
Abstract
Background:
Facilitating patient conversion to hospice at end of life is a prominent clinical concern. Enrollment in outpatient palliative care services is often assumed to encourage seamless transition to hospice care, but this has not been demonstrated. Moreover, decisions to convert from palliative care to hospice are generally treated as dichotomous, thus hampering our ability to understand decision processes.
Objective:
To examine medical decision-making among patients who are prospectively evaluating whether to convert from palliative care to hospice.
Design:
Qualitative case study, using in-depth interviews and constant comparative method.
Setting/Patients:
Terminally ill patients currently enrolled in outpatient palliative care services (N = 26) and their caregivers (N = 16), selected purposely for maximum variation in condition and personal background.
Measurements:
Themes identified in qualitative in-depth interviews.
Results:
Patients rarely refused hospice outright but more often postponed using a “soft no,” in which they neither accepted nor overtly refused hospice. Justifications patients and caregivers offered for why hospice was not needed (yet) appeared in these themes: (1) not seeing the value added of hospice, (2) assuming the timing is premature, and (3) relying on extensive health-related support networks that justify or endorse continuation of active care.
Conclusions:
Despite assumptions to the contrary, benefits associated with utilization of outpatient palliative care services have the potential to incentivize the delay of hospice in some cases. Clinical interactions with outpatient palliative care patients should consider the influence of these broad social support systems when discussing hospice options.
Keywords
Introduction
Hospice care services, while covered under Medicare and other insurances, are underutilized in the United States. 1,2 To obtain hospice benefits, users must relinquish curative medical treatment. Thus, hospice decisions are typically conceptualized as falling into 2 categories: acceptance or refusal. However, this dichotomous categorization overlooks a fuller spectrum of decision-making activities. As Romo et al 3 suggest, the choice to enroll in hospice is “better seen as a process arising from the interaction of beliefs, attitudes, and behaviors that evolves over time.”(p1) Building on this framework, we use qualitative interview data from one urban outpatient palliative care setting to examine social, contextual, and organizational factors influencing this variation in end-of-life health-care decision-making. Our goal is to further understandings of how hospice decisions unfold over time, consistent with recent calls for studying the complexity involved in end-of-life care. 4 -8
By taking a social science perspective on the topic of hospice decision-making, our approach allows for examination of how health-care systems and individual patients interact, occupying analytic space between traditional psychological and health services approaches. For example, previous work has generated important knowledge regarding psychological and psychiatric perspectives on hospice decisions, including individual characteristics such as death anxiety, 9,10 sense of coherence, 11,12 “middle knowledge” of the uncertain interval between living and dying, 13,14 and phasic models of dying. 15 At the same time, health services research is often focused on utilization patterns 2,16 and the ways in which palliative care and hospice have the potential to provide a seamless continuum of care for those with serious illness and facing end of life. Although studies of inpatient care have demonstrated that consultations with palliative care teams increased the likelihood of patient discharge to hospice, 17,18 comparable results have not been shown for outpatient hospice. Nevertheless, palliative care is often conceived as a service that should facilitate transition to hospice by helping stage a gradual transition from curative to comfort care. 19
In our qualitative interviews with terminally ill patients and their caregivers, however, we find that the presence of palliative care services may have the potential to incentivize the delay of hospice under some circumstances. Below, we examine a phenomenon we term a “soft no,” in which patients neither accept nor overtly refuse hospice. Those giving “soft” refusals do not explicitly refuse hospice, but their actions function to postpone a hospice decision in an uncertain health context that may become more clear over time. 20 In a health policy context wherein concurrent care options are being considered as part of the Medicare Care Choices Model, 21,22 it is critical to understand how palliative care and hospice sectors of health care coexist and shape patient choices. From a clinical perspective, understanding how and why patients resist or embrace hospice conversion is critical; lessons learned from this case study can shed light on this enduring puzzle by providing a deeper understanding of the longitudinal, iterative processes and alternative influences on patients and families—thus extending beyond existing assumptions about providers “recommending” hospice and patients “electing” services. 3
Method
Study Design
Qualitative study using in-depth interviews, reported in accordance with consolidated criteria for reporting qualitative research guidelines. 23
Participants and Setting
Patient participants were sampled purposely from an outpatient palliative care attached to a large urban hospice between May and December 2015. The palliative care team provided telephonic and at-home support from a multidisciplinary team consisting centrally of nurse case managers, a nurse practitioner, a social worker, and a patient navigator, all under the direction of a physician medical director. This team liaised with physicians to provide pain and symptom management for patients, as well as facilitating connections to eligible social services and home aide companies when needed. Frequency of patient contact was varied according to needs, and the service covered a geographic area of an approximately 25 mile radius from the office.
Inclusion criteria were developed in conjunction with clinic providers and aimed to achieve maximum variation by personal background and medical condition. Inclusion criteria included being eligible for hospice, aged 50+, able to consent, and able to participate in an interview in English. All medical conditions were included. Patients who met these criteria were approached by palliative care staff who introduced the study, and authors then followed up to schedule and conduct interviews. Patients were invited to include caregivers at the interview if they desired.
A total of 45 patients agreed to be interviewed, but many became unavailable for a variety of reasons, including primarily deterioration in health (N = 7) or changing their minds for unspecified reasons (N = 9); these are common challenges in palliative care research. 24,25 The final sample (N = 26 patients and 16 caregivers) was mostly female, patients with cancer, married, with some college education, and with an average age of 71.5 at the time of interview (Table 1). One patient aged 41 years was inadvertently screened into the study and the oversight was not detected until the interview was underway; this patient is included in the present analysis. We did not ask patients to self-identify their race/ethnicity. We did collect household income data but do not report it here as we found it to be an unreliable indicator of current socioeconomic status as so many patients had retired or gone on disability by the time of the interview; however, the sample has significant diversity in terms of education and we observed apparent diversity in socioeconomic status and race/ethnicity. We did not collect demographic data from caregivers. Eight palliative care staff working on the service were also interviewed for a separate portion of our study; these interviews, combined with ethnographic observations of interdisciplinary team meetings, provide background information, allowing us to contextualize clinic working and patients’ situations.
Characteristics of Patient Participants.a
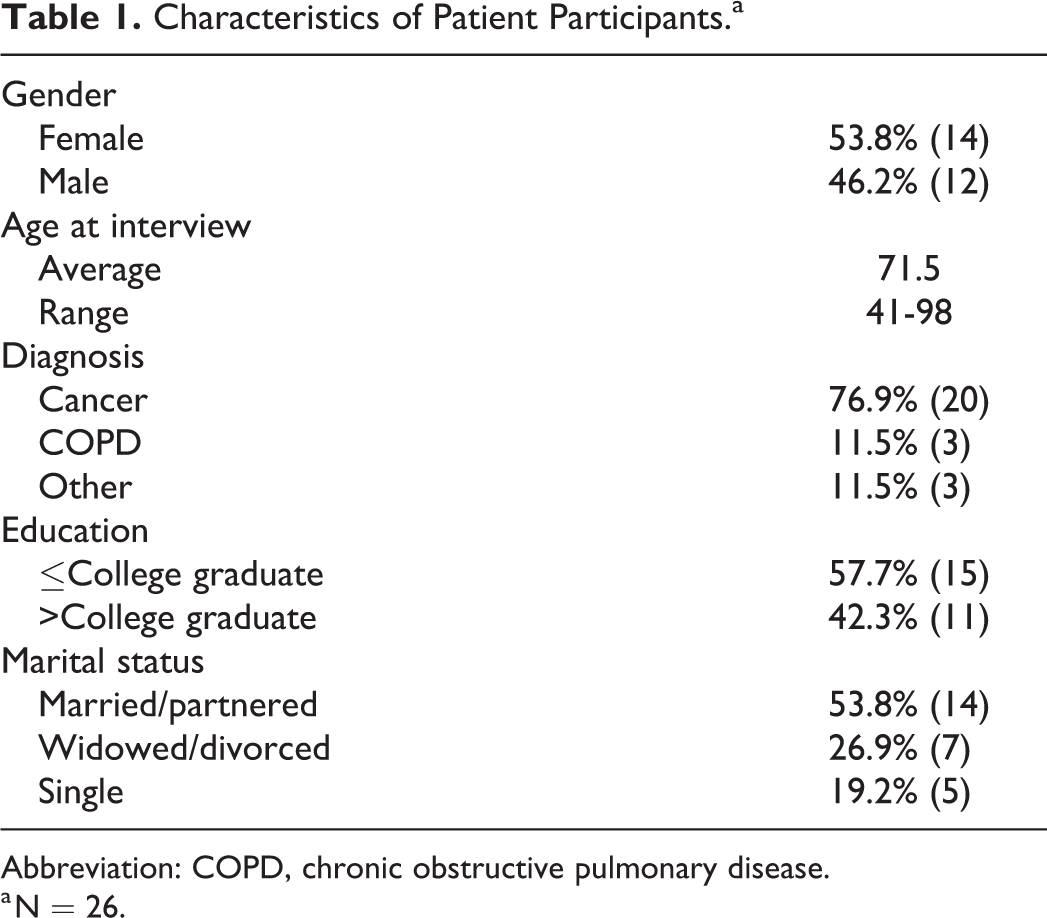
Abbreviation: COPD, chronic obstructive pulmonary disease.
a N = 26.
Data Collection
In-person, semistructured interviews were conducted by authors (K.L.S. and E.H.M.) at patients’ homes. Written informed consent was obtained prior to interviewing. All participants were advised that they could stop the interview if they found it distressing or did not feel well enough to continue, although this did not occur. A topic guide was developed based on a review of literature and previous work with physicians, who vetted the questionnaire for clinical authenticity and provided feedback before data collection started. The interview began with a history of the patient’s illness experience, followed by questions about key social supports; pathways by which they arrived in palliative care; past hospice exposure; and whether they would consider moving to hospice and under which circumstances.
We elected to not define hospice at the outset of the interview, nor did we ask participants to define it themselves. We also did not have information in advance about whether they had discussed hospice with anyone, though we answered technical questions about hospice as they arose. This approach allowed us to learn about participants’ native hospice assumptions and how those assumptions influenced decision-making. For these patients to receive hospice care, they would need to be certified by 2 physicians as having a life expectancy of 6 months and then would be required to relinquish their active care. A key benefit of hospice is that it can provide a care team in the event of an emergency, thus potentially preventing unwanted 911 calls, transfers, and hospitalizations. As patients become more ill, postponement of hospice enrollment left them increasingly vulnerable to such episodes.
All participants were given a US$25 gift card after completion of the interview. Data collection continued until data saturation was reached. All interviews were digitally recorded and transcribed verbatim.
Analysis
A phenomenological perspective was used to describe the meaning and significance of participants’ experiences with end-of-life medical decision-making. Analyses were conducted by all authors in 2017 to 2018, using an abductive framework that allows for concurrent inductive and deductive analyses. 26 Data were first coded in a word processing program, using the “comment” feature to allow all coders to make extensive comments in the margins as a coding scheme was developed. For each transcript, 2 authors coded and commented, and the third author reviewed and led in-person discussion of reconciliation of discrepancies and refinement of coding categories. Using constant comparative method, a final codebook was developed, and all transcripts were coded and reconciled by all authors. Next, we created a spreadsheet wherein coded excerpts were grouped together to allow for more in-depth thematic analysis with all the codes in one document and searchable by code, transcript location, and coding notes (eg, grouped by “hard no” or “soft no”). Themes were identified inductively with attention to understanding domains of patient challenges that may help explain late hospice referrals. Quotation excerpts presented here are representative of larger patterns.
Results
Defining a “Soft No”
We rarely observed patients providing definitive declinations of hospice; such “hard” refusals appeared in only 4 of 26 interviews. In these cases, patients typically resisted hospice based on having had negative prior experiences with hospice, religious preferences, or concerns about being able to maintain dignity and control over their situations after accepting hospice. One patient described her interlocking reasons for not wanting hospice despite her physician’s suggestion that she consider it: Well, I had a boyfriend I was with for 20 years and he died of colon cancer. And he was in hospice at his daughter’s. But the nurse only came one time. And we had to do all the stuff…It wasn’t pretty. And I was there with him the whole time…I don’t want that. Cause I am here believing for healing…[my] doctor just kinda doesn’t…give God credit. (Patient 5-014) [It is not the right time for hospice] unless she is suffering. And if she’s suffering, then that is a different story. By suffering we are talking about can’t breathe. You can’t eat…It is suffering where it’s to the point where it doesn’t seem to be a point of return. (Caregiver 6-008)
Reasons for a Soft No
We do not need those services (yet)
Patients and caregivers often claimed that they did not think hospice services were currently needed. Many families had already curated support networks to address curative, palliative, and home health-care needs, as well as supporting activities of daily living such as bathing, cooking, cleaning, and transportation as needed. These networks were tailored to patients and comprised of, for example, physicians, nurses, palliative care home service providers, family members, neighbors, colleagues, and community members who were able to respond to a wide range of needs and adjust over time to new circumstances. Often, these support networks were years in the making and family members in particular became expert caregivers. In many cases, it was unclear to patients and families what additional benefits may come by transitioning to hospice care.
For instance, one patient (5-019) shared how his daily activities, including playing piano, constructing train sets, social activities, and time with his family, were motivating factors in making decisions around his health. Palliative care made it possible for him to avoid hospitalizations and receive the treatments he needed to stabilize his health and continue to live independently with advanced bladder cancer. His granddaughter/caregiver explained: It’s very complicated, but I think we are doing a pretty good job meeting his needs. He doesn’t want to go anywhere. He wants to stay [in his home] and have his independence. (Caregiver 6-019)
I’m not dying (yet)
A second major justification patients provided for not currently wanting hospice was they felt it was premature. Even while acknowledging their terminal illnesses, participants often expressed that they were open to hospice, but it was not time since they were not yet dying, as this patient describes: Well, it’s like obviously I’m good enough to be well in certain ways. But, I’m pretty compromised in a lot of other ways. So, it’s not like [I’m ready for] hospice and actively dying. But it certainly is not…easy or comfortable living. (Patient 5-009) We both know, you know, if he makes the decision, at some point, to just stop the chemo and just be done with it all, you know…then yes. We would get ahold of hospice and we would let them know…. (Caregiver 6-001)
Social context of the “terrible choice”
Our data showcase the ways in which the “terrible choice” to stop active care in favor of hospice enrollment grows out of complex, established support networks that not only provide care but help define parameters of appropriate care and inform perceptions of timing. Patients count on their support networks to help them know where they are in an illness trajectory and when it might be appropriate to stop active care and/or consider a move to hospice. To the extent that these networks support an active care scenario (including use of palliative care), patients may be more likely to adopt a soft no posture toward hospice.
The role of health-care providers in helping patients make these assessments about timing and treatment options is especially critical. The below patient describes how he not only relies on his wife to help resolve the question of when to transition but also palliative care staff who come to his home, mentioning one of the nurses by name: Patient: I think [hospice] is a fantastic program. And I don’t have no issues with it. It’s just I’m not at that stage… Interviewer: And so then how do you think you’ll know when it’s time? Patient: I don’t really know. I really have to deteriorate to a point where I can’t function on my own the way I want to. And um…hopefully [my wife] will know what to do. But I think there is enough support through people like [the palliative care nurse] and [other palliative care] staff, who will help me. (Patient 5-002) I think about it like a trap. [Patients] know the nursing staff. They know the infusion nurses. They know the oncologist team. They have been with them for months to years, right? And then we [the palliative care team] come in. And who are we, right? (Palliative Care Staff 4-006)
Discussion
Our results show that hospice decisions are not simply dichotomous, one-time, individual-level decisions. 3 Rather, they are socially contextualized and unfold over time in response to uncertainty. In our study of one urban outpatient palliative care setting, patients overwhelmingly postponed hospice decisions with use of a “soft no” as opposed to providing a decisive declination. Such an approach allows patients to maintain the option of hospice should that care be required in the future. Justifications patients and caregivers offered for why hospice was not needed (yet) include patients not seeing the value added of hospice, assuming the timing is premature, and relying on extensive health-related support networks that either justify or endorse continuation of active care. 4
By stabilizing health care, providing expert health provider advice, and helping maintain the integrity of a support system that would be significantly dismantled by the discontinuation of active care, palliative care can disincentivize conversion to hospice. In offering a soft no, patients may be refusing hospice but are prioritizing their ability to “opt-in” to preservation of their normal function and social support systems to the extent possible. 27 Our data show how conversion to hospice entails cascading and interlocking disruptions to that social system, in turn creating the potential to incentivize delay—rather than facilitate—transition to hospice.
These issues beg the question of whether concurrent care is a meaningful solution to the problem of delayed hospice referrals: Would patients in our study be more amenable to hospice if they did not have to relinquish existing care? Would such a policy environment alleviate the pressure on them to resolve their uncertainty about their proximity to death and risk fracture of their current health support systems? In their examination of factors that influence the provision of concurrent care in the Veterans Affairs system, Haverhals et al 22 found that providers encourage hospice use by underscoring how it is always adding something to current services. Even then, it is still used relatively rarely, due in large part to administrative concerns about Medicare guideline compliance. This interplay between organizational constraints and patient decisions is consistent with the data we present above. Disentangling the relationships among individuals, support networks, various types of providers, payers, and policy will be critical for improving end-of-life health-care provision. The importance of long-term health-care support systems is not to be underestimated. In the context of current research underscoring the importance of routine palliative care consultation, 29,30 it is critical to also integrate an understanding of the underlying influences that constitute soft refusal so that patients’ needs can be more accurately and thoroughly met.
Patients in our purposive sample benefited from a large, interdisciplinary team of palliative care providers able to collaborate with medical teams; we do not claim that our results generalize to all palliative care organizations or geographic areas. Nevertheless, we believe there is reason to further investigate how social context (medical, social, and familial) influences decisions about hospice. Looking forward, there is a need to move beyond cognitive- and emotion-based paradigms of patient education and integrating social, organizational, and structural perspectives that show how hospice decision is socially contextualized.
Footnotes
Authors’ Note
This study was approved by the Colorado Multiple Institutional Review Board (protocol 14-0959).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received financial support for this research from University of Colorado Denver.