
Abstract
Objectives:
To estimate differences in spending and utilization between hospice users and non-users with lung cancer by length of hospice enrollment.
Study Design:
Retrospective analysis using 2009-2013 Medicare claims.
Methods:
The study sample was a 10% random sample of Medicare fee-for-service beneficiaries with lung cancer who died between 2010 and 2013. We identified different categories of hospice users (hospice enrollment for 1-7 days, 8-14 days, 15-30 days, 31-60 days, 61 days – 6 months) and non-users. We used propensity score matching to match users in each enrollment category with non-users. The outcomes were: a) total Medicare spending, b) number of hospitalizations, c) number of emergency department (ED) visits, d) number of physician-administered chemotherapy claims, and e) number of radiation therapy sessions. Regression analysis was used to compare outcomes between users and non-users by enrollment period.
Results:
Hospice users had significantly lower spending, fewer hospitalizations, and fewer ED visits than non-users across all categories of hospice enrollment. Large savings occurred when patients stayed in hospice for at least one month (US$16,566 for those enrolled 61 days – 6 months; US$16,409 for those enrolled 31-60 days). Significant reduction in use of outpatient services including chemotherapy and radiation therapy was observed among patients using hospice for at least 1 month.
Conclusions:
Hospice led to cost savings by reducing utilization of aggressive care towards end-of-life among lung cancer patients. While cost savings were realized even when hospice is utilized for a short duration, large savings occurred when hospice is used for at least 1 month.
Keywords
Hospice focuses on noncurative medical care, including pain and symptom management and emotional and spiritual well-being, to provide patients and their families with needed end-of-life care. 1 Cancer accounts for the largest category of diagnoses leading to hospice care, representing around 27% of hospice users. 1 Among the 4 most common cancers (breast, prostate, lung, and colorectal), hospice use is highest among patients with lung cancer at around 66.7%. 2 This is likely due to the severity of symptoms and poor prognosis of lung cancer; less than half of patients with lung cancer survive beyond 1 year of diagnosis. 3
A recent study by Kalidindi et al found that Medicare decedents with lung cancer who used hospice had significantly lower health-care spending than nonusers in the last 6 months of life, with most of the difference occurring in the final month of life. 4 This finding was consistent with studies of hospice use among patients with other conditions. 5,6 However, one limitation of these prior studies was that that they did not distinguish between patients with different lengths of hospice enrollment; instead, they lumped together patients who used hospice for 6 months or more with those enrolled for less than a week. A second limitation of prior work was that cost savings were estimated over long time intervals—such as last year of life, 5,6 last 6 months, 4 or last month, 7 while the median length of hospice use was only 17 days, and the average length of stay was around 88.2 days. 8 Given the variation in length of hospice enrollments, useful assessments of hospice savings must: (1) consider the patient’s actual length of hospice stay, and (2) use the period during which hospice is actually used for cost comparisons.
A few studies examined the impact of length of hospice enrollment on spending but produced mixed results. Some found that beneficiaries enrolled in hospice longer saved Medicare dollars more. 9,10 For example, Taylor et al 9 used Medicare claims data and found that hospice enrollment of 53 to 105 days before death maximized Medicare savings. Others showed that longer hospice stays were associated with higher Medicare spending because the costs of providing hospice exceeded savings from reduced utilization of other resources. 11,12 Kelley et al used survey data from the Health and Retirement Study along with Medicare claims data, and found that cost savings were higher for the most common enrollment periods: 1 to 7, 8 to 14, and 15 to 30 days before death, than the 53 to 105 period. 12 The difference in findings between these studies could be attributed to differences in study data, study periods, study samples, and study methodology. 9,12 For example, Kelley et al 12 had more comprehensive data that included information on patient functional status. Thus, they were able to control for some covariates that was unavailable to Taylor et al. 9
The studies by Kelley et al 12 and Taylor et al 9 included all Medicare decedents 9,12 (or all cancer decedents), 9 in their study sample. It is possible that the savings vary based on cancer type. For example, it is possible that for conditions such as lung cancer, longer hospice enrollments might lead to greater reductions in health spending. One study looked at the impact of hospice enrollment period on health-care utilization and costs for patients with poor-prognosis cancers. 13 It was found that the savings were maximized when patients enrolled in hospice 5 to 8 weeks before death. 13 However, this prior study was based on a single year of data, did not focus on a specific cancer type, and did not examine how hospice enrollment might affect utilization of different outpatient services such as chemotherapy and radiation therapy visits. Chemotherapy and radiation therapy are important drivers of cancer costs. Spending on each chemotherapy session among patients with lung cancer averages between US$1250 and US$1630 depending on site of chemotherapy. 14 Patients with lung cancer also receive more radiation therapy sessions than patients with other common cancers. 15 If services provided in hospice effectively substitute these aggressive services, hospice care could lead to substantial savings. Thus, examination of utilization of certain high-cost outpatient services can help us to better understand the potential mechanism by which hospice leads to savings.
The objective of our study was to examine the role of length of hospice enrollment on expenditures and utilization among patients with lung cancer. We used propensity score matching techniques to mitigate the selection bias, which is a common issue when studying the impact of hospice use. First, we created propensity score–matched cohorts of hospice users and nonusers across 5 different enrollment periods—(1) those enrolled for 1 to 7 days, (2) those enrolled for 8 to 14 days, (3) those enrolled for 15 to 30 days, (4) those enrolled for 31 to 60 days, and (5) those enrolled between 61 days and 6 months. Next, we examined spending and utilization differences during the target enrollment period between hospice users and nonusers. Similar to the study by Kalidindi et al, 4 we examined a comprehensive set of utilization measures including hospitalizations, emergency department (ED) visits, and use of select outpatient services including chemotherapy and radiation therapy sessions.
Methods
Data
Our primary data were the 2009 to 2013 Medicare claims including: Medicare Hospice claims; Part A Medicare Provider Analysis and Review files containing inpatient hospital and skilled nursing facility claims; Part B Medicare Hospital Outpatient files containing claims for services in hospital outpatient departments and Carrier files containing claims for services by noninstitutional providers; and Durable Medical Equipment (DME) files containing claims submitted by DME suppliers. The 2009 data were used only to observe 6 months of utilization prior to death for those who died in 2010.
Other data files included: Medicare Master Beneficiary Summary Files (MBSF) containing demographic characteristics and disease indicators for each beneficiary; American Community Survey (ACS) data containing zip-level income, education, and unemployment rates; and Hospice Compare files that provided information regarding the number of hospice providers serving the beneficiary’s zip.
Sample
The Centers for Medicare and Medicaid Services first identified all patients with cancer between 2009 and 2013 using 100% of Medicare claims and applying the standard algorithm used for creating cancer indicators in the Medicare Chronic Condition Warehouse files. 16 The research-identifiable claims and demographic information for a 10% random sample were then provided to us. From that sample, we identified beneficiaries with an indicator for lung cancer who died between 2010 and 2013.
We included only beneficiaries who were continuously enrolled in Medicare Part A and Part B for at least 6 months before death to ensure we could observe all utilization and spending data for the sample. We removed any beneficiaries who were enrolled in Medicare Advantage because their utilization information was not available to us. These exclusions resulted in a sample of 43 594 individuals.
Patients who enrolled in hospice at any time in the 6 months before death comprised the hospice user group. Beneficiaries enrolled for longer than 6 months were excluded. All patients who did not enroll in hospice comprised the nonuser group. Within the user group, we defined the following categories of enrollment period: those enrolled between 1 and 7 days, 8 and 14 days, 15 and 30 days, 31 and 60 days, and 61 days and 6 months.
We created the matched nonuser sample for each enrollment category using logistic regression. We estimated the propensity score of hospice enrollment using the covariates at the time of death. In general, the covariates included the following prior studies 9,13 : age, gender, race, time since diagnosis, chronic condition indicators (such as diabetes, hypertension, chronic obstructive pulmonary disease, etc), ZIP code-level income, education, unemployment rates, and number of hospice providers serving the ZIP code. Similar to the study by Kelley et al, 12 we included a covariate for the number of hospitalizations during the 6-month period prior to the target hospice enrollment period to account for prior utilization as a predictor of subsequent utilization (further details in Supplemental Appendix A1). We also added a metastasis indicator to partially capture the disease progression because the staging information was not available (Supplemental Appendix A1).
Next, we matched hospice enrollees with each enrollment period to nonhospice controls who were within 2% of the standard deviation of the propensity scores. All unmatched patients were excluded. We assigned a hypothetical enrollment date to each nonuser in a way that the time from enrollment to death was the same for the nonuser as their matched user.
Outcome Measures
(a) Spending: For each enrollment period group, we defined the primary outcome as the total Medicare spending from the beginning of the enrollment period to death. For the nonenrolled, the enrollment date was the assigned date based on matching (described above). Spending included the Medicare allowed payments for all inpatient stays, ED visits, outpatient procedures, visits, and drugs, DME, and hospice care. All costs were adjusted for inflation to 2013 USD using Consumer Price Index (further details in Supplemental Appendix A1).
(b) Utilization: For each enrollment period group, we identified the number of hospital visits, the number of ED visits, number of part B chemotherapy claims, and number of radiation therapy sessions from the outpatient claims data (further details in Supplemental Appendix A1).
Statistical Approach
First, we descriptively compared the covariates between hospice users in each enrollment period category and the overall sample of nonusers before matching. Next, using the matched groups, we compared covariates between each set of hospice users and their propensity score–matched nonusers to check the balance of the sample on observable covariates.
We compared unadjusted spending between hospice users and matched controls by enrollment period. We then estimated spending using generalized linear models with log-link and γ distribution separately for each enrollment period. 4,12 For count measures of utilization, we estimated negative binomial models. 4,12 The same set of covariates were included in the regression analysis as in the matching. For each outcome, we computed regression-adjusted predicted values among hospice users and nonusers after setting all other covariates to their mean values. All standard errors were clustered by zip because patients within the same zip share similar characteristics.
Sensitivity Analysis
We also ran analysis using a separate category of enrollees enrolled for 53 to 105 days to compare our results with prior studies using that category. For example, Kelley et al, 9 used enrollment periods of 1 to 7, 8 to 14, 15 to 30, and 53 to 105 days before death.
Results
Sample Characteristics
The characteristics of the sample before matching are summarized in Supplemental Appendix Table A2. In general, patients who used hospice were likely to be older, female, white, and had a higher likelihood of metastatic cancer than nonusers. Comparison of the patient characteristics in the matched samples by enrollment period is reported in Supplemental Appendix Tables A3 to A7. These tables indicate that matching resulted in cohorts that were better balanced on covariates.
Spending Measures
Figure 1 presents comparison of unadjusted mean spending between hospice users and nonusers in matched cohort. Longer enrollment periods were associated with larger savings with the largest savings of US$18 779 realized when beneficiaries enrolled for 61 days to 6 months (P < .01). Figure 2 presents the regression-adjusted mean spending differences between hospice users and matched nonusers by enrollment period. The trends in regression-adjusted spending by enrollment period were similar to the unadjusted measures, but the magnitude of savings was lower in the adjusted measures. Medicare lung cancer decedents who received hospice care for 61 days to 6 months had spending of US$20 107 during the period enrolled compared to matched nonusers who had spending of US$36 762 during the same period—a difference of US$16 566 (P < .01). The estimates of savings were US$16 409 (P < .01) for those enrolled between 31 and 60 days, US$12 209 (P < .01) for those enrolled for 15 to 30 days, US$8678 (P < .01) for those enrolled 8 to 14 days, and US$3714 (P < .01) for those enrolled 1 to 7 days.
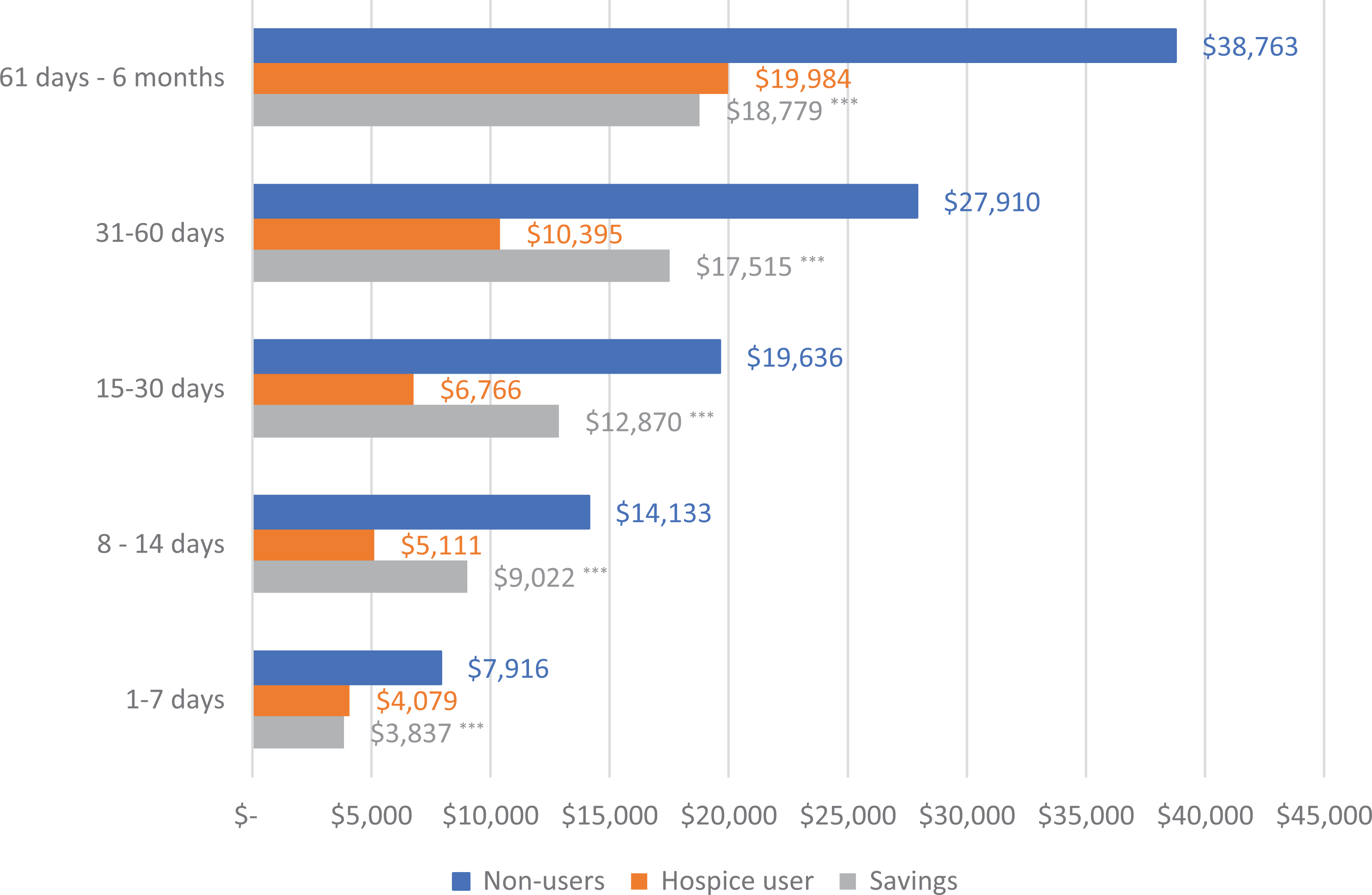
Enrollment period acategory wise comparison of unadjusted mean spending between hospice-users and their matched bnonusers and estimates of savings (among Medicare beneficiaries with lung cancer). Note: aFor hospice enrollees, enrollment period refers to the period between the hospice enrollment to death. For nonusers, enrollment period refers to the periods between the assigned enrollment date (based on propensity score matched hospice user) and death. bThe matched sample of hospice users and nonusers in each enrollment category.
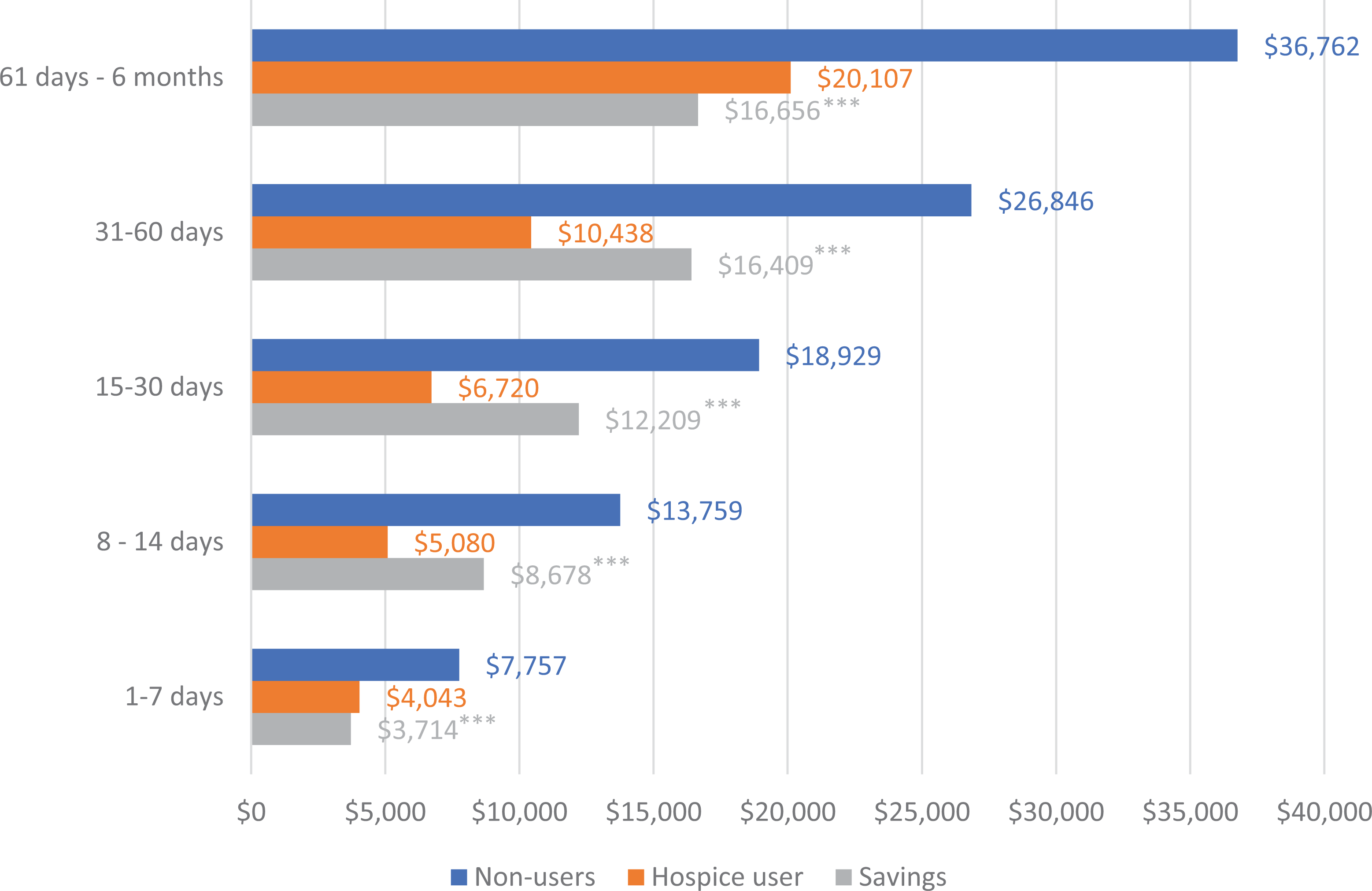
Enrollment period acategory wise comparison of adjusted bmean spending between hospice users and nonusers and estimates of savings (among Medicare beneficiaries with lung cancer). Note: aFor hospice enrollees, enrollment period refers to the period between the hospice enrollment to death. For nonusers, enrollment period refers to the periods between the assigned enrollment date (based on propensity score matched hospice user) and death. bUsing the matched sample of hospice users and nonusers in each enrollment category, spending during the enrollment period was adjusted for patient and market characteristics using GLM model with log link and γ distribution. Standard errors accounted for clustering within a ZIP. Value are predicted values among hospice users and nonusers after setting all the other covariates to their mean values; *P < .05, **P < .01, ***P < .001. GLM indicates generalized linear models.
Utilization Measures
Figure 3 presents regression-adjusted mean utilization measures for each group. In general, the utilization trends for hospitalization visits, and ED visits were similar (panels A and B). Beneficiaries who used hospice for 61 days to 6 months had significantly fewer hospital visits (1.02 fewer visits, P < .01), and fewer ED visits (0.33 fewer visits, P < .01), than matched nonusers. The estimated differences in number of hospitalization visits were −0.74 (P < .01) for those enrolled between 31 and 60 days, −0.50 (P < .01) for those enrolled for 15 to 30 days, and −0.28 (P < .01) for those enrolled 8 to 14 days, and −0.04 (P < .01) for those enrolled 1 to 7 days. The estimated differences in number of ED visits were −0.21 (P < .01) for those enrolled between 31 and 60 days, −0.14 (P < .01) for those enrolled for 15 to 30 days, −0.09 (P < .01) for those enrolled 8 to 14 days, and −0.06 (P < .01) for those enrolled 1 to 7 days.
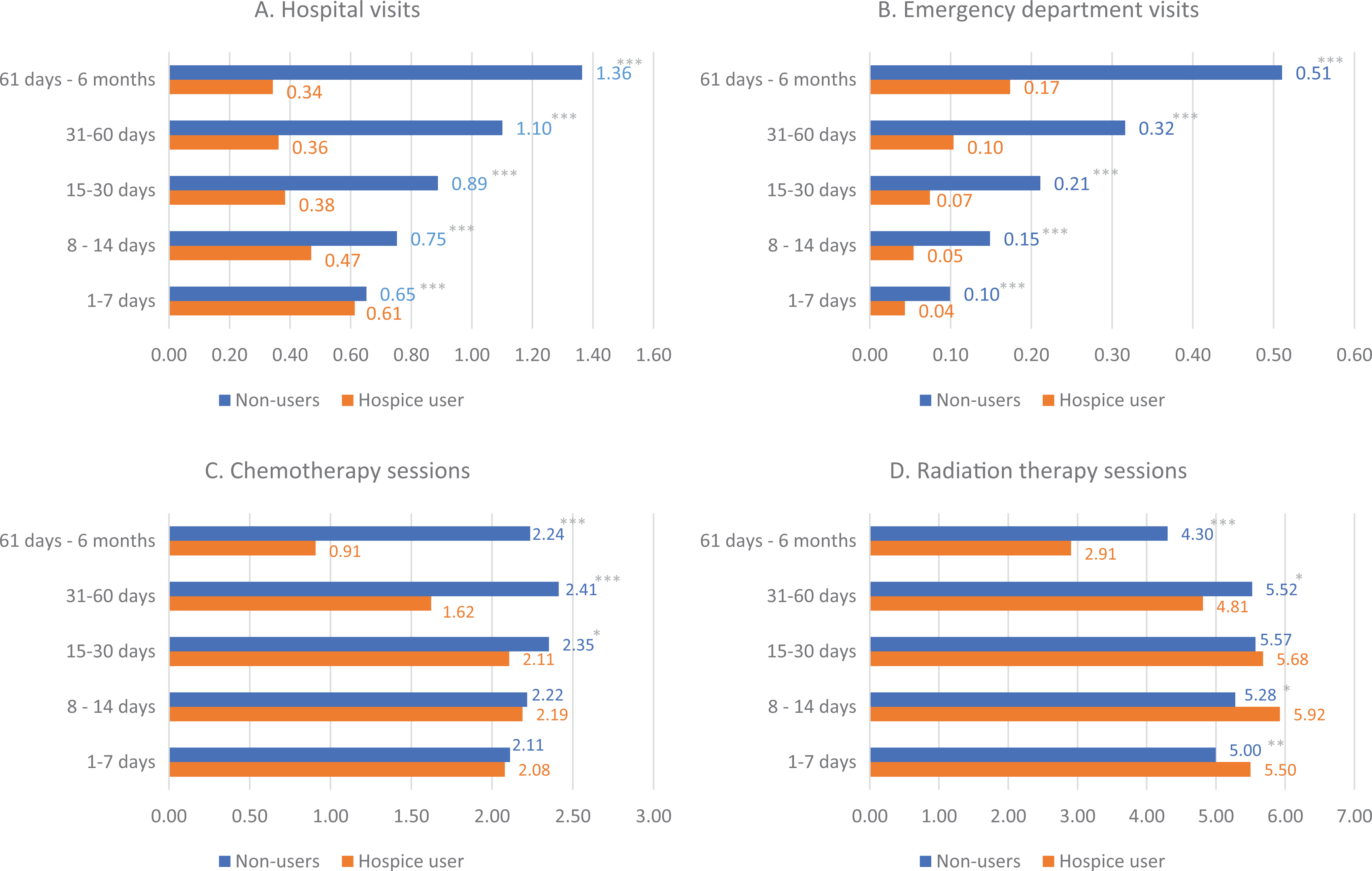
Enrollment period acategory wise comparison of adjusted bmean utilization between hospice users and nonusers (among Medicare beneficiaries with lung cancer). Note: aFor hospice enrollees, enrollment period refers to the period between the hospice enrollment to death. For nonusers, enrollment period refers to the periods between the assigned enrollment date (based on propensity score matched hospice user) to death. bUsing the matched sample of hospice users and nonusers in each enrollment category, the number of visits (counts) during the enrollment period was adjusted for patient and market characteristics using negative binomial regression models. Standard errors accounted for clustering within a ZIP. Value are predicted values among hospice users and nonusers after setting all the other covariates to their mean values; *P < .05, **P < .01, ***P < .001 for the estimates of difference between the 2 groups.
For outpatient visits (panels C and D), beneficiaries who received hospice care for longer durations (eg, 61 days-6 months) had a much lower number of chemotherapy visits (−1.33 visit difference, P < .01), and a lower number of radiation therapy sessions (−1.40 visit difference, P < .01) than matched nonusers. Lower chemotherapy (−0.78 visits difference, P < .01) and radiation therapy (−0.71 visits difference, P = .02) utilization was also seen for those enrolled between 31 and 60 days. However, unlike hospitalizations and ED visits, lower utilization was not seen for these services across all enrollment periods. While chemotherapy use was slightly lower among those enrolled in hospice for 15 to 30 days before death (−0.25 visit difference, P = .02), no significant difference in chemotherapy utilization was seen for those that were enrolled for 8 to 14 days or 1 to 7 days. For radiation therapy sessions, no difference was seen between hospice users enrolled 15 to 30 days and matched nonusers. Conversely, for those enrolled for shorter periods of 0 to 7 and 8 to 14 days, radiation therapy sessions were greater among hospice users than nonusers (0.64 visit difference, P = .02 for enrollment period 8-15 days; 0.50 visit difference, P = .01 for enrollment period 1-7 days).
Sensitivity Analysis
Using a separate category of beneficiaries that enrolled for 53 to 105 days did not impact our results (Supplemental Appendix A8). Savings using this enrollment category were around US$16 590 (P < .01), similar to the estimated savings for hospice enrollment of 61 days to 6 months and 31 days to 60 days.
Discussion
We found that longer lengths of hospice were associated with greater savings in Medicare costs among lung cancer decedents. We observed a clear gradient by length of hospice enrollment with those enrolled for longer periods of time experiencing greater reductions in spending. The savings increased substantially by each enrollment period category up to 31 to 60 days before death, but the change beyond this category was minimal. The incremental savings from having 61 days to 6 months of hospice enrollment versus 31 to 60 days of enrollment was only around US$250 (US$16 656 vs US$16 409). Our study confirms findings from prior studies that hospice saves money across different enrollment periods (up to 105 days shown by Kelley et al 12 and 233 days shown by Taylor et al 9 ). However, while the study by Kelley et al 12 found that the savings are maximized between 15 and 30 days, we found the savings were larger for longer enrollment periods up to 6 months. Our estimates of savings were also larger compared to the prior studies that included all Medicare patients. 9,12 Our results were likely driven by our selection of patients with lung cancer, who have particularly high utilization of services and spending compared to other patients with cancer in the last year of life. 17
Trends in utilization clearly drove the differences in savings across enrollment periods. Hospice use reduced hospitalizations and ED visits across all enrollment periods. The number of hospitalizations decreased by 1.02 for those enrolled for 60 days to 6 months and by 0.04 for those enrolled 1 to 7 days before death. The adjusted decrease in number of ED visits was 0.34 for those enrolled for 60 days to 6 months and 0.06 for those enrolled 1 to 7 days before death. These findings are consistent with other studies. 12
An important contribution of our study is that we show trends in utilization of outpatient services such as chemotherapy and radiation therapy differed significantly between hospice users and nonusers based on the enrollment period. For example, while beneficiaries that initiated hospice only 1 to 7 days before death had higher utilization of services such as radiation therapy, and similar utilization of chemotherapy as their matched nonusers, those that used hospice for longer than 30 days had reduced utilization of both services. Chemotherapy and radiation therapy are sometimes used for palliative purposes during end of life. But the benefits were found to be limited considering the toxicity due to chemotherapy, the health-care costs, and the time spent on these sessions at the hospital. 18 -20 Thus, reductions in aggressive care toward end of life could be beneficial to the patient.
Limitations
There are several limitations of this study. First, while our propensity score approach was able to match hospice users and nonusers on observable characteristics, there may still be differences in unobservable characteristics. For example, we do not have information on patient preferences available to some researchers. 12 Second, we did not have home health data; however, our estimates excluding home health costs are likely to be conservative because nonusers could potentially use home health to substitute for services provided in hospice. Third, we did not have cancer stage information. While we used an indicator for metastasis, there may be important differences in stage that we are unable to capture. 21,22 Last, enrollment period could also be impacted by time of diagnosis. A large number of patients with lung cancer are diagnosed in advanced stages of the disease. 23 It is possible that the difference between an individual who enrolled for 30 days versus 60 days was influenced by their time of diagnosis rather than patient preference.
Conclusion
Among patients with lung cancer, hospice leads to lower spending across all enrollment periods up to 6 months before death—the current period used to determine hospice eligibility. Longer enrollment appears to be associated with greater savings, likely driven by greater reductions in utilization of different services including inpatient hospitalizations, ED visits, and chemotherapy and radiation therapy sessions. Length of hospice enrollment may be driven by a variety of factors such as patient and family choice, and provider’s ability to accurately assess prognosis. Thus, it is important to assess and overcome some of the patient barriers toward hospice enrollment. Additionally, providers must weigh all patient and family factors against the benefits of early enrollment while formulating an end-of-life treatment plan.
Supplemental Material
Appendix - Impact of Length of Hospice on Spending and Utilization Among Medicare Beneficiaries With Lung Cancer
Appendix for Impact of Length of Hospice on Spending and Utilization Among Medicare Beneficiaries With Lung Cancer by Yamini Kalidindi, Jeah Jung, Joel Segel and Douglas Leslie in American Journal of Hospice and Palliative Medicine®
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH/NIA grant number 1R01AG047934-01, and NIH grant number R24 HD041025.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.