
Abstract
Palliative care services are increasingly required to consider issues of resource, management as demand for services increases. The processes of triage have been developed in health care as a means of balancing need and resources in an equitable and reproducible way.
Objective:
This article sought to explore ethical issues associated with prioritization decisions in palliative care.
Methods:
As part of a broader series of studies of triage in palliative care, this qualitative substudy was conducted via semi-structured focus groups and individual interviews. Transcripts were subjected to thematic analysis.
Setting/Participants:
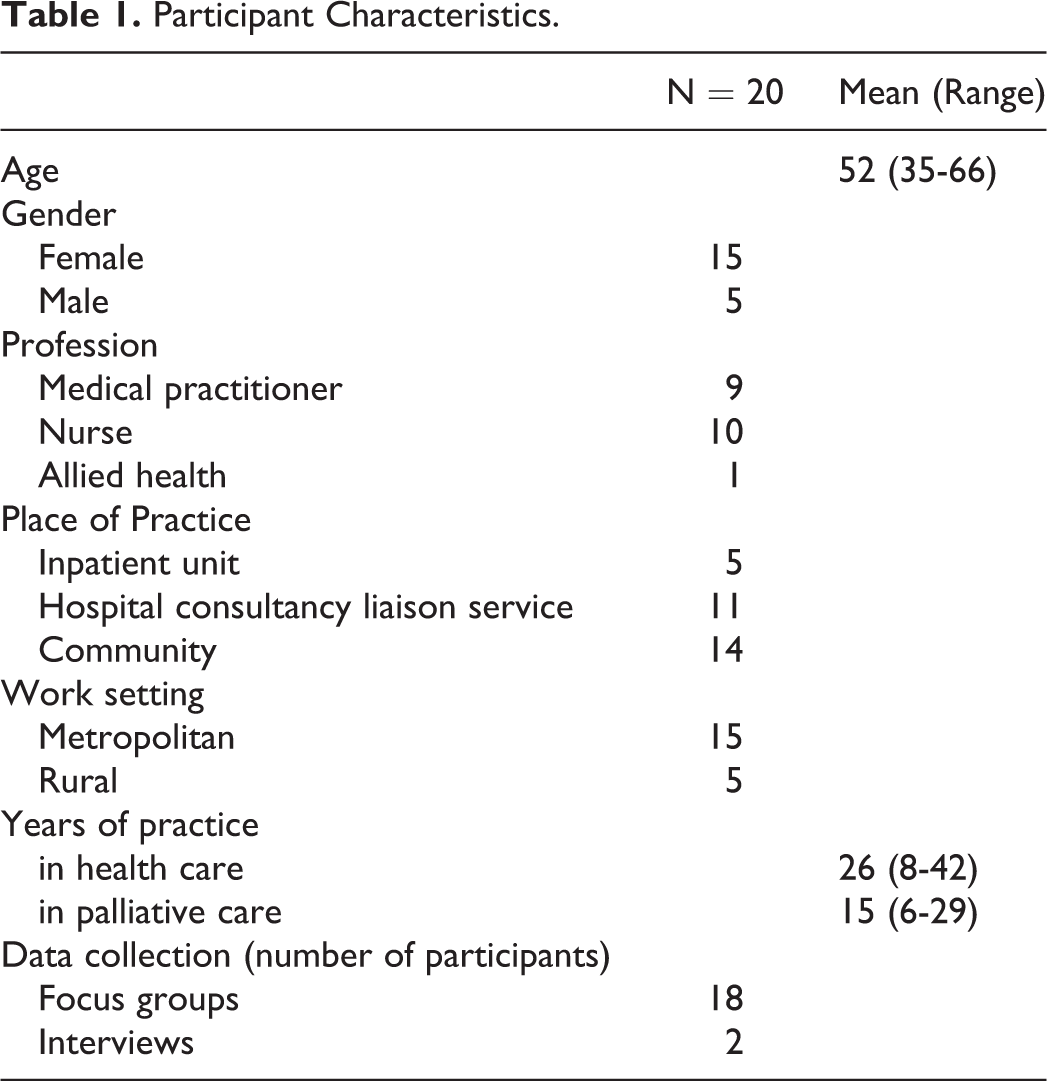
Twenty health professionals working across disciplines (primary, specialist; medicine, nursing, and allied health), service types (inpatient, hospital liaison, and community), and locations (metropolitan and rural) in Victoria, Australia.
Results:
Four themes emerged from the data: (1) Clinicians understood the tension between maintaining service quality with the delivery of a compromised service that sought to respond to demand. (2) They were aware of the influences of relationships and responsibilities upon patient waiting list prioritization, and (3) reported a hierarchy of suffering with certain types of clinical problems viewed as more urgent than others, for example, pain being more urgent than existential distress. (4) Clinicians noted a lack of transparency around waiting lists as they currently exist.
Conclusions:
This study revealed key ethical decision-making issues associated with prioritizing access to palliative care services. Making explicit the processes and influences upon decision-making provides greater transparency of health-care utilization at the end of life.
Introduction
Triage systems and waiting lists have been widely adopted in health care across both emergency and nonemergency settings. The process of triage and the use of waiting lists are intended as a means of balancing need (including seriousness and urgency) and resources in an equitable way. 1 Extensively described in the care of patients in disaster and emergency care, 2 –4 the principles of triage have also been applied to nonurgent areas of health care and underpin the establishment of waiting lists in publicly funded health systems. Iserson and Moskop have suggested there are 3 conditions of triage in health care: (1) a scarcity of resources; (2) a health worker (triage officer) who makes a, usually, brief assessment of a patient’s needs; and (3) the use of an established system or framework to determine priority for each of the patients. 1 Triage is frequently conceptualized ethically as an example of distributive justice, where access to treatment is made available to those with greatest needs who will most benefit across a population. Since it may not be possible for everyone with needs to immediately access the required form of health care, triage systems have been developed to facilitate care allocation.
The conditions of scarcity are evident in palliative care with increased demand for palliative care services internationally meaning a number of services establish waiting lists to manage responses within the available resources. 5 The use of waiting lists in the care of patients with advanced disease has received little attention, with little discussion of the decisions underpinning these waiting lists, namely, decisions around access, urgency, and competing needs. We have sought, as part of a broader program of work, to develop a triage tool for palliative care services. As part of this triage tool development, we undertook a qualitative study to explore palliative care providers’ practices toward triage 6 and their views of what should be included when assessing urgency in their patients’ care. Through this qualitative exploratory work, a series of moral challenges were highlighted which throw focus upon the nature of ethical decision-making underpinning triage in palliative care. This article seeks to explore the nature of these ethical challenges in palliative care triage according to health-care professionals.
Methods
This current qualitative study is part of a mixed-method program of work also involving discrete choice experiment methods and validation studies toward the development of a triage tool. In this qualitative study, exploratory semi-structured interviews and focus groups were conducted with health-care professionals. The methodology, described in detail elsewhere, 6 entailed a stratified purposive sampling strategy to ensure participant representation of specialist palliative care providers across disciplines (primary, specialist; medicine, nursing, and allied health), service types (inpatient, hospital liaison, and community), and locations (metropolitan and rural) in Victoria, Australia. Specialist palliative care services in Australia are publicly funded, referral-based services available to patients who are based in acute hospitals, palliative care inpatient units, and in community care settings. Service managers invited key staff for participation who had current clinical palliative care responsibilities and at least 2 years of clinical experience. Questions to both focus group attendees and interviewees, detailed in Box 1, explored participants’ practices around triage in palliative care and the factors they considered important to decision-making in access to palliative care services. All participants provided written informed consent, and recruitment continued until saturation of themes were reached within the data. The study was approved by the St Vincent’s Hospital Melbourne Research Ethics Committee (LRR: 161/14).
Questions Guiding Semi-Structured Focus Groups and Interviews.
Thinking back to the last patient you were involved with who had palliative care needs, which aspects of their case made you think they did or did not require urgent specialist palliative care?
If not already discussed, specifically prompt discussion regarding: – Symptom severity (physical and psychological) – Phase of disease – Performance status – Prognosis – Caregiver issues – Care environment – Requirements for daily hygiene or syringe driver – Potential for catastrophic events
Are there any other factors that you find helpful to determine the urgency of your patients’ palliative care needs?
Are there times when these concepts we’ve discussed might interact or overlap in the patients you see?
Imagine a triage system was going to be implemented in your workplace. What impact do you think this would have?
What potential barriers or enablers do you foresee to such a system?
Can you describe some of the challenges that you have come across when making decisions about which patient to see first/admit first/respond to first in your work?
Any things that make it easier or more straightforward?
Discussions were recorded and transcribed, with the transcripts analyzed independently by 2 researchers (B.R. and J.P.) using a thematic approach. A coding framework generated from the literature facilitated the organization and development of themes, which were then reviewed, discussed, and refined by the investigator group. The investigators included palliative care doctors, psychologists, and researchers and consisted of both those with and without relationships to the participants. The primary analysis detailed the hierarchy of patient-level factors considered when assessing urgency of need, with a view to triage tool development. 6 In addition, the analysis revealed a series of themes relating to ethical concerns raised by participants in the context of decisions made affecting resource management at the end of life. These themes are the focus here.
Results
Four focus group discussions were held with 18 participants and supplemented by 2 interviews for those who expressed interest but were unable to attend focus groups, giving a total of 20 participants (Table 1). The participants described a constellation of ethical issues arising when considering palliative care triage and practices, which were characterized into 4 key themes: (1) A quality service versus some service with questioning around acceptable levels of service compromise when responding within constrained resources; (2) The hierarchy of the causes of suffering when weighing triage decisions; (3) The influence upon urgency of nonclinical factors (such as, needs of the health service and its operation, the influence of personal relationships); and (4) The lack of accountability around waiting lists in palliative care. These themes are discussed below in turn, with exemplar quotes from participants, representing the ethical dilemmas considered by palliative care professionals in the practice of triage.
Participant Characteristics.
1. A Quality service versus Some service? What level of service is “good enough” when responding within available resources?
The assignment of urgency or systems of triage are only required when there are limitations in the available health resources including time, staffing, and beds available. Attempting to provide patient care if resources are not available will inevitably impact upon the comprehensive nature of the care provided. The participants noted that responding to ever-increasing number of patients within the same resources meant quality of care would be reduced. In short, palliative care would be “spread too thin” (Nurse). When managing within available resources, participants noted that some minimum standards of care must be maintained to ensure specialist-level palliative care was being delivered. At some point, the stretching of available resources to meet all demands could no longer be sustained if, by doing so, care became too compromised. The question raised by health-care professionals was what level of compromise was no longer acceptable and what constituted this minimum standard of specialist palliative care? You can see the need…but…if you haven’t got the staffing…you’re not going to put a good service in by trying to put together a patched-up one. (Nurse) Is (the care) adequate?…well, it’s not quite perfect, so is it adequate? (Doctor) 2. The hierarchy of the causes of suffering when weighing triage decisions.
Among participants, there was suggestion of a hierarchy of clinical problems, with physical symptoms taking priority over psychological and spiritual concerns. Such a hierarchy challenges the holistic approach to palliative care which acknowledges the importance of the “whole person experience” and the primacy of the patient’s reporting of that experience. While the participants (predominantly doctors and nurses) acknowledged the importance of other forms of suffering such as anxiety or carer distress—among other psychological and spiritual concerns—the physical symptoms were prioritized when it came to access to palliative care services. I think we’ve always been taught…that to try and manage the physical symptoms will then allow the person to actually be able to embrace some of the other stuff that’s going on. (Nurse) We would probably respond quicker to someone with pain and nausea because you can fix it with an injection…There’s no point getting out there quickly if we can’t do much when we get there. (Nurse) But for someone that’s got chronic dyspnea, (that is)…not so urgent compared to some other things…If it’s…COPD then we know that that person’s used to living with a certain amount of shortness of breath or distress. (Nurse) 3. The influence upon urgency of nonclinical factors.
When making decisions about admissions to palliative care services, clinicians noted they were required to balance the patients’ needs and simultaneously be responsive to, and helpful within the health system more broadly. We’re meant to be doing patient-centered care…and yet that it’s never as simple as that…Is it more ethical to admit the patient in crisis or to empty a bed on the hematology ward so that someone who has the potential to be cured can…be admitted to get their life-saving treatment? (Doctor) We have to consider…the needs of the team, you know (Doctor) Sometimes…if the intensity or severity of the problem is very high, it can almost count against you as a referrer because the receiving agency actually knows they’re going to need more resources in order to respond to this referral. (Nurse) You’ve got a favorite oncologist in a local private hospital and you give priority to his patients…I think—occasionally it’s inevitable. In a weak moment, you know, “Yeah John, sure.” (Doctor) If it’s a colleague (who is the patient)…people are going to bend over backwards. (Nurse) It’s very complicated…When you send someone off to have their radiotherapy and you’ve got to readmit (when treatment is complete)…You’re obliged to take them back. (Doctor) 4. The lack of accountability around waiting lists in palliative care.
Participants highlighted concerns that waiting lists may be used as a means of responding to demand without the expenditure of resources. Assigning a patient to a waiting list may give providers the (false) assurance that they have responded to the referral when, in fact, no response has been meaningfully implemented from the patient’s perspective. Patients on a waiting list received no care and therefore did not use any significant service resources until the time they were admitted. There appeared to be a lack of responsibility for patients who were on a waiting list, including if adverse events occurred for such patients, since they were not yet admitted. Who’s going to answer the questions when…people on the waiting list…had an adverse outcome because they were on the waiting list? (Doctor) It has to be informed consent to the people on the waiting list, that…they know what it means, what will happen. (Doctor) I’m sorry Jack, I’d like to help but the waiting list says…(Doctor) Should you (even) have a waiting list? That’s a really important question. (Doctor)
Discussion
This study reveals the complexity of ethical factors considered in decisions made by clinicians, as they balance competing needs of patients requiring palliative care. While such decisions are based primarily on the immediate patient needs, these needs exist and are interpreted within the framework of systems of care and networks of relationships, with decisions reached therefore a composite outcome of all these factors. Such a decision may reflect the particular patient problems such as the man with pain being seen before the man with emotional distress, or it may reflect simultaneously the broader health-care system requirements whereby prioritizing one particular patient will enable freeing of resources elsewhere in the system. The discussion of these factors, to our knowledge, has not been previously documented.
The delivery of care that is compromised has been highlighted in this study as a source of concern by clinicians, as they grappled with the idea of what constitutes the minimum standard of specialist care. If adequate resources are not available to deliver this minimum standard of care, perhaps such a patient should not be treated in palliative care at this time? Yet, what constitutes the minimum standard of palliative care and is that worse than no palliative care? Best or ideal palliative care has been described as involving the establishment of a relationship, setting goals, comprehensive communication, acceptance, advocacy, flexibility, symptom relief, and recognizing the identity of each person. 7 Challenges to achieving this ideal standard of care have been noted to include (at times) the particular demands of families, for example, who demand burdensome futile treatments, of other health professionals, of administrative structures and as a result of conflict. 7 The limitation of resources as a challenge to provision of ideal care as raised in this current work is an important additional factor to consider. As resource limitations are often reached in a gradual cumulative manner, the care compromises resulting may likewise accrue in small steps and therefore may not always be apparent to clinicians involved. The ability of health professionals to be vigilant of incremental change to their aspirations for care should be encouraged, enabling them to pause at times and reflect upon the changes occurring as they navigate real-world practicalities of providing care. The other dimension of providing less than idea care is the moral distress which may result. Weissman has noted that moral distress of clinicians may be evoked by “being unable to act upon the ethically appropriate course of care, due to external or internal constraints.” 8 A vigilance to the moral distress which may result from decision-making in the setting of insufficient resources, and the ensuing potential for avoidance and burnout is also a key responsibility of palliative care teams as they support each other. 9
The priority given to physical symptoms raises interesting challenges for palliative care which, as highlighted in the World Health Organization definition, seeks to address all aspects of suffering, including physical, psychological, and spiritual. 10 The participants in this study were almost all doctors and nurses, and this may influence how they consider this hierarchy of needs, while other clinicians such as spiritual care workers may prioritize these needs differently. Despite the tenet of palliative care to attend to the whole person, in times of increased service activity, it appears that practitioners struggle to equally recognize nonphysical versus physical symptoms when determining urgency of response. 11 A series of reasons may underlie this implicit preference, including the perceived time taken to address nonphysical symptoms, 12 the health practitioners’ confidence in addressing certain areas of care, 11 and the overt and therefore confronting nature of some physical symptoms compared to sometimes less demonstrably overt psychological and existential suffering. 13
It is unsurprising that there are clinician values—professional and personal—which underlie decisions assigning urgency to patients requiring palliative care and which play an important role in addition to the particular needs of the patients themselves. These values are evident in the influence of relationships with colleagues, with the systems of care and the patients and families themselves. 14 These values need not necessarily be considered “wrong” or held in error. For example, the priority given to readmitting a previously cared for patient who has now completed a course of radiotherapy at another facility means that not only will that particular patient receive ongoing, appropriate care but relationships remain in place such that future patients who may require radiotherapy will be readily accommodated. All of health care is conducted within a network of relationships, and these relationships can facilitate care. 15
Nevertheless, consciousness of this potential for bias as decisions are made around prioritization of access to care, with commitment to acknowledge and make these relationships and influences explicit should occur to ensure transparency to all involved. Attention to such transparency may go some way to improving the accountability to patients who are “on” a waiting list, as the processes are explained and the decision-making made explicit. Information around what is available, and perhaps more importantly, what is not available to those who wait, should be part of this transparency process.
This study included a robust sample of palliative care providers who gave rich insights into the ethical concerns surrounding the practice of triage in palliative care, and for some, the novel concept of introducing waiting lists in response to rising service demand. The participants’ views reflect their own experiences, and, consistent with the qualitative methodological approach, may not be widely generalizable or represent the ethical dilemmas faced by all palliative care services. Nonetheless, these experiences reveal several important considerations underpinning the complexity of triage in palliative care, and provide a framework in which to understand the future implementation of the prospective triage tool.
Conclusion
The concept of prioritization and rationing of resources in health care, beyond surgical waiting lists and triage in emergencies, receives little public discussion in developed economies. In areas of sensitivity such as the care of the dying, such discourse is largely silent. Nevertheless, palliative care services have seemingly developed internal systems of balancing demands and available resources, although in most services these systems are not explicit, including, frequently, to the health-care professionals working within the services.
The assignment of urgency in palliative care and the institutionalization of this in the form of a waiting list holds implicit ethical content which requires consideration. We contend that by making this ethical content explicit, palliative care services will be well placed to navigate the challenges of resource allocation and, through the process of discussion, simultaneously support the clinicians providing care.
In particular, such challenges to be highlighted include the influence of professional comfort with different domains of care provision and the impact of personal and professional relationships require highlighting. The reasons and service imperatives for establishing a waiting list, the responsibilities to those who are listed and how this is communicated must all be considered. Similarly, systems must be in place to make the influences of relationship transparent. All these decisions must be explicated and justified. Services that engage in an exploration of the ethics of palliative care resource management have the potential to enhance communication, transparency, clinician support, and, ultimately, patient care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Received grants from Department of Health & Human Services, Victorian Government, and Research Endowment Fund, St Vincent’s Hospital, Melbourne.