
Abstract
Interest and appreciation for palliative care (PC) has resulted in increased demand for both PC services and education. The PC rotation has been shown to improve PC knowledge in medical students (MS) and internal medicine (IM) residents, and PC specialists stand poised to direct the primary PC education of learners at different levels of training. To concurrently teach learners of different levels of training on a busy PC service, we created an educational system that emphasizes management of learner schedules, organization of teaching activities, faculty development to improve teaching skills, and learner self-evaluation. Both MS and IM residents showed an improvement in self-assessed competence as well as increased comfort level with seriously ill patients after PC rotation. Careful adjustment of learner schedules has accommodated an increasing number of learners, while maintaining a low learner to faculty ratio. The PC educators face an exciting and daunting challenge as the number of patients with PC needs and the number of learners requesting PC experience grow. We continue to improve milestone-based PC assessment tools, to invest in faculty development, and to explore innovative ways to support PC educators as they strive to provide consistent PC education that is both useful for learners and can be incorporated into busy PC clinical practice.
Keywords
Introduction
Interest and appreciation for palliative care (PC) has resulted in increased demand for PC services by clinicians, patients, and health-care systems. Despite the increase in PC programs and the number of specialty-trained PC clinicians, there remain too few PC specialists to meet the current and future PC needs of an aging population. 1 The PC rotation has been shown to improve the PC knowledge of medical students (MS) 2 and internal medicine (IM) residents, 3 and many PC specialists are working to balance increased teaching responsibilities. Despite having little formal education in teaching, 4 PC specialists stand poised to direct the primary PC education of learners at different stages of training. 5 In order to concurrently teach learners at different levels of training on a busy PC service, we created an educational system that emphasizes management of learner schedules, organization of teaching activities, faculty development to improve teaching skills, and learner self-evaluation.
Methods
In July 2012, we restructured our PC educational program to create a robust and consistent learning experience for learners at different levels of training. Prior to the restructuring, learners worked with PC faculty but formal didactics and learner experience was variable. Study data were collected and managed using REDCap electronic data capture tools hosted at Vanderbilt University. 6 The institutional review board (IRB) approved the collection of preassessment and postassessment data from the learners under exempt status (Vanderbilt IRB #121669).
Management of Learner Schedules
As schedules grow more complex with both increasing team size and an increasing number of clinical sites, our PC education system has been able to accommodate more learners while ensuring that each learner is able to rotate at different sites of training and work with different members of the interdisciplinary team (IDT; Table 1). To add to the complexity of the scheduling, the PC faculty and IDT rotate through different sites of practice which include an academic hospital consult service (2-3 faculty physicians, 1 PC fellow, 1-2 advance practice nurse practitioners, 1 nurse case manager, 1 chaplain), an academic hospital PC unit (1 faculty physician, 1 PC fellow, 1 nurse case manager, 1 social worker, 1 chaplain), a Veterans’ Administration hospital consult service (2 faculty physicians, 1 PC fellow, 2 advance practice nurse practitioners, 1 clinical psychologist, 1 social worker, 1 chaplain), community hospice (home visits with nurse or chaplain), and outpatient PC clinic (1 faculty physician, 1 advance practice nurse practitioner, 1 chaplain, 1 social worker).
Sample Learner Rotation and Education Activities Schedule.
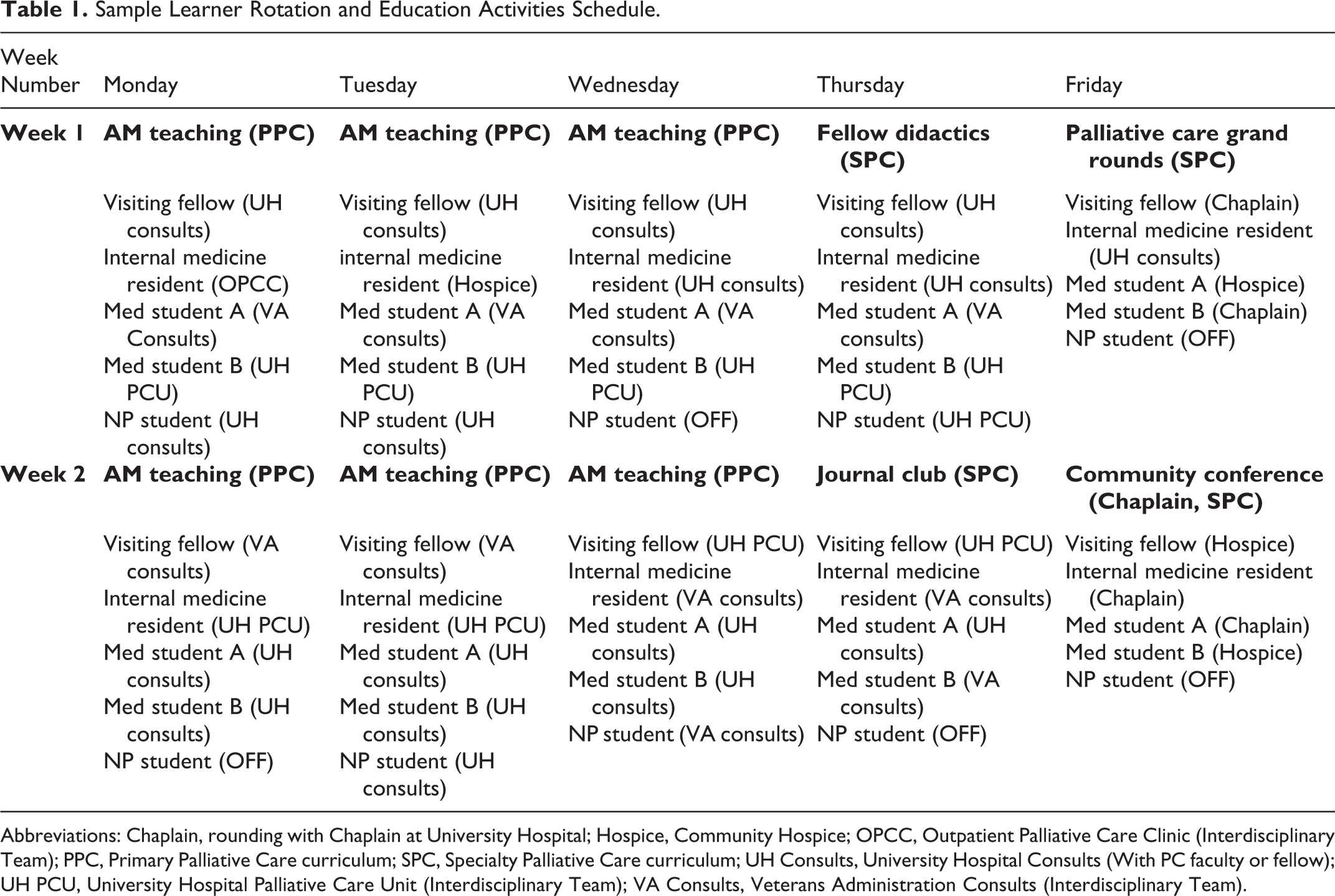
Abbreviations: Chaplain, rounding with Chaplain at University Hospital; Hospice, Community Hospice; OPCC, Outpatient Palliative Care Clinic (Interdisciplinary Team); PPC, Primary Palliative Care curriculum; SPC, Specialty Palliative Care curriculum; UH Consults, University Hospital Consults (With PC faculty or fellow); UH PCU, University Hospital Palliative Care Unit (Interdisciplinary Team); VA Consults, Veterans Administration Consults (Interdisciplinary Team).
We create a calendar in March for the upcoming academic year, which allows us to account for different academic schedules and to accommodate learners on a rolling basis throughout the year. In general, we plan to accommodate 1 visiting fellow or resident (a person who has completed a residency or who is not in an IM resident, rotations between 1 and 4 weeks), 1 IM resident (2-week rotation), 1 second-year MS (2-week rotation), and 2 third- or fourth-year MS (4-week rotation). We usually average 3 to 9 learners per month, approximately 50 learners per academic year.
One month prior to the start of the rotation, learners are asked to confirm their attendance and give scheduling requests. This information is used to create a learner schedule that optimizes faculty to learner ratio and that provides individual learners time at different sites of practice. Weekly group e-mails contain the learner rotation site and didactic schedule for the upcoming week and assign learners to the PC faculty member with whom they will work. Careful arrangement of learner schedules has allowed us to have 1 to 2 learners per faculty member (Table 1). It is important to note that these numbers do not include our PC fellows. We teach PC fellows at all sites of rotation concurrent with the above learners, accommodating fewer visiting learners at the beginning of the academic year in order to engage fully with new PC fellows and allowing more visiting learners later in the academic year as PC fellows gain more independence.
Organization of Teaching Activities
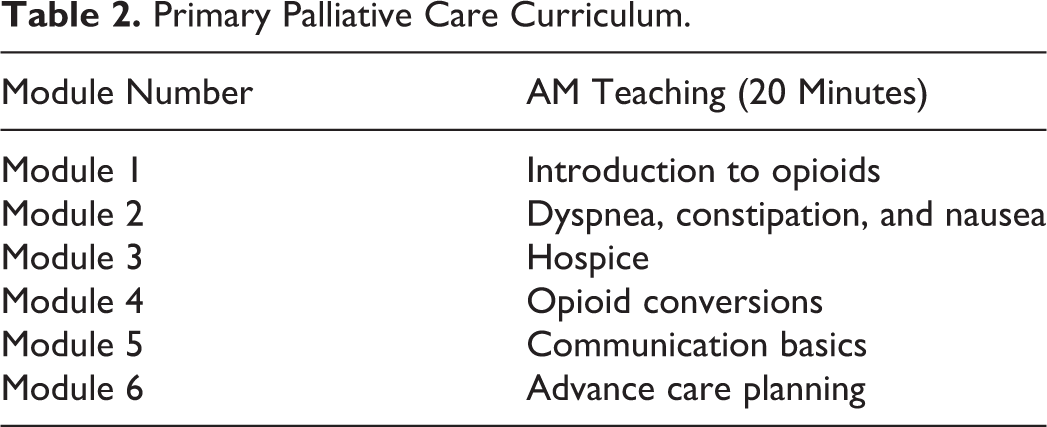
One of the most popular elements of our educational system is a primary PC curriculum that consists of 6 core primary PC modules and is taught 3 days per week for 20 minutes per session (Table 2). Before the beginning of daily clinical work, all learners and PC fellows meet to review a module; the schedule is repeated every 2 weeks (Table 1). The content was developed by our PC fellows as a quality improvement project and consists of a standardized PowerPoint presentation attached to the weekly scheduling e-mail. This primary PC curriculum is taught by PC faculty for the first 2 months of the academic year with the PC fellows as learners, followed by 1 month of PC fellows teaching with faculty observation and getting feedback on teaching skills. The PC fellows then teach for the remaining of the academic year. Learners are encouraged to review the content prior to the session, so meeting time can be used to answer questions and discuss clinical scenarios.
Primary Palliative Care Curriculum.
The remainder of the didactic sessions throughout the week is dedicated to specialty PC content, and all learners are encouraged to attend all learning opportunities (Table 1). This educational system allows time for both primary PC content and specialty PC content throughout the week, thereby addressing the educational needs of visiting learners, PC fellows, PC faculty, and PC IDT members. The week’s didactic schedule is included in the weekly scheduling e-mail.
Each learner’s expectations, experiences, and assignments for the rotation are based on a combination of accreditation council for graduate medical education requirements from their home program and PC faculty experience with learners from that discipline. For example, all learners start their rotation by shadowing PC faculty and then are assigned graded responsibility for patient encounters. Medical students are expected to write patient history and physical with emphasis on spiritual and social needs, to research a focused question pertaining to a PC patient encounter, and to reflect on their time with the chaplains. Because of the one-on-one time with clinical faculty and chaplains, faculty can debrief after difficult or intense patient encounters and can monitor learners for when a break from clinical care is needed. Both IM residents and visiting fellows are often steered toward patients they may see in clinical practice (a critical care fellow may see more intensive care patients) and will begin assuming responsibility for patients earlier than more novice learners but always at the discretion of PC faculty.
The learners are graded based on modified assessment tools used in their home program. We have worked with each home program to adjust and modify their assessment tools to most accurately reflect their time on the PC rotation. Written feedback is also solicited from all the faculty and IDT members who have worked with the learner, and these comments are added to the summative and formative evaluation space that is present on learner evaluation forms.
Faculty Development to Improve Teaching Skills
Faculty development sessions are regularly scheduled to review, discuss, and practice teaching techniques. These 1-hour sessions are held quarterly. Educators outside of the PC specialty are invited to give sessions on best practices within the field of education to improve and expand the educational skills of the faculty. Emphasis is given to milestone-based assessment, teaching communication at the bedside, and giving learners feedback on clinical performance.
Milestone-based assessment
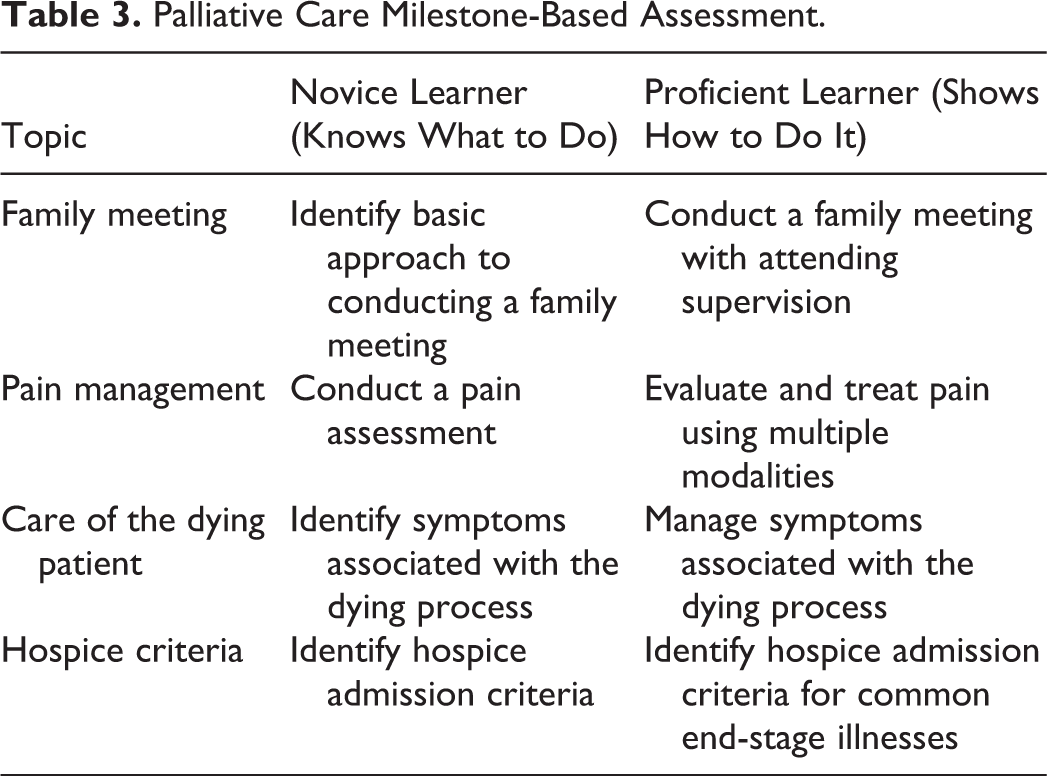
Medical education has shifted from an assumption of competency after time spent with a medical specialty to a delineation of core competencies that a learner is expected to achieve within a medical specialty. We have used the Hospice and Palliative Care Competencies of the American Academy of Hospice and Palliative Medicine (version 2.3, September 2009), Clinical Practice Guidelines for Quality Palliative Care (2013), Hospice and Palliative Medicine Entrustable Professional Activities (2015), and Hospice and Palliative Medicine Curricular Milestones (Draft 2017), and available consensus data 7 to create a milestone-based assessment tool of 4 common PC topics (Table 3). This evaluation tool reflects elements from Miller’s triangle 8 (Figure 1) and encourages learners and faculty to view learning as a predictable process of first obtaining knowledge then applying it. We continue to develop this evaluation tool by adding more detail to the current topics and expanding the list of PC topics. Currently, we use a milestone-based assessment as a self-assessment tool for the learners who have completed their rotation and are working on a way to combine our current self-assessment questionnaire with a milestone-based assessment. We anticipate that a milestone-based PC assessment will be an invaluable tool for both PC learners and faculty to use as a roadmap to improve PC knowledge and skills that can be used across different sites of training.
Palliative Care Milestone-Based Assessment.

Miller’s triangle.
Teaching communication at the bedside
For learners, we review basic communication techniques in the primary PC curriculum such as Ask-Tell-Ask, 9 NURSE empathic statements, 10 and a visual model for goals of care discussions. 11 Learners are encouraged to refer to these tools as they see patients with faculty and on their own. The faculty utilize an educational roadmap described by Back et al 12 that reflects elements from the One-Minute Preceptor 13 and is adapted for teaching communication at the bedside. The faculty first assess the learner’s understanding and brainstorm an approach to the clinical encounter. After observing the patient encounter, the faculty encourage the learner to reflect, give the learner feedback, and encourage identification of a learning point. 12,14
Faculty feedback to learners
Giving feedback is challenging and time intensive in medical education but is critical for obtaining medical competence 15 and is highly valued by learners. 16 We held faculty development sessions to help faculty develop skills in both coaching (assessment and feedback of a single part of a clinical encounter) and evaluation (assessment and feedback of overall learner performance). 17 Coaching-based feedback is a single take-home point after a clinical encounter, while evaluation-based feedback incorporates feedback across numerous encounters and areas of performance. 12,14 Faculty can give quick coaching-based feedback several times per day in between patient encounters. Evaluation-based feedback, which is more comprehensive and time intensive, can occur at designated times throughout a learner’s rotation by individual faculty or by a designated faculty member who compiles feedback across sites. Learners report getting helpful feedback from faculty, and faculty has given informal feedback that the development sessions have helped their bedside teaching. We are looking into ways to measure the impact of faculty development sessions on learner educational experiences, perhaps by adding questions specific to coaching-based feedback and evaluation-based feedback to the posttest assessment survey. Currently, faculty give informal feedback on the educational system and faculty feedback sessions during faculty meetings.
Learner Self-Evaluation
Assessment and improvement in self-efficacy is critical to translate knowledge and skills into behavioral change. 18 Before and after the rotation, learners complete an electronic survey (RedCap) adapted from the Medical College of Wisconsin Palliative Care Program. They self-assess their competence on PC topics with a 4-point scale (1—needs further instruction, 2—needs close supervision, 3—needs minimal supervision, and 4—can perform independently). Topics include conducting a family conference, breaking bad news, discussing do-not-resuscitate orders, discussing home hospice, discussing shift in treatment to comfort care, discussing treatment withdrawal, performing a basic pain assessment, using oral and parenteral opioids, using adjuvant analgesics, assessing and managing difficult symptoms (terminal delirium, terminal dyspnea, constipation, nausea, and vomiting), discussing advance directives, and assessing decision-making capacity. Learners also report their comfort level with seriously ill and dying patients on a scale of 0 to 10 points, with 0 being poor and 10 being excellent.
As a part of the prerotation survey, learners are asked to write their objectives for the time on PC rotation. As a part of the postrotation survey, they are asked to give feedback on the educational system, content, and overall experience during their PC rotation, information that is invaluable as we adjust and improve the PC experience for future learners.
Results
We report here data collected from all the MS and IM residents who rotated with the PC team between 2012 and 2017. All learners complete the surveys, and data from visiting fellows, residents, and nurse practitioner students reflect the trends reported with MS and IM residents but are not reported here due to lower participant numbers. Before participating in the rotation, second-year MS (n = 14) felt that they needed further instruction on PC topics (1.2 [confidence interval [CI]: 1.1-1.2]), and by the end of the rotation, they felt that they were competent to address PC topics with close supervision (2.1 [CI: 1.9-2.3]; P < .001; Figure 2). Third- and fourth-year MS (n = 46) felt that they needed further instruction on PC topics before the rotation (1.4 [CI: 1.2-1.7]) and felt competent to address the PC topics with minimal supervision after the rotation (2.9 [CI: 2.6-3.2]; P < .001).
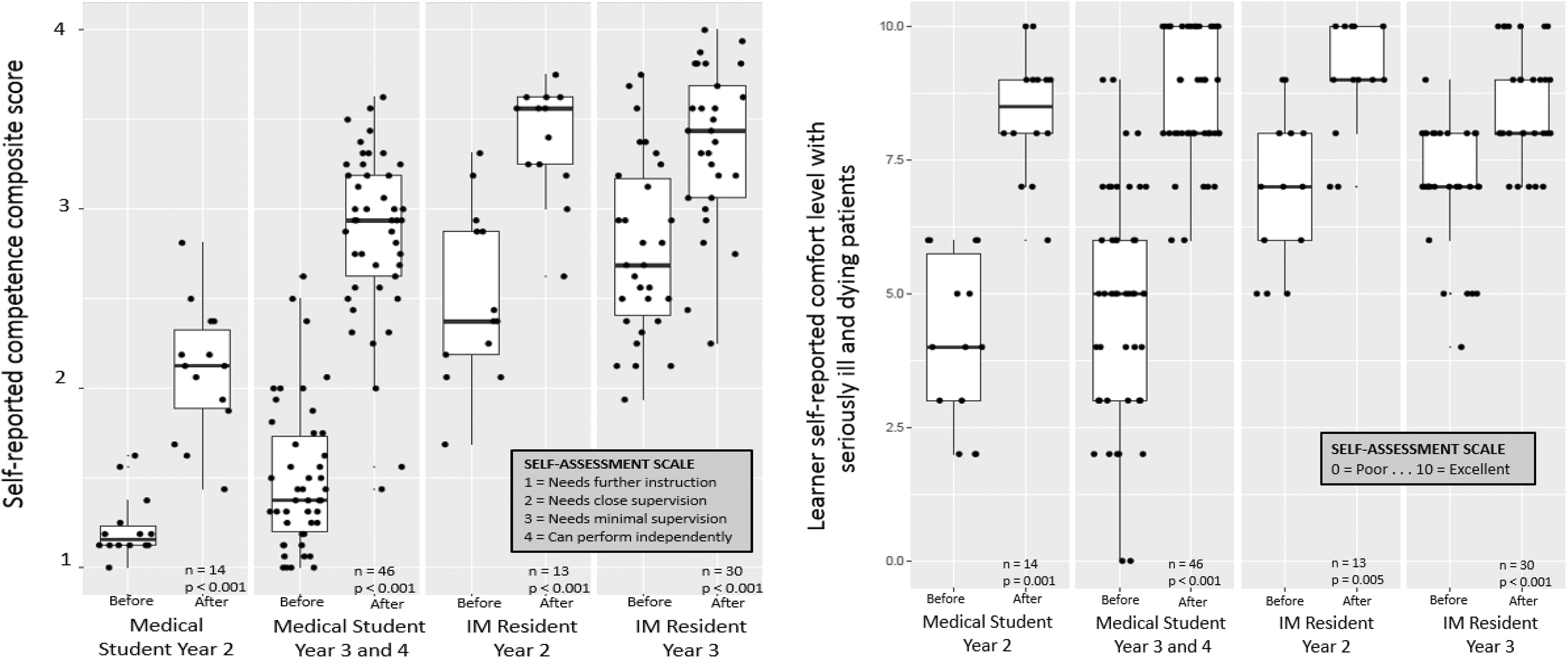
Medical student and internal medicine residents report improved competence with palliative care (PC) topics and improved comfort level with seriously ill patients after elective PC rotation.
Before the rotation, second-year IM residents (n = 13) felt that they needed close to minimal supervision for PC topics (2.4 [CI: 2.2-2.9]), then felt they were competent to address these topics with minimal or no supervision after the rotation (3.6 [CI: 3.3-3.6]; P < .001). Third-year IM residents (n = 30) initially felt that they needed close to minimal supervision (2.7 [CI: 2.4-3.2]), then felt that they needed minimal or no supervision to address these PC topics after completing the rotation (3.4 [CI: 3.1-3.7]; P < .001].
Second-year MS self-reported comfort level with seriously ill and dying patients increased from 4 (CI: 3-5.6) to 8.5 (CI: 8-9; n = 14, P < .001) after the elective rotation. Third- and fourth-year MS self-reported comfort level with seriously ill and dying patients increased from 5 (CI: 3-6) to 8 (CI: 8-10; n = 46, P < .001) after the elective rotation. Second-year residents’ self-reported comfort level with seriously ill and dying patients increased from 7 (CI: 6-8) to 9 (CI: 9-10; n = 13, P < .001) after the elective rotation. Third-year residents’ self-reported comfort level with seriously ill and dying patients increased from 7 (CI: 7-8) to 9 (CI: 8-9; n = 30, P < .001) after the elective rotation.
There are several limitations of the results reported here. One limitation of this survey is that it assesses the self-efficacy and comfort level of the learners but does not assess learner knowledge, learner behavior, patient perceptions of care provided, or direct impact on patient outcomes. It is important to note that the implementation of our educational system and the learner self-assessment occurred at the same time; we do not have comparable assessments of the learner experience prior to the implementation of the educational system. Learners completed self-assessment directly after completion of the PC rotation, and we do not know whether they retain the improvement in self-efficacy after completion of the rotation. Although the feedback from learner surveys has reflected learner gratitude for the one-on-one time and debriefing sessions, it is unclear whether they need further support after the rotation ends. The PC rotation is an elective for both MS and IM residents, so may reflect improvement in self-efficacy for learners who are primed to improve their PC knowledge and skills.
Discussion
By creating an educational structure that emphasizes management of learner schedules, organization of teaching activities, faculty development, and learner self-evaluation, both MS and IM residents improve in self-efficacy with PC topics and comfort level with seriously ill and dying patients. We give examples of how to create a learner schedule that allows the learner to rotate across different sites while keeping learner to faculty ratios low.
To our knowledge, this is the first time that a primary PC curriculum has been described both in content and in implementation. By creating space for both primary and specialty PC didactics within the schedule, we can meet the educational needs of visiting learners, PC fellows, and PC faculty. The feedback from the faculty regarding the broader educational system and faculty development sessions has been positive, allowing faculty to spend their time with the learners building upon a base of knowledge rather than teaching each learner from scratch.
We believe that there will be ample opportunity to bring primary PC teaching to the greater health-care system over the coming years. One area for future development would be to create a primary PC-specific tool that would combine learner self-assessment, faculty assessment of the learner, and the home program assessment tools. This assessment tool will be able to give an accurate picture of the learner’s primary PC knowledge and skill level as well as provide a roadmap to improve their primary PC skills. Our current educational system has given us the opportunity to craft a primary PC curriculum for learners on a PC elective rotation, and we hope to bring primary PC knowledge and skills to faculty, staff, and learners who have not had the opportunity to work with our team. We currently give didactics throughout the health-care system, and we have begun to look for opportunities to incorporate communication training into these short learning sessions. There will be opportunities to use online modules, simulated patient encounters, and other new and exciting teaching tools to help non-PC clinicians care for people with serious illness.
The need to develop primary PC skills in all clinicians caring for patients with serious illness is a daunting but exciting task. We hope that the tools discussed here will support PC educators with practical and innovative teaching strategies as they work to balance patient care and education of a new generation of PC learners.
Footnotes
Authors’ Note
Sumi Misra is also affilaited with Geriatrics Research Education and Clinical Center, Veterans Affairs, VISN 9.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.