
Abstract
Purpose:
This study aimed to determine the impact of advanced care planning (ACP) on potentially avoidable hospital admissions at the end of life (EOL) among a sample of hospice-referred patients with cancer, in order to present actionable considerations for the practicing clinician.
Methods:
This study was designed as a retrospective cohort using electronic health record data that assessed likelihood of hospital admissions in the last 30 days of life for 1185 patients with a primary diagnosis of cancer, referred to hospice between January 1, 2014, and December 31, 2015, at a large academic medical center. Inverse probability treatment weighting based on calculated propensity scores balanced measured covariates between those with and without ACP at baseline. Odds ratios (ORs) were calculated from estimated potential outcome means for the impact of ACP on admissions in the last 30 days of life.
Results:
A verified do-not-resuscitate (DNR) order prior to the last 30 days of life was associated with reduced odds of admission compared to those without a DNR (OR = 0.30; P < .001). An ACP note in the problem list prior to the last 30 days of life was associated with reduced odds of admission compared to those without an ACP note (OR = 0.71, P = .042), and further reduced odds if done 6 months prior to death (OR = 0.35, P < .001).
Conclusions:
This study shows that dedicated ACP documentation is associated with fewer admissions in the last 30 days of life for patients with advanced cancer referred to hospice. Improving ACP processes prior to hospice referral holds promise for reducing EOL admissions.
Keywords
Background
Patients with cancer and caregivers often view hospice admissions as marking the loss of hope of recovery, accompanied by deep grief and a sense of loss. 1 However, prior research has shown that those with terminal illness who died in hospice had better outcomes at the end of life (EOL) such as increased quality of life (QOL), better patient experience, and reduced likelihood of intensive care unit (ICU) admissions and hospital mortality, relative to those who died in an institutional setting. 2 -5 Despite the desire of medical professionals to smooth these transitions to hospice care, they are still fraught with challenges resulting in increased patient and caregiver vulnerability. 6 Although the use of hospice services has measurably increased since the year 2000, ICU use in the last month of life, health-care transitions at the EOL, and live discharges from hospice have also increased over the same time period. 7 -10 Care transitions near the EOL, short hospice stays, and unnecessary hospital admissions are often considered failures of hospice to provide comprehensive comfort care for the patient and family. 11 -14 Often, caregivers and patients are ill-prepared for transition to hospice when they make the decision to forgo curative care 15,16 ; one study revealed that patients and families often lack basic understanding on the concepts of hospice upon the first visit and after referral. 17
The American Society of Clinical Oncology (ASCO) guidelines, as well as others, have emphasized the importance of ongoing fluid advanced care planning (ACP) communications in the course of clinical management of advanced cancer and other progressive, nonremitting chronic diseases in order to improve the patient experience of care and QOL. 18 -22 The effects of advance directives (ADs) such as a Living Will or Health Care Power of Attorney form on quality outcomes have been mixed. 23 -26 The ACP in the form of early conversations has been shown to reduce unnecessary and unwanted medical interventions and improve QOL. 27 Early palliative care, including ACP geared toward caregivers, has also been associated with better caregiver outcomes such as a reduction in depression and stress. 28 Although ADs have not been consistently associated with cost reductions, 29 studies suggest that comprehensive and early ACP as part of palliative care interventions are associated with lower overall costs for the health-care system. 30,31 Based on evidence of improved outcomes with early discussions, the National Hospice and Palliative Care Organization guidelines and ASCO state that ACP conversations should universally occur as part of patient and family preparation for hospice and more generally as preparation for the EOL. 22,32
The impact of ACP on hospice transitions for patients with cancer has not been studied comprehensively; moreover, research on the impact of ACP in the last year of life for patients with cancer is limited. This study examined the relationship of ACP in the last year of life to hospital admissions in the last 30 days of life among a group of hospice-referred patients with cancer. We hypothesized that the likelihood of hospital admissions among hospice-referred patients with cancer would be significantly lower for those who had a prior dedicated ACP documentation in the electronic health record (EHR).
Methods
Study Cohort Selection
This retrospective cohort study was conducted using EHR data to assess the association of ACP in the EHR with admissions in the last 30 days of life among a population of 1185 patients with a diagnosis of cancer referred to hospice between January 1, 2014, and December 31, 2015. A cancer diagnosis was defined using International Classification of Disease Codes, Ninth Revision Clinical Modification codes 140-239, which is consistent with previous studies. 33,34 A custom data set from a Midwestern academic medical center was used to identify all patients with cancer with an ambulatory referral to hospice between January 1, 2014, and December 31, 2015, who died on or before June 30, 2016, to account for a full 6 months (criterion for hospice eligibility) for all patients in the cohort. Patients who survived beyond the measurement period were excluded to remove those who were outliers in terms of expected survival. The EHR data set also contained information on EHR-based ACP documentation. Data for this study were deidentified and obtained through an Honest Broker Protocol and were exempt from institutional review board approval. Stata IC/version 14.2.26 was used for the analysis. 35
Main Outcome Measure
The main outcome measure for this study was admission to the hospital in the last 30 days of life. Aggressive medical care and hospital utilization during this period has been used by other studies to identify quality failures among terminally ill patients. 6,36,37 Date of death was measured throughout the study period and for 6 months beyond; a prognosis of 6 months or less is required for referral to hospice under Medicare payment guidelines. 38
Independent Variables
There were 3 separate treatment measures, each indicating a different form of ACP. The treatment measures included an ACP note in the problem list, a scanned AD, and a verified do not resuscitate (DNR) order. Each of the measures were included in separate analyses to determine the impact of documenting ACP in different ways. These particular measures were chosen based on institutional best practices for the provision of ACP at the health system in which this study took place. While Physician Orders for Life-Sustaining Treatment forms have also been used in some states, not all states and institutions (including this study site) have incorporated them into routine clinical care. 39
For each of these variables, the potential exposure period was 1 year prior to death. To ensure the exposure period occurred prior to the measurement of admissions, a value of “yes” was assigned to the variable of ACP if it occurred prior to the last 30 days of life and within the last year of life. Since an ACP note in the problem list indicates that communication and conversation around EOL planning and ACP had occurred, we measured this variable at 2 different time points (prior to the last 30 days/6 months of life) to determine whether earlier conversations had a stronger association, as has been suggested in the literature. 40
The ACP note in the problem list was analyzed as a binary variable representing whether or not a note was present in the problem list of the EHR during the measurement period. Presence of an AD was defined as a binary variable indicating whether or not a document was present in the medical record at the time of data acquisition. The final measure, verified DNR, was an indicator of whether or not a DNR order was placed in the EHR by the physician after consultation with the patient and/or surrogate and was also measured as having occurred on any encounter in the last year of life prior to the last 30 days of life.
Data Analyses and Covariates
Chi-square test statistics and t tests were performed, as appropriate, to test for differences in baseline characteristics, between treatment and comparison groups. Propensity scores, representing the probability of a subject’s likelihood to be in the treatment group given baseline covariates, were used to reduce selection bias and improve balance between the groups. 41 Based on guidance from related studies, the following covariates were selected: age, race, sex, Charlson comorbidity index (CCI), palliative encounter prior to the measurement period, and education. 14,42 -44 Age was measured as a continuous variable. Race was included as a categorical variable indicating “white,” “black,” or “other.” Sex was modeled as a binary variable indicating male/female. Palliative medicine encounter was a binary variable indicating if the patient had a palliative encounter during the measurement period. The CCI was a continuous variable, with higher score indicating a greater burden of morbidity on the date of hospice referral or 2 years prior. Patient zip code was ascertained from the medical record and linked to Zip Code Tabulation Area (ZCTA), which are areal representations of United States Postal Service Zip codes. 45 The ZCTA-level estimates of education were available in the American Community Survey 5-year estimates, conducted by the US Census Bureau and available at American FactFinder. 46 Education was calculated to indicate a proportion of the ZCTA having some college education or greater. The proportion was recorded into quartiles, resulting in a 4-level ranking representing community education status.
Using logistic regression, inverse probability treatment weights were calculated and applied to generate the average treatment effect and potential outcome means of each form of ACP. 47,48 Stata codes from the study by Garrido et al, including a combination of pscore, psmatch2, and teffects, were used to calculate propensity scores, assess balance, estimate average treatment effects, and estimate potential outcome means. 49 Balance was assessed by exploring the standardized differences between the treated and untreated groups. 49,50 We used a standardized difference threshold of less than 0.25 as a marker of adequate overlap between exposed and unexposed groups on each confounder. 51
Results
Baseline descriptive statistics are displayed in Table 1. For each of the treatment groups, unweighted and weighted statistics as well as standardized differences were calculated to assess balance and are available in Supplement Table 1. The unweighted standardized differences suggest some imbalance in confounding variables such as age, education, race, sex, having a prior palliative encounter, and the CCI. The unweighted patient characteristics for ACP problem list entry prior to the last 30 days of life show that patients with a problem list entry were on average younger, better educated, more likely to have had a palliative encounter, and had a higher average CCI score. Unweighted patient characteristics for those with an ACP problem list entry earlier (6 months before death) were similar to the 30 days before death group except they were more likely to be female and they had a lower average CCI score. Unweighted characteristics for those with a DNR prior to the last 30 days of life show that treated individuals were on average older, better educated, more likely to be black, more likely to be female, more likely to have had a palliative encounter, and had a higher CCI score. Finally, unweighted characteristics for those with an AD show that treated patients were younger, more educated, more likely to be female, more likely to have had a palliative encounter, and had a higher CCI score.
Patient Characteristics.
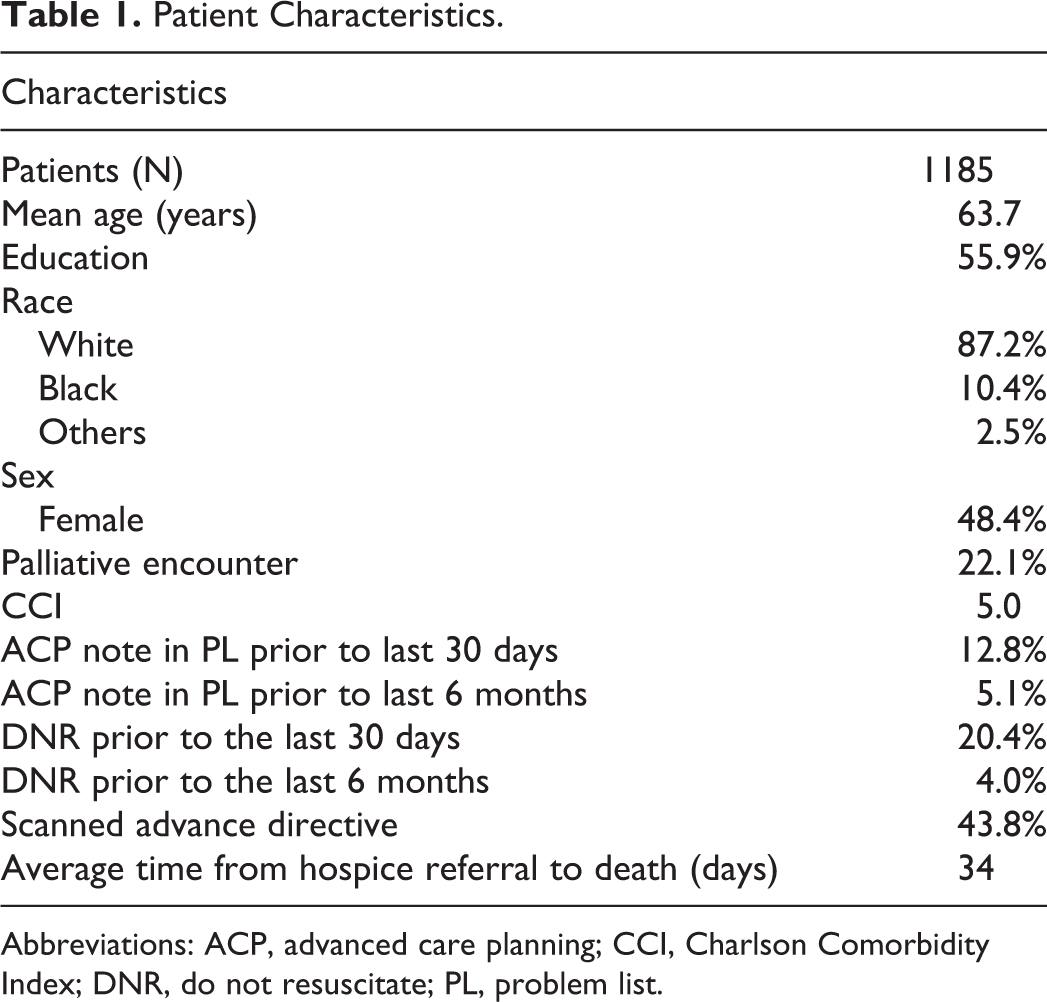
Abbreviations: ACP, advanced care planning; CCI, Charlson Comorbidity Index; DNR, do not resuscitate; PL, problem list.
Table 2 shows the odds ratios (ORs) for admissions in the last 30 days of life, based on whether or not the patient had each form of ACP. For the first treatment, a verified DNR prior to the last 30 days of life, odds of having an admission in the last 30 days of life were significantly less than the odds of those without a DNR (OR = 0.30, 95% confidence interval [CI]: 0.21-0.41; P < .001). The odds of admission in the last 30 days of life for those with an ACP note in the problem list were significantly less than without an ACP note if done 30 days prior to death (OR = 0.71, 95% CI: 0.51-0.88; P = .042) and were even less if done 6 months prior to death (OR = 0.35; 95% CI: 0.22-0.55, P < .001). Having a scanned AD was not significantly associated with reduced odds of admission in the last 30 days of life.
Weighted Odds of Admission in the Last 30 days of Life and ACP Treatments.
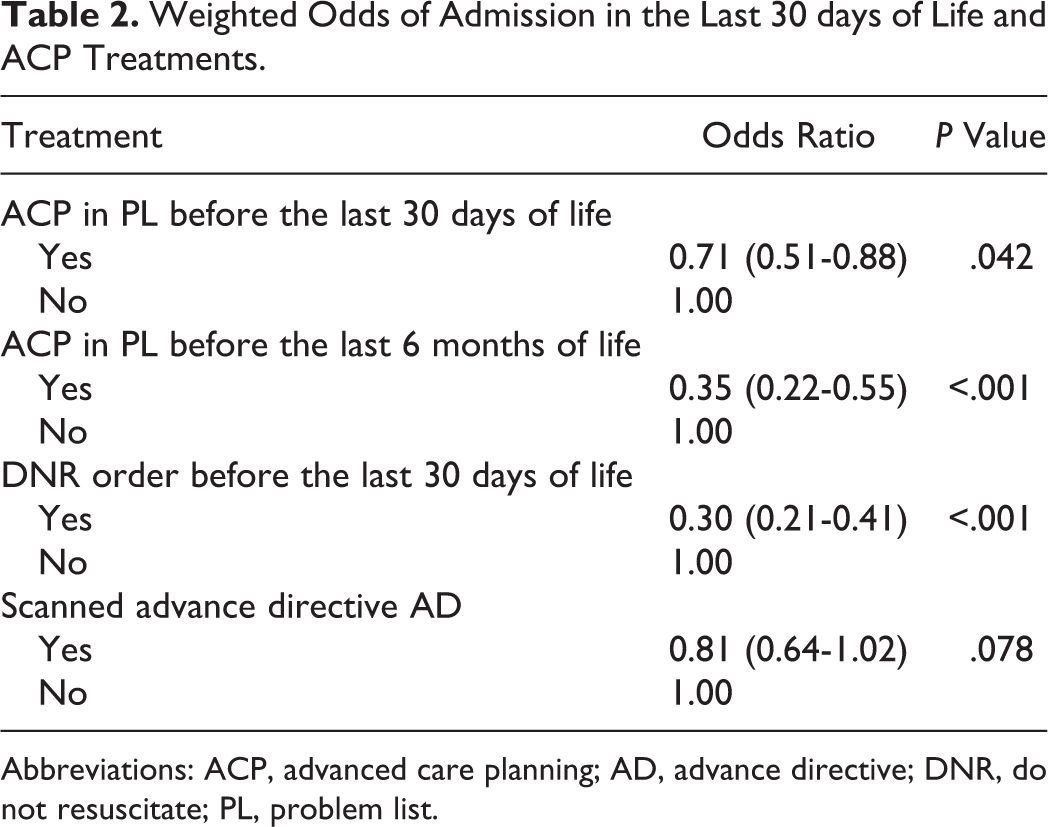
Abbreviations: ACP, advanced care planning; AD, advance directive; DNR, do not resuscitate; PL, problem list.
Discussion
Ensuring patients and caregivers are adequately prepared for transitions to hospice in the form of comprehensive ACP has potential to improve outcomes at the EOL. Our primary finding was that in the last year of life, the presence of an ACP note in the problem list of the EHR was associated with a reduced odds of admission in the last 30 days of life when it was completed on any encounter prior to 30 days before death, and even more so on any encounter prior to 6 months before death. Additionally, having a DNR order verified in the EHR 30 days before death significantly reduced the odds of admission in the last 30 days of life. This finding is in contrast to another study by Goldenheim et al, which assessed DNRs and found no significant difference in 30-day hospital readmissions in a sample of seriously ill patients. 38 The conflicting results could have been due to that study’s very limited sample size and the fact that the DNR was noted on index admission, which was on average only 8 days prior to readmission, a critical difference in study design because we intentionally studied ACP events occurring prior to the last 30 days of life.
Our finding that an ACP note in the problem list (indicating that an EOL conversation occurred with the patient) had a stronger association when done prior to 6 months before death as compared to just 30 days before death supports the idea that earlier ACP conversations and documentation may have been more beneficial for improving outcomes at the EOL. Having an AD had no relationship to admissions in the last 30 days of life, which is consistent with other studies demonstrating that ADs show little promise for improving outcomes. 52 -54 Our results also indicate that having a palliative encounter 30 days or more before death lowered the odds of being admitted in the last 30 days of life, which is consistent with studies showing that early palliative care can lead to less aggressive medical care near the EOL. 55
The mechanism through which ACP leads to improved outcomes may be limited to the elements of care that require some form of a discussion, as opposed to simply uploading a lengthy document such as a living will. This finding, and other critiques of ADs, support the movement away from the Patient Self Determination Act–emphasized methods of ACP, such as legal documents, and toward methods such as an early conversation with a care provider, which may result in a documented, verified DNR. 52,53 Many studies have concluded that the integration of early ACP is critical to providing effective communication at the EOL, particularly for those with a chronic illness. 56 -58 Our results extend the findings from earlier studies to show a reduction in hospital admissions associated with ACP among patients with advanced cancer referred to hospice.
Improving transitions to hospice for patients with advanced cancer will most likely require a multidimensional approach. Our study indicates that EHR-documented ACP is associated with reduced odds of admission in the last 30 days of life. Prior studies have shown that only 13% to 44% of terminally ill patients have documentation of ACP in the EHR 59 and that it is often inconsistent in location. 60 Consistency in documentation location and retrievability of pertinent information relevant to care coordination across settings of care continues to be a major concern among providers. 61 Documentation of ACP could potentially be improved by either aligning organizational/provider incentives or allowing patients to upload ACP preferences from patient portals, which has been shown to improve the quality of ACP documentation in the EHR. 62,63 For those that do have EHR-documented ACP, ensuring that this information is exchanged with the hospice is essential, and smoothing care transitions may depend on it. This would require a more aggressive push toward interoperability, which is already a challenge given lower than average, although increasing, rates of EHR adoption within hospice and home health organizations. 64,65
The second potential area for improvement is to ensure that communication around hospice and goals of care is occurring prior to referral. Patients with cancer often face a long illness trajectory with very slight decline over a period of years, followed by steep decline over the course of a few months. 66 Cancer trajectories lend themselves well to palliative care and discussions on goals of care, but too often providers and patients follow more compartmentalized care, reluctant to discuss palliative care until all curative approaches have been exhausted. Even when receiving palliative care early, discussion on ACP and treatment decisions often occur late in oncology settings, although they are consistently associated with better quality EOL care. 67 Recent clinical movements have promoted pursuing concomitant palliative/curative measures, but such movements should do more to incorporate ongoing, routine conversations about ACP. 55,68
Furthermore, although many nonpalliative providers may worry about damage from an early discussion of prognosis, there is evidence showing that it strengthens the patient–provider relationship. 69 An even better approach would be one which considers both palliative and curative approaches early after diagnosis, with ongoing conversations regarding ACP and continued discussion and updating of the care plan reflecting changing views and preferences as death becomes imminent. 70 To assist in communication, empathy-building training interventions have shown promise toward helping health-care providers respond more effectively to a patient’s emotions and have shown an increase in trust in the provider from the perspective of the patient. 71 There is a gap in the literature on best practices for implementation and evaluation of caregiver communication programs, and more attention and research is needed in this area. 72
There are several limitations to this study. First, the study only assessed the impact of ACP on outcomes in the last year of life, using referral to hospice as the inclusion criterion, with limited information on whether or not the patient followed through on the hospice referral or the quality of the hospice to which they were referred. There is substantial variation in hospice ownership structure as well as performance on quality metrics, which could impact the likelihood of readmission. 73,74 Second, the study was conducted at a large academic medical center; therefore, the generalizability of the results may be limited. An additional threat to generalizability is our focus on patients with cancer who were referred to hospice, a sample which may not be a representative of all patients with cancer nearing the EOL. Finally, we were unable to mine individual encounter notes for ACP; however, institutional policies outlined for ACP to be documented in the problem list when discussed, for enhanced retreivability and visibility.
While increasing palliative medicine workforce and improving EOL communication skills for all physicians might be the ideal solution for improving outcomes at the EOL, a change of this magnitude would require significant resources. A potentially promising implication from the results of this study is that a coordinated and organized intervention targeting consistent EHR-based ACP documentation may be a relatively low-cost and high-impact alternative for improving outcomes for the patient with advanced cancer at the EOL. The development of interventions centering on ACP documentation, while considering the literature on influencing provider behavior, is a logical next step for improving outcomes at the EOL.
Supplemental Material
Supplemental_material - The Impact of Advance Care Planning on End-of-Life Care: Do the Type and Timing Make a Difference for Patients With Advanced Cancer Referred to Hospice?
Supplemental_material for The Impact of Advance Care Planning on End-of-Life Care: Do the Type and Timing Make a Difference for Patients With Advanced Cancer Referred to Hospice? by Laura C. Prater, Thomas Wickizer, Julie K. Bower and Seuli Bose-Brill in American Journal of Hospice and Palliative Medicine®
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.