
Abstract
Objectives:
Although the experiences of family members who care for relatives at the end of life have been researched extensively, little is known about the needs and experiences of families caring for hospice patients with pacemakers.
Aim:
To better understand the experiences of family caregivers of a terminally ill patient who received hospice care at home and chose deactivation of a pacemaker.
Design:
The exploratory, cross-sectional design involved semistructured, in-depth interviews. A narrative analysis focusing on form and content was chosen to analyze the data.
Participants:
Five bereaved caregivers from the Midwestern United States who provided care and participated in the deactivation of their family member’s pacemaker.
Results:
Four storylines that described, gave meaning to, and contextualized the caregivers’ experiences were identified: “I am done. I am not doing it anymore”; “Whatever you decide, I’ll support you”; “It is really difficult to watch, but you want to be there”; and “I will not have part of this.” Caregivers struggled with lack of support, understanding, and acceptance from medical providers when their family member decided to have her pacemaker deactivated, and they believed that the hospice model of care was appropriate to support and help them in that process.
Conclusions:
This research aids in understanding the ramifications of family-provided end-of-life care to a patient whose pacemaker has been deactivated. This can help to increase hospice clinicians’ knowledge regarding caregivers’ experiences facing deactivation of a pacemaker, before and after the patient’s death.
Introduction
In the past 20 years, a number of studies have explored the experiences of deactivation of implantable cardioverter-defibrillators (ICDs) at the end of life (EOL). 1 -3 However, contemporary research suggests that additional exploration is needed regarding patients with cardiovascular implantable electronic devices who are near the EOL. 1 Many prior studies have focused either on the ethical aspects of deactivating ICDs or the experiences of patients and the clinicians involved in their care, but little about the same procedure with pacemakers has been published. 4 Experts suggest that the psychological distress experienced by patients with such devices, as well as by their families, might be underappreciated, 5 and this area warrants additional investigation by specifically exploring the caregiver experience.
Pacemakers are not life-support devices and will not resuscitate a patient, but clinicians agree that pacemakers are subject to the same ethical standards as other medical treatments. 6 Although device deactivation is legally and ethically acceptable when requested by the patients themselves or by their primary caregivers (when patients lack decision-making capacity), 7 caregivers have difficulties coping with and discussing the use and deactivation of implantable cardiac devices. 1 Understanding the caregivers’ perspectives, needs, and experiences is as important as understanding those of the patients themselves because pacemaker deactivation typically is a family-based decision. Family members caring for a terminally ill relative with a pacemaker face severe challenges, including stress, guilt, depression, hopelessness, lack of family support, and changes in family roles, 8 in addition to the numerous challenges associated with caring for a dying patient. 9,10
Considerable gaps remain in understanding the experiences of those who care for a dying relative with a pacemaker. The caregiver experience is of great importance as it helps interdisciplinary team members, who often struggle with such a procedure, to recognize and provide appropriate hospice care. 11 The aim of this research was to better understand the experiences of family caregivers of a terminally ill person who was receiving hospice care at home and underwent deactivation of a pacemaker.
Methods
Study Design and Participants
This research used a qualitative, exploratory, cross sectional study design to explore caregivers’ experiences about caring for a patient with a pacemaker receiving hospice care at home and about deactivation of such a device. A purposive sampling of bereaved primary caregivers who received support from the hospice program associated with a large, not-for profit health system in the Midwestern United States participated in the study. Ethics approval was granted by the organization’s institutional review board. Verbal consent was obtained.
Data Collection
In-depth, semistructured, open-ended interviews were used as a data collection method to elicit chronologic narrative accounts of the experiences of family members caring for a dying patient with a pacemaker and their experience arising from participation in the process of deactivation. They were conducted and digitally recorded from January through May 2018, in a location of the participants’ choosing.
Data Analysis
Interviews were analyzed by using a narrative approach based on narrative research pedagogy 12 -14 and aided by the “River Allegory.” 13 Analysis quality was safeguarded by the criteria for establishing transferability, credibility, dependability, and confirmability. 15,16
Results
Five family members (daughters), each of whom provided unpaid care to their terminally ill mother, were interviewed. The patient received hospice care at home for 19 days and died shortly after deactivation of her pacemaker (<24 hours). All caregivers were white women, aged 50 to 72 years, and all were thought to have a low risk of complicated grief. The family was recruited to participate in the study 6 months after their mother’s death.
Four major storylines were identified that reflected the experiences of caregivers caring for a family member whose pacemaker was deactivated while receiving support from a home-hospice team. The identified stories were interwoven to form a narrative about caregivers struggling with the process of having their mother’s pacemaker deactivated and detailing their experiences, challenges, needs, and family dynamics during the process.
Patient’s Story: “I am Done. I am Not Doing It Anymore.”
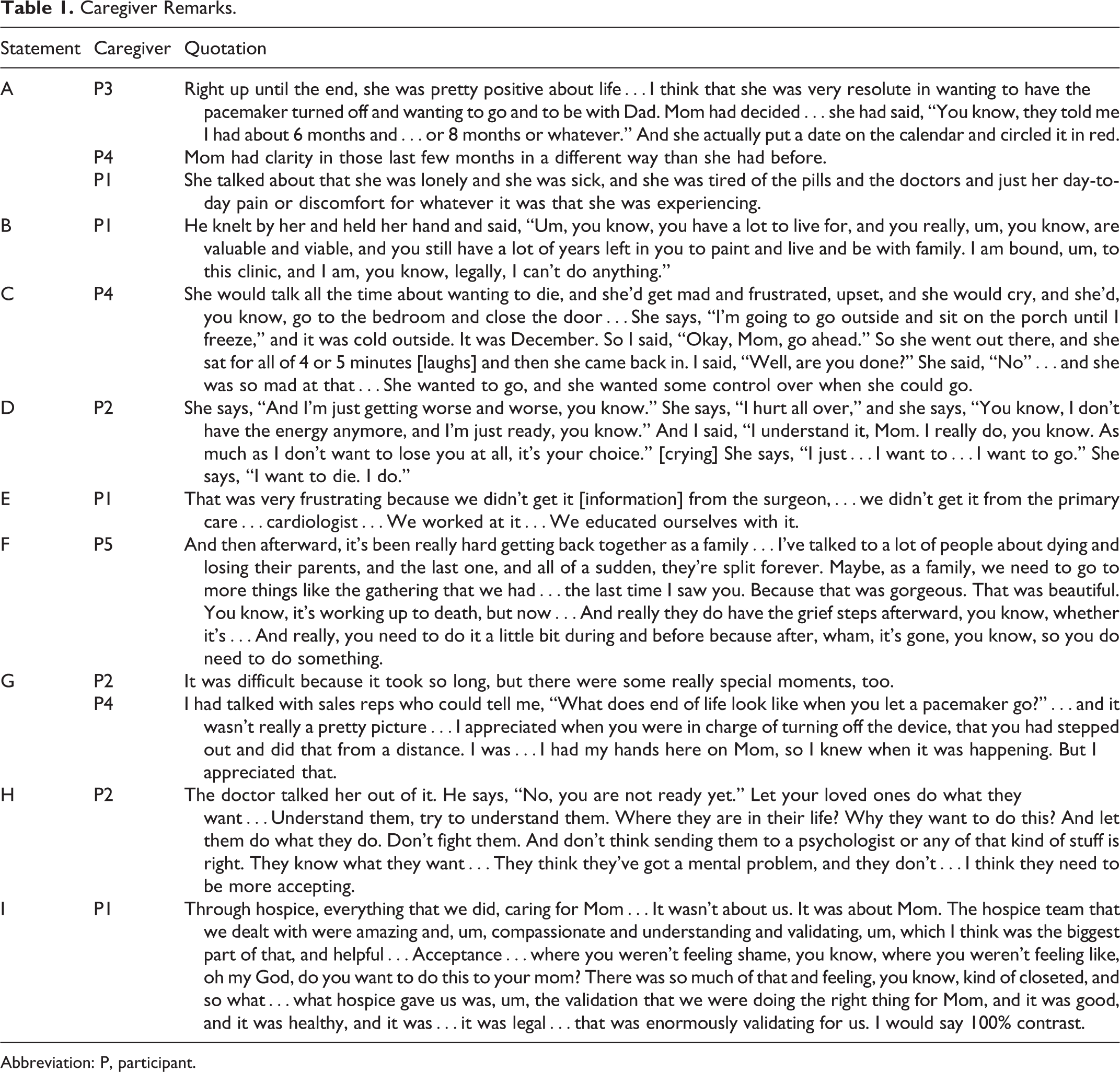
Mary (pseudonym) was a 90-year-old woman, terminally ill, with the primary diagnosis of complete atrioventricular block. Although she had dementia, her caregivers described her last months of life as being marked by an awareness of her diagnosis and wanting to be in charge of the decision to deactivate her pacemaker. Her caregivers said she understood the consequences associated with its deactivation. Participants (P) P3 and P4 described that awareness and Mary’s cognitive abilities for her decision-making (Table 1, statement A). Mary’s desire to deactivate the pacemaker was the result of her declining health and challenges of living with a terminal disease (Table 1, statement A, P1).
Caregiver Remarks.
Abbreviation: P, participant.
Constant health challenges, physical decline, losing control, and desire to be in charge coincided with her desire to be reunited with her beloved deceased husband. Mary believed that in death, she could rejoin her husband, and so Mary had her family organize a “wake awake,” a party that served as her farewell and as a celebration of her reunion with her husband. It also was a celebration of her decision to not implant another pacemaker, which would only prolong her life.
Subsequently, Mary’s medical care team persuaded her to consent to replacing her pacemaker, even though she had a clear awareness of the consequences of not replacing the device. The caregivers’ stories indicated that health professionals appeared to disregard her wishes and signs of declining quality of life. Participant 1 described one such conversation that Mary had with her doctor (Table 1, statement B).
The new pacemaker did not result in viable time; rather, it caused greater frustration, disappointment, and additional burdens. Participant 4 recalled how Mary expressed suicidal thoughts after her pacemaker was replaced (Table 1, statement C). Mary’s experience of living with a pacemaker, despite her desire to die, dominated her last few months until she learned that device deactivation was an option.
Caregivers’ Story: “Whatever You Decide, I’ll Support You”
The caregivers’ story is about the family’s acceptance of her decision, their frustration with medical systems, their needs, and the conflicts that arose from family dynamics and lack of communication. Despite their pain about losing their loved one, the family recognized Mary’s struggles and needs; thus, they consistently respected her wishes and supported her decision to deactivate her pacemaker (Table 1, statement D). This acceptance later simplified their own grieving process. Their story emphasized a considerable struggle with the lack of understanding and support from medical professionals, who showed great enthusiasm for inserting a pacemaker but great reluctance when considering its deactivation. Without the support and understanding of the medical team, the caregivers felt lost and helpless, and they were forced to navigate alone through a difficult health-care situation (Table 1, statement E).
The caregivers’ story also highlighted the needs that arose during the process of caring for a person who wanted to deactivate her pacemaker. Their most urgent need was to have the medical personnel accept the patient’s wishes and support the caregivers’ decision to support their loved one. The caregivers also wanted support from the medical personnel as they worked through ethical concerns and would have appreciated their help in coordinating communication in the setting of difficult family dynamics. Another important and revealing need in the caregivers’ story was the need for support after their mother’s death (Table 1, statement F). This nuanced cry for help from P5 expressed the caregivers’ need to be cared for after the death of a loved one in the same way that they were cared for before the death. Caregivers felt that the support from the hospice staff suddenly ceased after the death, and they lacked guidance in their grief, which can be complicated when death results from the physical process of turning off of a mechanical device.
Pacemaker’s Story: “It Is Really Difficult to Watch and be There, But You Want to be There”
The caregivers clearly had challenges in caring for a patient who wished to deactivate her pacemaker, especially regarding the process of actually deactivating the device. The caregiver stories described their need to be prepared for such an event. They had received information and support when the device was implanted, but they reported a lack of information and support about the deactivation process. Caregivers were forced to educate themselves about the differences between various implanted mechanical devices. They were not able to find or receive informational pamphlets or flyers about device deactivation and had to rely on Internet sources for ethical views and the practical aspects of the process itself. They wanted help in discussing the process with their mother to reassure and confirm that what she wanted was not biased by their own opinions. It was crucial for them to meet with the hospice interdisciplinary group (IDG) members, including the medical director, a registered nurse, a social worker, and a chaplain, to be educated about the process of deactivation and to communicate it to Mary herself.
Although the process of deactivating the pacemaker was emotionally charged, difficult to witness, and did not result in the immediate death of the patient, the caregivers recognized their own need to be there, as well as their need to understand how the process would be performed. They appreciated that the mechanical device used in the deactivation process was not present in the patient’s room, and they expressed gratitude about being told about what might occur and how the hospice team members would support them. Participants 2 and 4 described how they felt as the deactivation was performed and after it was completed (Table 1, statement G). Despite the difficult experience, the caregivers recognized that the support from the hospice team members and their presence during the event was meaningful and indispensable.
Health Care and Support Professionals’ Story: “I Will Not Have Part of This”
Mary’s family caregivers described a marked lack of support from the medical and professional community when assessing the process of pacemaker deactivation. That lack of information added to their emotional pain, and the lack of acceptance and understanding left them believing that they were on their own. The caregivers’ decision to support the patient’s decision contributed considerably to their difficulties. None of the professionals (eg, from the lawyers drafting the will to the doctors) acted in accord with the patient’s wishes. At times, the conflicts were based on differing ethical convictions or institutional regulations, and at other times, they were due to the professional’s minimal understanding of the patient’s and the caregivers’ needs (Table 1, statement H). Caregivers wanted to have their needs recognized and met, even if they were inconsistent with the medical professionals’ desire to save and prolong life.
The caregivers expressed that understanding, support, and acceptance were provided only when their mother entered a hospice program and the hospice IDG became involved in her care (Table 1, statement I). Family caregivers recognized that the support from different members of the IDG helped them with distinctive needs: medical, emotional, legal, and spiritual.
Discussion
The experiences of individuals caring for a hospice patient who has chosen to have her pacemaker deactivated reveal a story of caregiving in an uncommon context. These interviews underscore the importance of respecting the decisions of patients with pacemakers at the EOL. Although some patients might not be able to make a conscientious decision in such an important matter, this study showed that even if the patient’s reasoning skills might be affected by illness, just the sense of being in control and having a meaningful existence might improve quality of life and enhance coping. Antonovsky’s theoretical formulation of the sense of coherence 17 is helpful for understanding behaviors that change previously challenging behaviors into positive ones and ultimately result in better family dynamics.
Families facing the death of a loved one already have major difficulties and burdens. 9,18,19 Caring for a patient who decides to deactivate a pacemaker and hasten death adds to those burdens and requires additional support, understanding, and acceptance of such decisions. Lack of such support and understanding on the part of the medical community might decrease the caregivers’ confidence about caring for a dying person at home 20 and create additional burdens. When a patient’s wishes are not respected, the caregivers’ response is to blame the health-care system for the lack of compassion and support, and it affirms the stereotype that medical care is focused primarily on saving or prolonging lives, regardless of the patient’s personal wishes and goals. The need for information is crucial. 21 -23 Caregivers need to have easy access to information so that they can understand the process and feel supported, even if the medical provider is objecting to the decision. Theories related to caregiving 24,25 strongly suggest that practical and emotional needs must be satisfied in such a difficult context of caregiving.
It is extremely important that health-care systems recognize the benefits of allowing caregivers and patients to make their own decisions regarding device deactivation, even if it hastens death. Their autonomy is preferable to medical professionals and institutions projecting their own convictions and regulations. The hospice model of comprehensive and whole-person care seems to recognize caregiver and patient needs best, 26 and hospice care should be offered immediately when a terminal illness is diagnosed.
This research offers additional perspectives regarding the technical process of pacemaker deactivation. Involvement of the entire IDG, with each member providing support according to his or her role, is indispensable to the process. Spiritual support from the hospice chaplain also was crucial in this case, even though the family and patient held varied religious beliefs; their experience emphasizes the importance of involvement by the entire IDG. The family must be made aware of the steps that will be taken and the physical signs of the process so that they are prepared for possible complications of discomfort. Similarly, the environment where the process takes place must correspond to the patient’s and caregivers’ wishes, to respect their socioemotional meaning of home. 27 The intrusion of devices used in the deactivation must be minimized as much as possible.
The hospice model of care and support in such a process contributes positively to grief. None of the participants of the study experienced complications in their grieving process, even though the patient’s death was influenced by the additional emotional and ethical stressors of deactivating the pacemaker.
The caregivers’ story of supporting their mother’s decision to deactivate her pacemaker included their difficulties, needs, search for help, and finally the acceptance, approval, understanding, and support from hospice services. The hospice model of care appears to be effective for situations in which complex dynamics arise.
Limitations
A limitation of this study is that it presents the experience of only 1 family; thus, caution should be used when generalizing these findings to other caregivers and contexts. However, the nature of narrative analysis is to conduct a detailed exploration of the experiences of individuals or units, which is how we identified nuanced aspects of the caregivers’ story. Furthermore, these details are important to report because little has been published about deactivating a pacemaker in the home care hospice setting.
Conclusion
This study described the experiences of family members who were the primary caregivers of a relative who decided to deactivate her pacemaker. It sheds light on family needs during this EOL circumstance, which can inform hospice clinicians about how they approach providing caregiver support before and after a patient’s death. This study affirms the importance of qualitative research methods, especially narrative analysis, to gain insight into how families experience health care, and we suggest that broader use of these methods might accelerate the health-care improvement process.
Footnotes
Acknowledgment
Authors recognize the work of Margaret Mudroch, MA, and express gratitude for her second-round data analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.