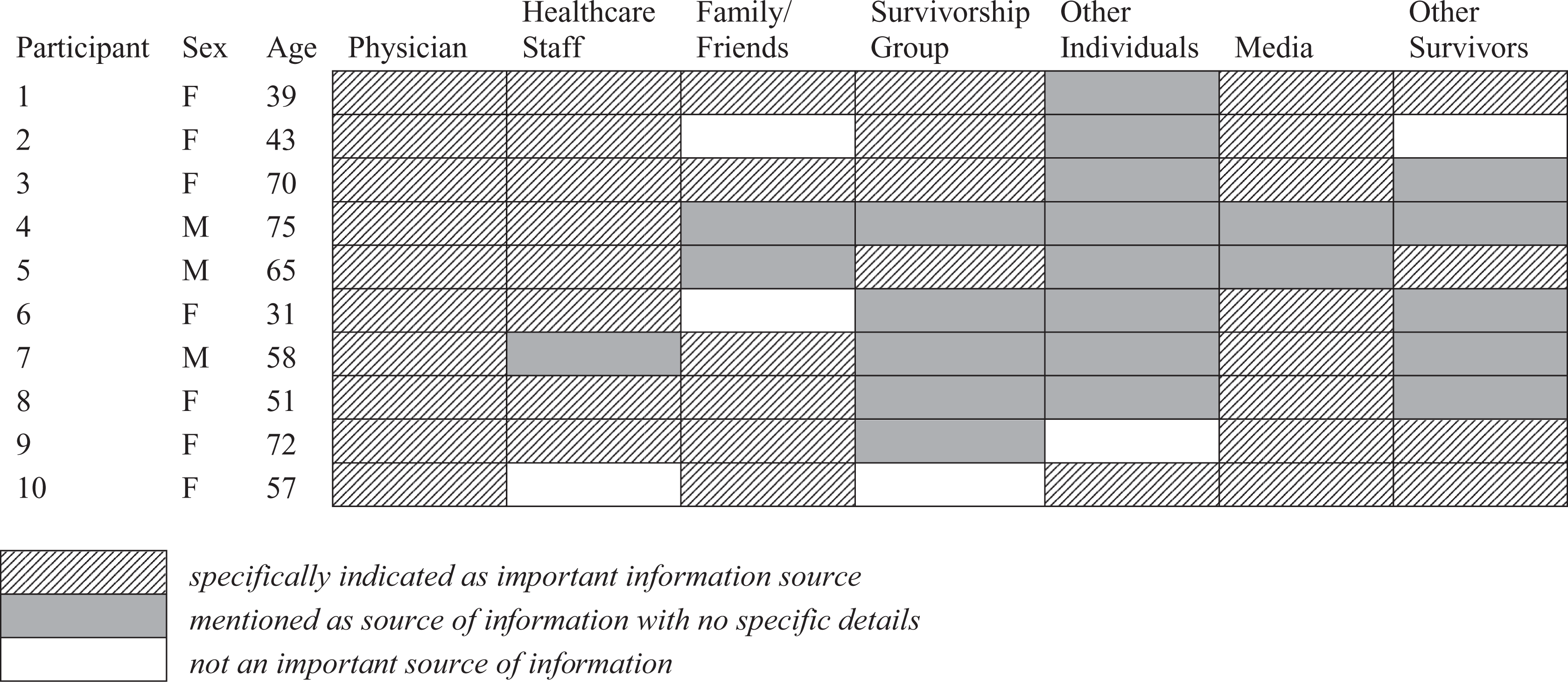
Sources of prognostic information for participants.
Health-Care Staff
Participants mentioned multiple people with who they interacted regarding their prognosis within the health-care setting, including nurses, nurse navigators (specifically assigned to oversee participants’ cancer care), social workers, psychologists, nutritionists, and/or outside specialists (eg, primary care physician [PCP]).
Almost all participants perceived nurses as critical sources of information and often sought them out more than physicians for input and advice. This may be attributable to the fact that interactions with nurses are more frequent during treatment; hence, ample communication opportunities were present. The perception that nurses were better equipped and had more time to empathize and understand their concerns was common. Nurses also seemed to provide more insight into the details of what to expect during and after cancer treatment: “The nurse was able to pinpoint (possible problems)…She could give me a better idea of specifically what to expect” (participant 6). Several participants recommended that nurses should be assigned to discuss aspects of prognosis instead of the physician.
Notably, nurse navigators often played a pivotal role for participants in understanding and interpreting their experience. Several participants noted the importance of having a nurse specifically dedicated to their care who was knowledgeable about the information communicated to them by treating physician(s) and staff regarding their treatment, care, and prognosis.
Additionally, PCPs were seen as salient and trusted sources of information with a long-established relationship. Some participants turned to their PCPs when they experienced communication difficulties with their treating physicians (eg, felt ignored or complete communication breakdown).
Although not as common, other staff (especially social workers and counselors) also played important informational roles for some participants by addressing practical concerns (eg, financial worries and effects on family or relationships), providing emotional support, and providing key information about treatment, side effects, available resources, or how to prepare. In some instances, these staff encouraged participants to elicit more information, ask more personally relevant questions, and probe for more information in discussions with physicians.
Family/Close Friends
Family and friends were also significant informational sources for the majority of participants. Often, these individuals became “researchers” who sought out information that verified or added depth to what they were discussing with their physician. This meant playing an active role in listing relevant concerns/questions, understanding information that was received, and seeking additional information. Participant 1 said her husband sought out information on treatment, side effects, and other concerns. Sometimes, this information was then brought to her physician, but in other cases, she felt such discussion unnecessary. Participant 2’s mother attended the “tumor board,” where her particular case was discussed by a team of physicians. Her mother then informed her of the tumor board recommendation, which was different from her preferred course of treatment previously discussed with her surgeon. This played an important role in her decision to choose an alternative course of treatment than the initial board recommendation.
The role of “researcher” also meant exploring other options or informational avenues, which the physician either did not or would not discuss. Participant 7 described his own research process involving his friend (who was being monitored for similar cancer). They would each collect research about his particular form of cancer and then compare to what his physicians were saying: We started collaborating right away…. He came to all of my appointments and did heavy research at the same time that I was doing at the beginning. That was extremely helpful.…. It is very useful to have a second set of ears…. I got big benefit[s] from doing strategy with my friend.
Other Survivors
Other survivors were also noteworthy sources of more specific/relevant information, often in the beginning when major decisions needed to be made: “[I talked with my survivor network] mostly very early on when I was trying to figure out my way through” (Participant 9). In other instances, other survivors became important later, especially as participants were dealing with unexpected side effects or aspects of their treatment. Significantly, other survivors often provided specific medical information: “I was finding out what happens when you’re on this medicine or that medicine…In some cases, I’m finding my medical answers nonmedically” (Participant 1).
They also seemed to provide more detailed information about what to expect, especially when they had similar diagnoses. Participant 7 was able to gain insight into what his situation may be like in the future through these interactions: “[It was helpful] to engage with people who had the longer term experience. People who could tell me what it’s like to be alive 2 years after getting a [similar diagnosis].” Having similar experiences also seemed to make it easier to trust these individuals and the information they provided. Participant 5 described taking a struggling local survivor to meet another survivor who had undergone the same surgery he experienced years before. He noted the camaraderie, trust, and support his friend derived simply because this was the “first time he was in a room with 2 other people who had his surgery.”
Survivorship Groups
The format of a survivorship group was a unique supplemental source of information mentioned by several participants. Although survivorship groups necessarily entailed interacting with other survivors (see above), some participants only interacted with other survivors in this context. Alternatively, some participants did not utilize these groups at all. Survivorship groups were relevant resources particularly for gathering the perspectives and advice of several survivors at once, as well as discussing and interpreting their experiences and concerns in a group format. Participant 4 mentioned that one strength of his group was the ability to add “depth” to the information given: “to help people make sense of some of the things that they’re hearing.…If they’re having difficult times, to be a good ear. To be a caring listener and responsive to that. Helping them navigate that whole experience.”
Media
There were many different media sources that participants went to for information. These included Internet sources, books, survivor blogs, and cancer discussion forums. Often, these were sources of information that complemented or reinforced what the physician was communicating. However, there were participants who employed these resources to find alternative or additional information they were not receiving from their physician. Media sources also seemed to aid in managing the amount of information participants were receiving, allowing them to focus on details relevant to particular concerns at different moments: “I remember that I would digest the information as I needed.…I was pretty focused on ‘what do I just need to handle now?’ so that it wasn’t overwhelming” (Participant 8).
In some instances, these resources helped to streamline familiarization with the treatment process and concerns or questions patients typically have. They also helped participants make sense of the information that they were receiving from their physician and nurses. Participant 6 mentioned that she found the materials (pamphlets and websites) she received at the hospital useful, but was concerned that they were too general. This caused her to seek more specific data through the Internet. Several participants mentioned that the information they found was not always useful, and sometimes caused more concern. In spite of these risks, participants expressed that this information gave them more understanding of their situation and what to expect, and aided in decision-making and communicating with their physician.
The blogs and forums for other survivors served similar functions providing deeper insight into the treatment experience, finding solutions to questions about side effects, learning of new treatments or addressing treatment concerns, and seeing what to expect down the line.
Other individuals
This category is the broadest category, including a wide range of individuals or sources: acquaintances or strangers, hospital staff not directly involved in treatment, survivor events or activities run by the hospital (eg, art therapy, yoga), church/religious groups, and community connections (eg, a child’s teacher, hobby groups).
These informational sources often focused on long-term side effects of treatment as well as other concerns that arose after completing treatment. Often, these individuals did not have personal experience with cancer but were connected to someone who did. This meant that they provided information that was somewhat further removed or could connect participants with other survivors or helpful resources. Participant 10 mentioned a discussion with her boss whose wife had been treated for cancer: “He was informed enough and said, ‘Well, you know, my wife does this.’ He didn’t feel the need to [pry or tell me too much].” Participant 2 emphasized the same thing with the “yoga for survivors” instructor who had not had cancer. Her awareness of the concerns of survivors she had encountered allowed her to provide insightful and helpful support.
Discussion
Importantly, all participants expressed or emphasized the use of (and benefit from) different sources of information in understanding their prognosis. Some participants centered on one particular group, while others sought out information more evenly among several different sources (Figure 1). Additionally, each participant discussed aspects of their prognosis with at least one other person outside the communication with their treating physician (including strictly medical aspects; eg, side-effects and medical resources). These interviews provide a glimpse into the process patients undertake to interpret and understand their prognosis and (more broadly) their experiences with cancer treatment. The information that participants employ is certainly informed by the physician who holds authority over many aspects of care. However, our study suggests that in understanding prognosis, patients bring to bear information they have received from potentially many other sources, including family and friends, other survivors, and various media sources. These interactions and the information received from them can affect how a patient with cancer understands their experience and what they should expect (their prognosis). Specifically, as patients are incorporating pieces of information that differ from the treating physician’s perspective (about which the physician is unaware), it can contribute to increasingly divergent understandings of prognosis between physician and patient.
More generally, several participants discussed the idea that they experienced a sense of 2 different worlds relative to their cancer experience and physician communication. These were roughly described as medical and nonmedical worlds, each with its own pertinent concerns but which, to participants, felt interconnected. Participant 1 described this as “finding my medical answers nonmedically.” Participant 6, a nurse, saw this in the impact of being treated for cancer on her understanding of the patient experience: “It’s definitely changed how I am as a nurse and how I handle [working with patients]…. You get a report on a patient and they’re a list, a history. It’s easier now for me to see, to realize that I’m really stepping into someone else’s, I’m sharing someone else’s reality. And it’s more than just a list of diagnoses.”
At times in their communication, participants noted frustration with the inability to bridge these 2 aspects of their care simply because their physician seemed either unwilling or incapable of effectively navigating both worlds. Although sympathetic to the difficulty this poses, Participant 9 stressed the need for doctors to “figure out how to meet the person that’s in front of them.” Participant 7, who relied heavily on his friend for information and advice, described this frustration as needing to navigate “more than one kind of communication going on here” to be able to address his different needs.
Our study suggests that prognosis communication is a moment where these 2 different worlds tend to overlap significantly. This may stem from the tendency in prognosis communication research to differentiate between medical aspects of prognosis and other aspects of prognosis. 21,31 Our study suggests that for patients, the line between what is “medical” information and what is “nonmedical” becomes increasingly unclear. Alternatively, prognosis (and the understanding of a prognosis) can be understood as being a process of communication/information gathering that is connected to (and affected by) factors that fit within both medical and nonmedical realms (cf, the definition of prognosis advocated by Clayton et al 20 ). This medical/nonmedical overlap has the possibility of placing any number of different individuals or other sources alongside the treating physician as authoritative sources for prognosis information in the patient’s view. 33,34 In describing the significance of other external sources of information and support, participant 1 noted that “I would be very worried about myself if I didn’t have the external support that I have. Because [in the medical team] there’s little overlap in all of that:…understanding the invisible side effects,…and being supportive about all the other things that this affects.” Friends and family, Internet and print sources, survivorship groups, and other survivors all contribute relevant information that can inform how an individual with cancer understands their experience and what they can expect. Furthermore, because prognosis entails such a wide range of personal and interpersonal aspects, it is no wonder that patients feel that their doctor should not be the only individual who is providing them perspective, advice, and information throughout the cancer experience.
Limitations
We had a relatively small sample size with breast cancer being overrepresented. It was clear that although experiences were similar, the different cancer types often came with unique prognosis concerns. We were unable to capture this diversity with our sample. Additionally, we recruited participants from a cancer center focused on individuals with breast cancer who often had different interactions and communication with hospital staff.
Because communication about prognosis was discussed in retrospect, there may be some recall bias. Although most participants (7/10) had finished treatment within the past year, 3 participants had finished cancer treatment 3+ years in the past. This may have affected their recollection of the details of their experience.
Finally, our participants tended to be middle-aged adults or older adults (2 participants were under age 40; Figure 1). Generational differences may have influenced how participants communicated with physicians as well as their expectations regarding physician roles and good communication with their physician.
Conclusion
Focusing on patient–physician communication is insufficient to capture the complexity of interactive communication moments that go into a patient’s understanding of their prognosis. 34 Prognosis cannot be understood as solely a medical consideration, the physician’s domain. In order to understand how physicians and patients come to acquire differences in their understanding of prognosis, it is important to consider the process a patient undergoes to interpret their experience and prognosis, including especially the different sources of information they turn to for added perspective and information. 33
This means that physicians and treatment teams should consider their patients’ processes of negotiating the meaning of their prognosis. This entails situating their own authority and contribution (however expansive or limited) within a broader array of other sources available to their patients that they see as authoritative regarding various aspects of their experience and prognosis. In particular, in some instances, nurses may be better equipped to elicit, understand, and address concerns and questions that may arise during treatment. Patients may sometimes prefer to communicate with nurses instead of physicians. Utilizing nurses (and, more generally, other members of the health-care staff) to carry out these discussions can be an effective way to assess patient understanding and tailor information to specific patient concerns and questions. We also suggest being more generally attentive to the dynamic nature of what a prognosis “means” to individual patients. This should be considered as discussions of treatment options and plans, measures of treatment success/failure, survival, and decision-making are taking place. This may simply encompass checking in with patients at various points (and more frequently) throughout treatment to reengage relevant aspects of prognosis, reevaluate patient understanding, and recommunicate the physician’s perspective. Additionally, because patient understanding can be uncoupled from the information disclosed by their physician, informed consent may entail an ongoing process and not just a single communication event. This has implications for the practice of obtaining informed consent in these contexts.
Supplemental Material
Appendix_A - Cancer Communication Outside of the Physician-Patient Relationship: The Experience of Communicating and Understanding the Meaning of Prognosis
Appendix_A for Cancer Communication Outside of the Physician-Patient Relationship: The Experience of Communicating and Understanding the Meaning of Prognosis by Matthew Adamson, Crina Cotoc, Kelsey Choi and Stephen Notaro in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
We sincerely thank the 2 anonymous reviewers for their constructive feedback, which improved the manuscript. In particular, we acknowledge one reviewer’s contribution regarding the relevance to informed consent as mentioned in the conclusion.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.