
Abstract
Objectives:
Recent evidence suggests that music therapy, a holistic method of care, potentially is beneficial for symptom management. This quality improvement project aimed to evaluate the effect of music therapy on symptom management and coping skills of patients receiving palliative care and to measure patient satisfaction with the therapy. A secondary aim was to evaluate staff perception of patient outcomes of music therapy services.
Methods:
Palliative care clinicians attended a 30-minute education session on music therapy before the project was initiated. Study participants were patients and their families who were cared for by the inpatient palliative care consulting service at Mayo Clinic (Rochester, Minnesota) from June 1 through December 31, 2016. Patients were eligible if they required ongoing management of pain and anxiety or needed adaptive coping strategies. Patients and families were asked to complete a survey after each music therapy session. Staff were asked to complete a survey after completion of the project.
Results:
Music therapy was provided to 57 patients and 53 family members. Patient surveys indicated a decrease in anxiety and pain. All patients reported that music therapy facilitated stress relief, relaxation, pain relief, spiritual support, emotional support, and a general feeling of wellness. All participants recommended music therapy services for others. Palliative care clinicians reported that music therapy added value as a holistic service.
Conclusions:
In this quality improvement project, music therapy positively affected multiple domains of well-being for patients receiving palliative care.
Introduction
Music therapy is a therapeutic modality designed to address physical and nonphysical symptoms that adversely affect a patient’s quality of life. Patients experience music therapy either through active or receptive participation. During active participation, patients partner with a music therapist to creatively express themselves through music or to develop personalized physical or psychosocial rehabilitation plans. During receptive participation, music therapy may be used for self-reflection and relaxation. 1
Music therapy is an adjuvant therapy for patients receiving medical care. 2 Palliative care is specialized medical care for people living with serious illness, focusing on providing relief from the physical and psychosocial symptoms that affect a patient’s quality of life. 3 Music therapy can improve perceptions of analgesia and anxiety in various clinical settings, and it can enhance quality of life for patients by improving pain and symptom management and providing a means for creative self-expression. 4 Similar findings have been reported for patients of all ages receiving palliative care. 4 –6 Indeed, even a single music therapy session can positively impact perceived pain control. 7 Additionally, the use of rhythmic stimulation in music therapy can aid patients with stroke through the complicated process of regaining gross motor movement and improve effectiveness of gait-training therapy. 8 Music therapy is associated with a discussion of spiritual beliefs in the hospice setting. 9 A combination of active and passive music therapy interventions may improve a patient’s overall sense of well-being, reduce distress, and improve self-rated resilience. 5,6
Patients seen by the palliative care consult service at Mayo Clinic (Rochester, Minnesota) have a wide range of serious illness diagnoses and complex symptom clusters. Prompted by patient requests and the palliative care clinicians’ desire to expand the nonpharmacologic options for addressing symptom management, we undertook a quality improvement project to evaluate patient responses to music therapy with regard to its impact on symptom management and coping skills, as well as on patient satisfaction. A secondary aim was to evaluate staff perception of service implementation, delivery, and patient outcomes of music therapy services.
Methods
This quality improvement project was a 6-month endeavor led by an interdisciplinary group of stakeholders, including a board-certified music therapist and multiple members of the inpatient palliative care consulting service (physicians, administrators, and advance-practice nurses). This quality improvement project was determined to be exempt by the institutional review board of Mayo Clinic and followed the DMAIC (Define, Measure, Analyze, Improve, and Control) quality-improvement process. 10 The reporting of this study is in compliance with the SQUIRE (Standards for Quality Improvement Reporting Excellence) 2.0 guidelines. 11
Study Participants and Referral Process
Participants in this quality improvement project were patients and family members who were seen by the palliative care consulting service at Mayo Clinic (Rochester, Minnesota) from June 1 through December 31, 2016. Patients were eligible if they had ongoing need for the management of pain and anxiety or needed adaptive coping strategies, as assessed by the consulting palliative care clinicians. No specific exclusion criteria were used.
Palliative care clinicians attended a 30-minute education session, led by the music therapist, before this project was initiated. This education session addressed how to identify clinical reasons for referral and how to introduce music therapy services to patients and family members. The music therapist worked closely with the palliative care team throughout the project to address any questions that arose regarding how to best introduce music therapy services. Palliative care clinicians approached patients whom they believed potentially would benefit from music therapy. If the patient and family agreed to a visit with a music therapist, the team then placed a referral. Family members were invited to complete a survey if they were present for the intervention. Referring palliative care clinicians were surveyed after the completion of the project.
Intervention
A board-certified music therapist (C.W.) followed a standard consultative approach based on current practice guidelines for music therapy at Mayo Clinic. She met with patients to provide individualized supportive music therapy interventions.
Sessions focused on enhancing coping skills by incorporating music into the patient’s health-care journey, such as through therapeutic singing, music-assisted relaxation, creative self-expression through music, and supportive counseling through music. Interventions were chosen on the basis of the patient’s immediate needs and always incorporated patient-preferred music.
Survey Instrument, Administration, and Measurement
The music therapist recorded the reason for referral and had the patient rates his or her pain and anxiety before and after each session by using a verbal numeric rating scale (range, 0-10; with 0 being no perceived symptoms and 10 being the worst possible symptom intensity). Patients unable to respond were still provided services, but ratings data were not collected. The music therapist also recorded pertinent details of the patient encounters, including the music therapy interventions and patient preferences.
After each intervention, patients and included family members were asked to complete an anonymous survey, which was developed by the workgroup, to evaluate the patient’s experience. Survey questions included 4-point Likert scales to rate effectiveness of therapy, with an option for open-ended feedback and comments (Supplemental Figure 1). Survey forms were left with patients and families at the conclusion of each intervention and were returned to the workgroup by clinical staff. Family members were instructed to complete a survey based on the patient’s experience of the music therapy session if patients themselves were unable to complete a survey. Upon completion of the 6-month project, an anonymous survey was sent to the palliative medicine physicians and advanced practice clinicians to obtain their feedback on the process and offering of music therapy services (Supplemental Figure 2). The team continues to review patient and staff feedback with individual music therapy interventions to be able to revise the process of providing this service.
Patient clinical data at presentation (eg, symptom scores), reason for referral, and postintervention survey data were entered into a spreadsheet (Excel; Microsoft Corp, Redmond, WA) and de-identified. Descriptive statistics were used for the analysis.
Results
Music therapy was provided to 57 patients and 53 family members. Most patients were female (n = 37 [60%]) and middle-aged (mean age, 53 years; range, 23-98 years). The primary reasons for referral included a constellation of symptoms, anxiety, and coping; additional indications for music therapy included dyspnea, nausea, actively dying, spiritual support, family support or anticipatory grief, cognitive stimulation, psychosocial needs, feelings of despair, and quality of life (Figure 1).
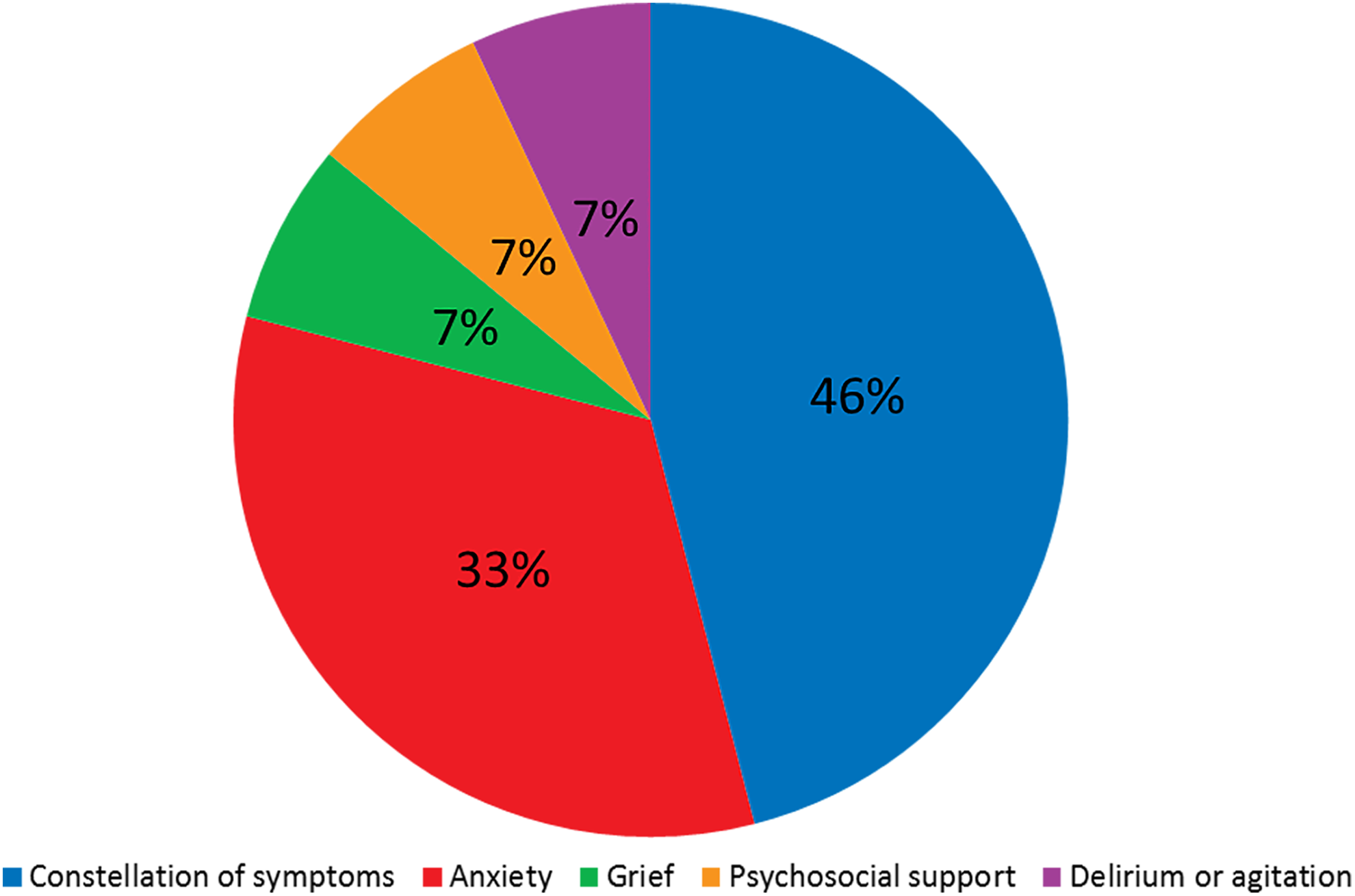
Reasons for physician referral for music therapy.
The average session lasted 32 minutes. Patients were offered various interventions, based on the music therapist’s assessment of patient needs. Interventions included psychosocial support and supportive counseling through music (n = 23), music-assisted relaxation (n = 20), therapeutic singing (n = 8), procedural support (n = 3), local and recorded music resources (n = 5), spiritual support (n = 1), functional rehabilitation (n = 1), reminiscing through music (n = 1), and supportive music imagery (n = 1). Patients were seen 1 or 2 times during their hospitalization. Surveys were given after each visit if patients were seen more than once. Postintervention surveys for 6 patients were not fully completed.
The assessment data indicated that the music therapy intervention decreased the patients’ pain and anxiety (Figure 2). Notably, all patients reported that they found music therapy to be either somewhat or very effective for stress relief, relaxation, pain relief, spiritual support, emotional support, and general feelings of wellness. Specifically, 100% of patients (n = 57) responded positively (“somewhat effective” or “very effective”) to all survey questions. Further, all indicated that they would recommend music therapy services to others (Supplemental Figure 3). Fourteen of the 17 providers who responded to the survey reported that music therapy added value as a holistic service offering to 25% to 100% of their patients (Figure 3). Providers who completed the survey commented that they were surprised that the music therapy interventions provided relief for patients’ physical and emotional distress. One noted, “Even patients who claimed to ‘not like music’ found the music therapy sessions enjoyable.” Twelve providers commented that they (as providers) benefited from having music therapy available as a service or treatment for their patients.
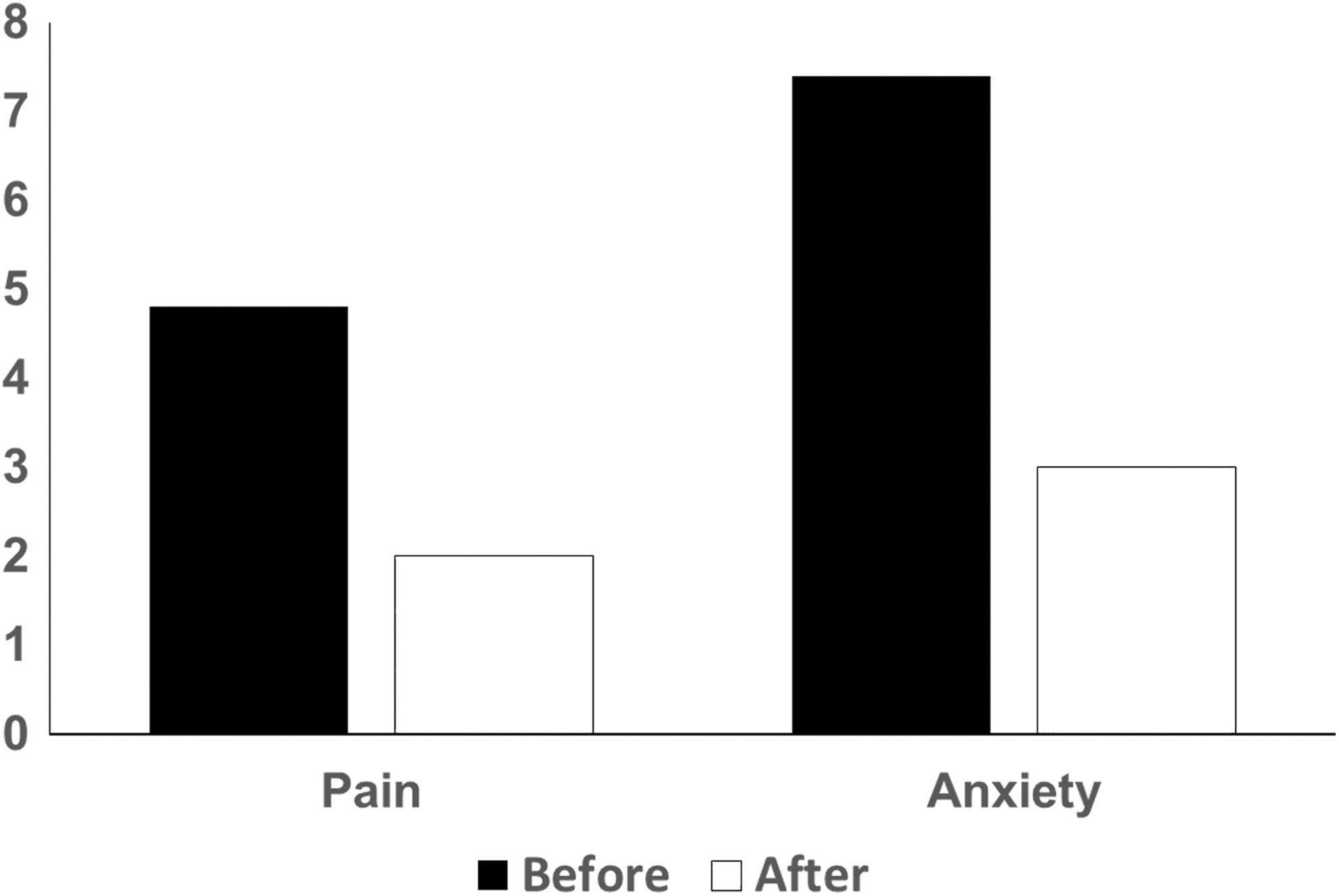
Effect of music therapy on pain and anxiety scores. Patients rated their pain and anxiety before and after the intervention. Possible scores ranged from 0-10, with 0 = best and 10 = worst.
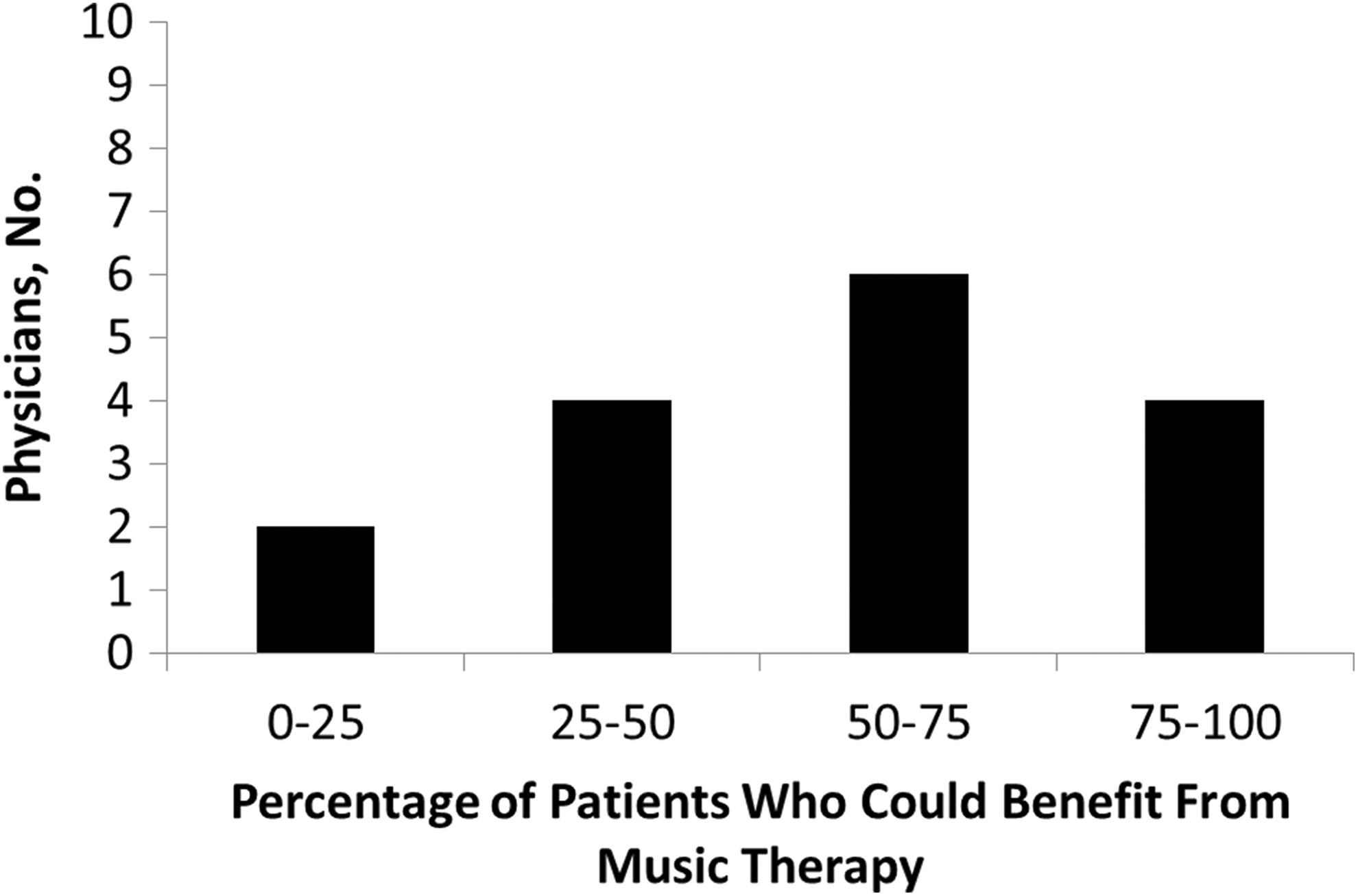
Physician opinion about the percentage of patients who could benefit from music therapy.
Discussion
This quality improvement project evaluated potential patient benefits with targeted music therapy and assessed satisfaction from the referring palliative care clinicians. Patients perceived a decrease in symptom burden after music therapy, indicated that music therapy was effective, and thought they would recommend it to others. Most palliative care physicians also indicated support for a music therapy program.
We learned several lessons throughout this project about patient perceptions and palliative medicine team awareness of music therapy as an offering. Providers mentioned existential distress as a reason for referral, and it would have been beneficial to assess the patient perceptions of existential distress further. Additionally, we did not assess the expectations or effects of music therapy on family member well-being. To provide and maintain awareness of this quality improvement project with the palliative medicine team, we needed to augment the initial education session with regular reminders (eg, e-mails, departmental meetings, and individual conversations) about the availability and benefits of music therapy.
Feedback from the palliative care team was important when reviewing and revising the referral process and to understand the concerns for which music therapy might be most effective. Some providers offered the positive comment that they appreciated having an intervention to suggest to patients, which helped alleviate their frustration from not having another pharmacologic treatment to offer patients experiencing multiple symptoms.
This project aligns with previous literature and research 12,13 regarding the patient-reported outcomes for music therapy. Prior research in music therapy has shown statistically significant improvement in pain, anxiety, depression, shortness of breath, mood, and facial expression 12 and improvement in patient coping and symptom management. 13 Music therapy is gaining acceptance as a fundamental holistic service offering for palliative care programs because it follows the mission of palliative care, which is to provide specialized medical care, focusing on symptom control and improving quality of life, for patients with chronic, life-limiting disease. Music therapy provides additional tools and techniques to manage symptoms and further expands the expertise and services of an interdisciplinary team.
This quality improvement project provides some initial data that palliative care leadership need to continue to garner administrative support to continue offering music therapy as a standard option for patients. It may also encourage development of new ideas for novel complementary and integrative medicine practices that could enhance the patient experience.
Limitations
We acknowledge several limitations to this quality improvement project. This was a small project without a control group. Because of limited funding, the study period was only 6 months; a longer period would have allowed additional provider experience with referrals to music therapy, which would help facilitate its integration as a support service for patients. This quality improvement project took place in a large Midwestern medical center, and the referrals were spread throughout the campus, which limited the time that the music therapist could interact with the staff and providers to improve program visibility and understanding of music therapy interventions. Financial resources to support the clinical time of the board-certified music therapist was provided by donor dollars, and a cost analysis was not completed with this project. However, in the future, patient volume data, clinical outcomes, qualitative comments, and total cost should be examined. Finally, we did not track specific associations between the severity of patient distress and the perceived effectiveness of the intervention.
Conclusion
The initial results of the quality improvement project were strongly positive and provided perceived benefits to patients, families, and palliative care providers. We are pleased to report that, as of manuscript writing, this quality improvement project is in the control phase (final phase of a DMAIC project), with administrative support to continue offering music therapy as a standard option for patients receiving palliative care and their families. We hope that the continuation of music therapy in palliative care will help improve patients’ symptom burden, provide patients and families with additional coping skills, and contribute to an overall improvement in quality of life. Furthermore, hospice programs within the health system have also chosen to implement music therapy services after seeing the benefits of this service for patients in palliative care and their families. It is important to continue exploring additional benefits of music therapy in palliative care on a larger scale.
Supplemental Material
Supplemental_Material - Implementing a Palliative Medicine Music Therapy Program: A Quality Improvement Project
Supplemental_Material for Implementing a Palliative Medicine Music Therapy Program: A Quality Improvement Project by Christina Wood, Susanne M. Cutshall, Rachel M. Wiste, Rachel C. Gentes, Johanna S. Rian, Amie M. Tipton, Dose Ann-Marie, Saswati Mahapatra, Elise C. Carey and Jacob J. Strand in American Journal of Hospice and Palliative Medicine®
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Mayo Clinic Dolores Jean Lavins Center for Humanities in Medicine. The sponsor had no role in the design, implementation, interpretation, or reporting of this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.