
Abstract
Background:
The Palliative Care and Rapid Emergency Screening (P-CaRES) tool has been validated to identify patients in the emergency department (ED) with unmet palliative care needs, but no prognostic data have been published. The Palliative Performance Scale (PPS) has been validated to predict survival based on performance status and separately has been shown to predict survival among adults admitted to the hospital from the ED.
Objective:
To concurrently validate the 6-month prognostic utility of P-CaRES with a replication of prior studies that demonstrated the prognostic utility of the PPS among adults admitted to the hospital from the ED.
Design:
Prospective cohort study.
Setting/Subjects:
Adults >55 years admitted to the hospital from the ED at an urban academic hospital in South Carolina.
Measurement:
Baseline PPS score and P-CaRES status were evaluated within 51 hours of admission. Vital status at 6 months was evaluated by phone or chart review.
Results:
131 of 145 participants completed the study. Six-month survival was 79.2% of those with a PPS of 60-100 (22/106 died) and 48% of those with a PPS of 10-50 (13/25 died) (p = 0.0004). Six-month survival was 85.2% for P-CaRES negative (13/88 died) and 48.8% for P-CaRES positive (22/43 died) (p < 0.0001). The inferred hazard ratio (HR) for PPS 10-50, as compared to PPS 60-100 was 3.003 (95%CI (1.475, 6.112) p = 0.0024) and the HR for P-CaRES positive, as compared to P-CaRES negative was 4.186 (95%CI (2.052, 8.536) p < 0.0001).
Conclusion:
The P-CaRES tool and PPS can predict 6-month survival of older adults admitted from the ED.
Keywords
Introduction
Inpatient palliative care has been associated with increased patient satisfaction, lower health care costs following discharge, fewer ICU admissions on hospital readmission, and longer median hospice stays in a randomized controlled trial. 1 As awareness of the potential benefits of palliative care increased, the American College of Emergency Physicians (ACEP) recognized the unique opportunity that emergency clinicians have in determining patients’ trajectory of care and made addressing end of life care a priority. 2,3 As a result, in 2013 the ACEP joined the ABIM Foundation’s “Choosing Wisely” campaign with the recommendation “Don’t delay engaging available palliative and hospice care services in the ED for patients likely to benefit.” 4 In the time since that initiative, Grudzen et al. demonstrated in a randomized clinical trial that emergency department initiated palliative care consultation for patients with advanced cancer improved their quality of life and did not shorten survival. 5 A recent systematic review of palliative care consultation or referral in the ED found that interventions in the ED improved quality of life compared to usual care, expedited palliative care consultation during admission, and that palliative care in the ED is feasible. 6
Several studies have demonstrated that ED clinicians acknowledge the utility of palliative care in the emergent setting, but that they may benefit from predetermined criteria and mechanisms to initiate palliative care. 7,8 In an attempt to facilitate identification of those that might benefit from palliative care consultation, the Palliative Care Rapid Emergency Screening (P-CaRES) tool was developed. 9 The P-CaRES tool involves 2 steps outlined in Figure 1. The first step identifies if patients have a life-limiting condition. The second step identifies if the patient has 2 or more unmet palliative care needs and, if so, palliative care consultation is indicated. The tool demonstrated content validity, reliability, and acceptability to palliative care specialists and emergency medicine clinicians. 10 A systematic review by George et al. evaluated palliative care screening methods in the ED and proposed several characteristics of an optimal screening tool, such as a time to screen of 1-2 minutes, assessment of functional status, and prognostication. 11 While numerous methods of prognostication exist, one of the goals of the current study is to assess if P-CaRES status itself predicts survival. As a prospective implementation of the P-CaRES tool has not yet been published, no prognostic metrics exist.
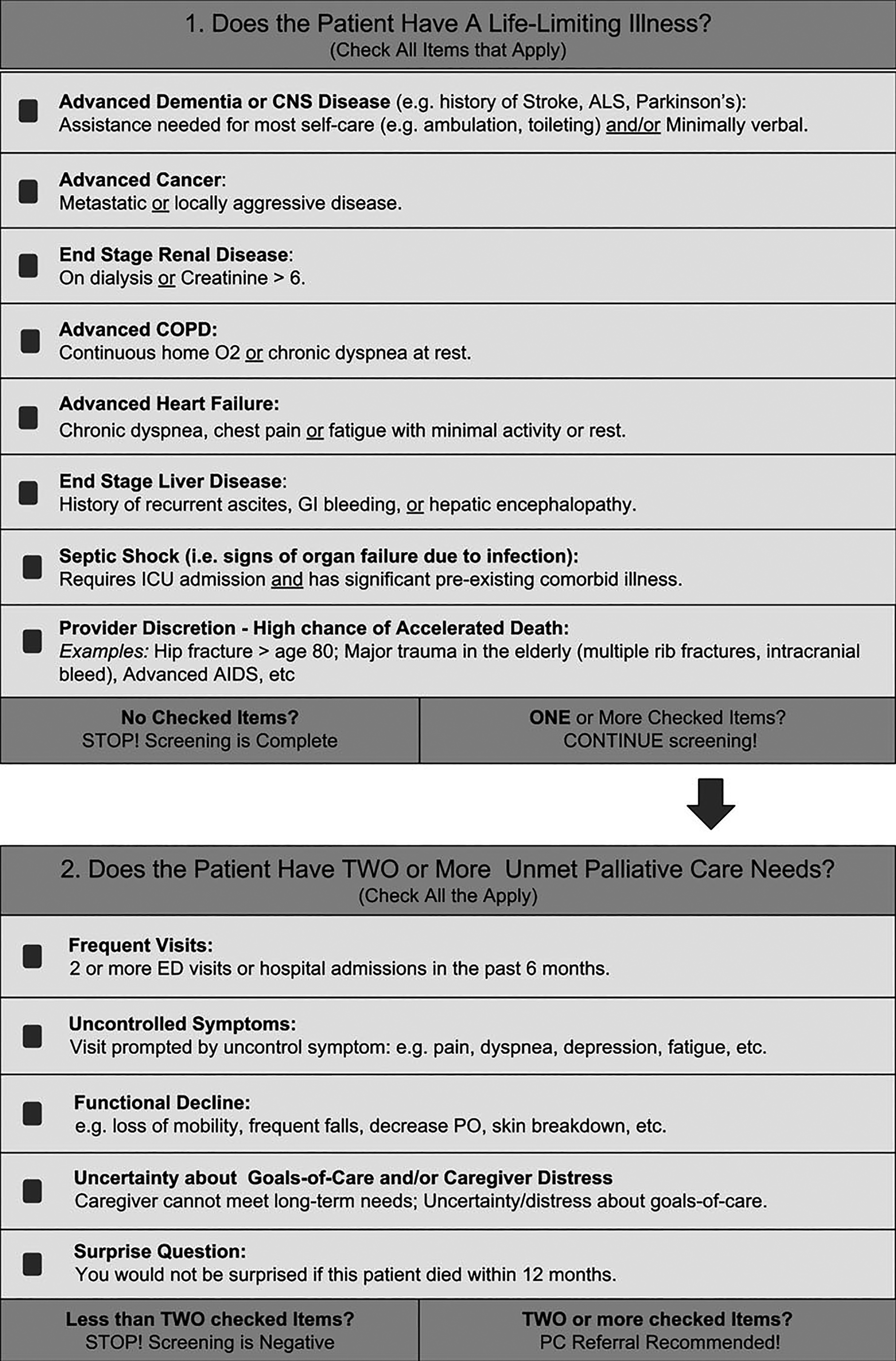
Palliative care and rapid emergency screening tool.
The P-CaRES tool incorporates a component of prognostication by asking if the clinician would be surprised if the patient died within the following year. However, the P-CaRES tool was not specifically designed for prognostication alone, and thus we seek to validate this use with a measure of functional status that has been shown to predict survival. The Palliative Performance Scale (PPS) was developed by the Victoria Hospice Society in order to facilitate communication of patient functional status, provide a useful measure of patient care needs, and for prognostication. 12 The PPS was based on the Karnofsky Performance Scale (KPS) that included assessment of ambulation, activity/extent of disease, and self-care, and then added further functional specificity by assessing oral intake and level of consciousness. The PPS also removed language dependent on patient location, making it applicable across clinical settings. Downing et al. conducted a systematic reviewed of several studies that demonstrated construct validity of the PPS as a prognostic tool by demonstrating a direct ordinal relationship between each PPS score and patient survival. 13 These studies affirmed this relationship across multiple clinical settings including a tertiary hospital at the time of palliative care consultation, an inpatient palliative care unit, as well as among outpatient and inpatient hospice patients. More recent studies have supported the use of PPS for prognostication of a general population of adult patients in the ED, but they were limited by small sample size and racial homogeneity. 14,15 The PPS benefits from being a more rapid assessment than the P-CaRES tool.
The current study seeks to establish survival estimates of both P-CaRES positive patients and performance status as assessed by the PPS. In doing so, we hope to replicate the findings demonstrating the prognostic utility of the PPS in the ED in a more diverse sample, while simultaneously validating the prognostic utility of P-CaRES. Having accurate survival estimates of applicable patient populations would help inform early goals of care conversations, potentially even while still in the ED. We hypothesize that P-CaRES positive patients will have a significantly decreased survival. Additionally, we hypothesize that a decreased PPS will concurrently be associated with decreased survival.
Methods
Overview
This study is a prospective cohort design that involved patients admitted through the ED at an urban academic tertiary care center in South Carolina. The methods were approved by the Institutional Review Board.
Participants
This study was conducted by consideration of all patients admitted through the ED from late September through October 2017. Potential participants were successively identified via daily reports generated from the electronic medical record showing those patients aged 55 or older who had been admitted to the hospital in the prior 24 hours. The potential participant’s care team was then approached by a co-investigator who confirmed inclusion or exclusion criteria of the patient. Inclusion criteria consisted of patients age 55 or older and patients with an admission order for acute or critical care services from the ED. Those patients excluded from participation were prisoners, patients with primary psychiatric diagnosis, patients under observation status, non-English speaking patients, and those patients or legal representatives with an inability or unwillingness to give informed consent. There was no plan to exclude any gender or racial groups. Non-English speaking participants were excluded for practical purposes of not having the funding to support translation services and because their exclusion was judged to be unlikely to alter the study endpoints.
Once the participant was confirmed to meet inclusion criteria, a member of the patient’s care team solicited participation in a research project to the potential research participant and/or their legal representative. If the participant or their legal representative verbally agreed to consider participation in the study, the co-investigator approached the patient and/or legal presentative, explained the nature of the study, enrolled that participant via written informed consent and then completed the interview for all study items.
Data Collection
The enrollment process consisted first of chart review followed by an in-person interview by 1 of 3 trained co-investigators who were all hospice and palliative medicine fellows. The co-investigators screened participants using the P-CaRES tool (Figure 1) with information gathered from chart review or by direct assessment during interview with the participant and/or primary caregiver. Detailed instructions for completing the P-CaRES tool can be found in George et al. 9 Participants screen positive for palliative care referral were defined as P-CaRES positive.
The co-investigator then assessed a baseline PPS of the participant in the standard manner on a scale from 10 to 100 by asking the participant or their caregiver questions about their functional capacity, including; ambulation, activity/evidence of disease, self-care, dietary intake, and level of consciousness. The baseline PPS was assessed regarding the participant’s functional status just prior to the inciting events of their admission. Participants were defined as having a PPS of 10-50 if their functional status was as follows, or worse: mainly sit/lie, unable to do any work, has extensive disease, and considerable assistance required for self-care. Finally, the participant and/or caregiver was asked if they could be contacted by phone to repeat PPS questioning at 3 and 6 months after initial data was collected.
Follow Up Data Collection
The participants were called 3 and 6 months after admission to the hospital to reassess their PPS at that time. Date of death was assessed by review of the medical record, report of the caregiver when attempting to contact the patient, and internet search of obituaries. Patients not confirmed deceased were contacted again at 6 months. Those patients not successfully contacted at either 3 or 6 months were coded as lost to follow-up and the data censored as of their last confirmed contact within the medical record up to 6 months after admission.
Outcomes
The primary endpoint was 6-month survival after admission to the hospital. Covariates include age, race, gender, marital status, prior hospice or palliative care, PPS score, and P-CaRES score.
Analysis
Participants were grouped by baseline PPS with ranges of 10-50 and 60-100. Participants who met criteria for palliative care consultation according to the P-CaRES tool were categorized as P-CaRES positive, in contrast to P-CaRES negative for those not meeting criteria. Univariate statistical comparisons were made using Fisher Exact and Analysis of Variance (ANOVA) tests. Survival plotting were created using Kaplan-Meier survival technique. A multivariable Cox proportional hazard model was used to control for interacting factors of age, gender, race, marital status, PPS Score, and P-CaRES status. Separate multivariable cox models were run for PPS and P-CaRES as the 2 variables were so highly correlated. Prior hospice or palliative care status was too correlated with age, PPS score, and P-Cares score to be included in the multivariable models. SAS 9.4 (SAS Institute Inc., Cary, NC) was used for statistical analyses.
Results
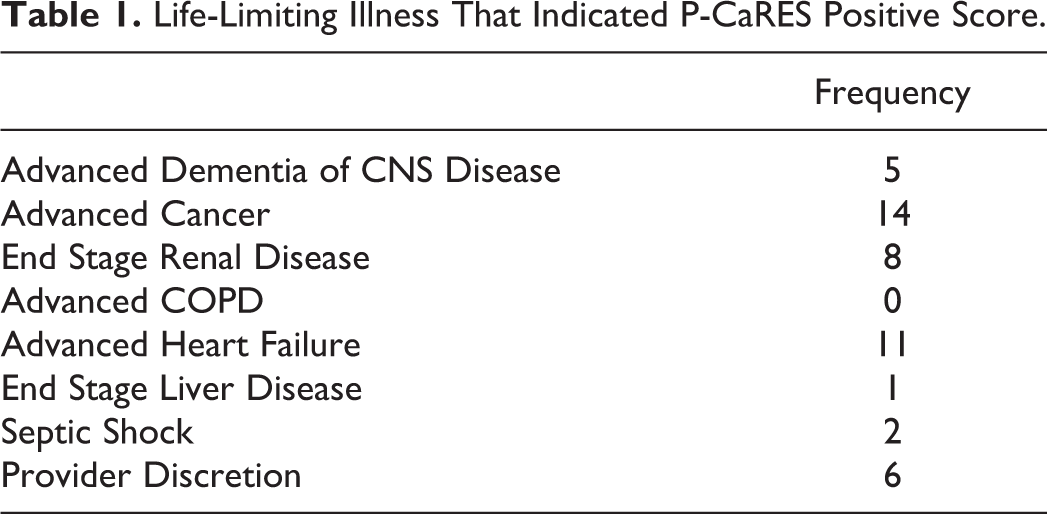
Enrollment was conducted from August 2017 through October 2017. Of the 348 screened for inclusion, 145 participants were enrolled in our study, and 131 were followed to 6 months or death. Reasons for patients declining participation included lack of decision-making capacity and/or legal guardian representation, unmet symptom burden, or simply that they were not interested in participating in a research study. Participants were enrolled a mean of 26.2 hours after admission (SD: 8.7, range 1-51). The frequencies of life-limiting illnesses that caused a participant to have a positive P-CaRES are outlined in Table 1.
Life-Limiting Illness That Indicated P-CaRES Positive Score.
Univariate analysis (Table 2) revealed similar demographics within the 2 P-CaRES statuses (positive and negative) and 2 PPS groups (10-50 and 60-100) with only several exceptions. The mean age of P-CaRES positive patients was greater than that of P-CaRES negative status, but not significant when stratified by 10 year groupings. No significant differences by age existed between the 2 PPS groups. P-CaRES status varied significantly by PPS. The PPS 60-100 group had a significantly higher proportion of patients with P-CaRES negative status than the PPS 10-50 group, and conversely a lower proportion of patients with P-CaRES positive status. Both P-CaRES and PPS varied significantly by prior hospice or palliative care and by death at 6 months. The P-CaRES positive and PPS 10-50 group had significantly higher proportion of patients who had received hospice or palliative care compared to the P-CaRES negative and PPS 60-100 group, respectively. The P-CaRES positive and PPS 10-50 group had significantly higher mortality rates at 6 months compared to the P-CaRES negative and PPS 60-100 group, respectively.
Demographics.
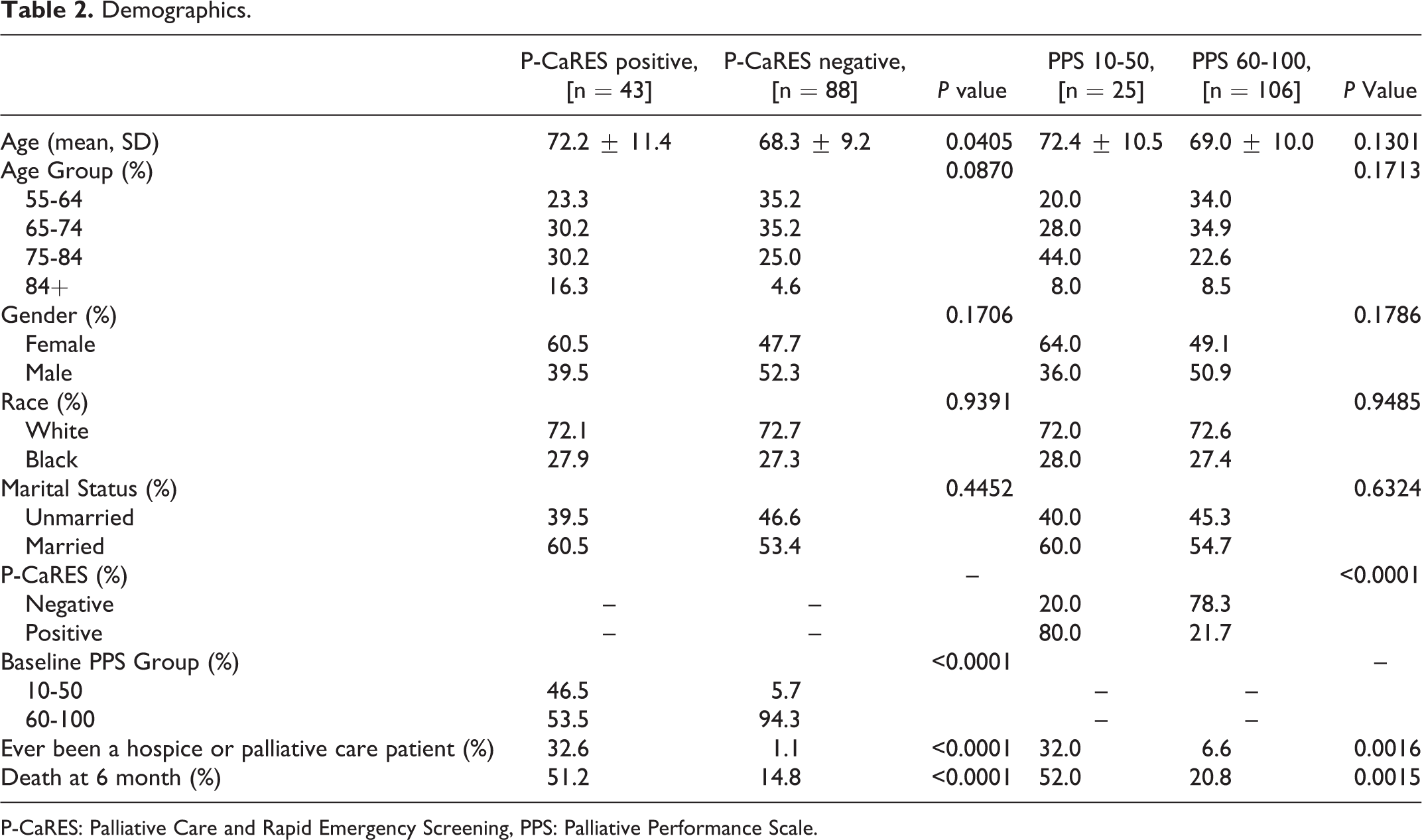
P-CaRES: Palliative Care and Rapid Emergency Screening, PPS: Palliative Performance Scale.
The multivariable analyses confirmed the significant increase in mortality associated with P-CaRES positive (Table 3). From this model, the inferred hazard ratio (HR) of P-CaRES positive, as compared to P-CaRES negative was 4.186 (95%CI (2.052, 8.536) p < 0.0001), implying that the risk of dying is roughly 4 times greater for the P-CaRES positive patients than the P-CaRES negative patients. In terms of other predictors of mortality, older aged patients tended to have slightly higher mortality rates than younger patients (p = 0.0163). The Kaplan-Meier survival curves by P-CaRES grouping are shown in Figure 2 with survival measured in days from time of admission to death or up to 180 days. The results are supportive of those from the univariate and multivariable mortality results suggesting that P-CaRES positive patients have higher mortality through time.
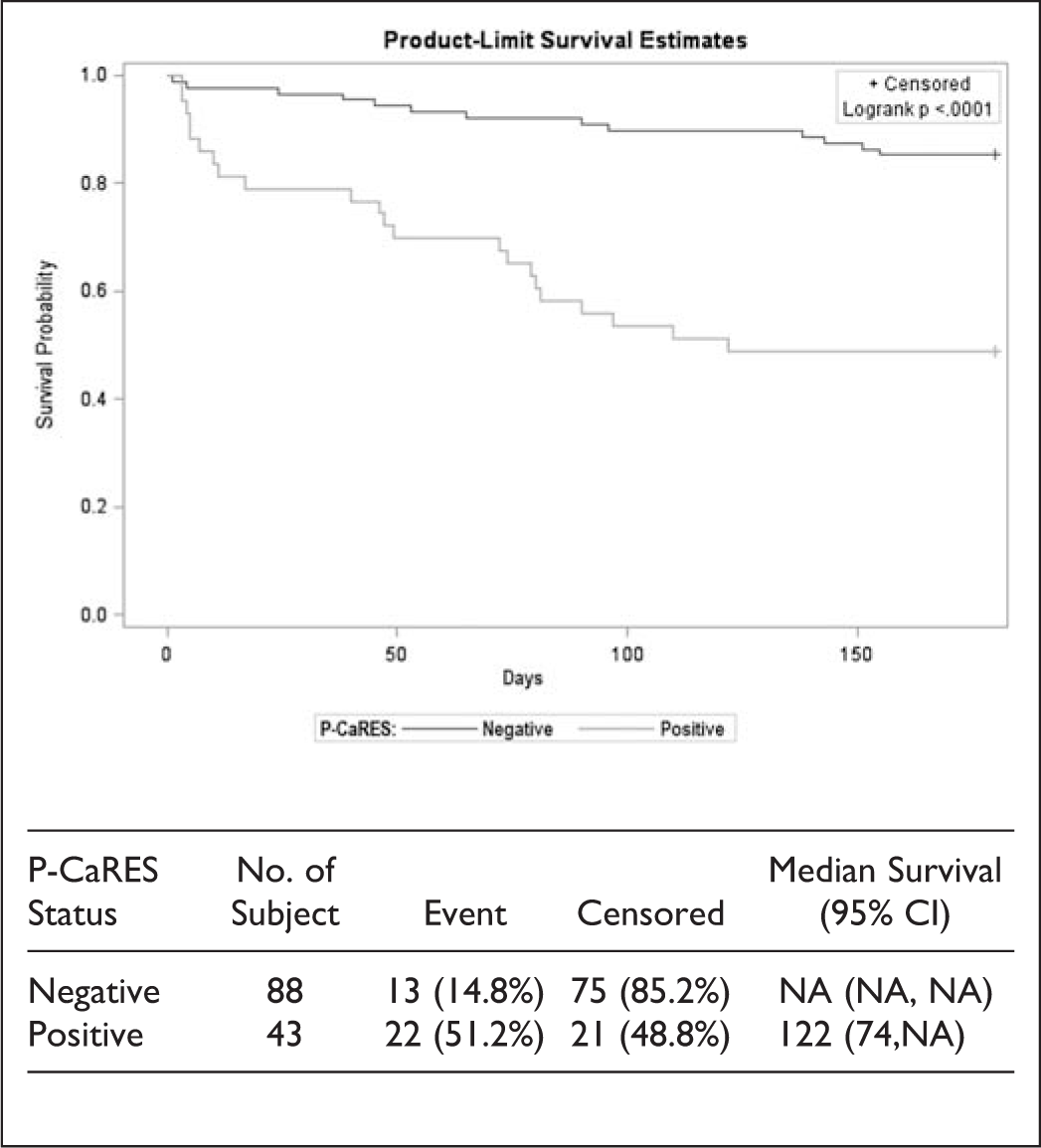
Kaplan-Meier plot by P-CaRES status.
Survival Analysis Model Results (P-CaRES as Primary Covariate).
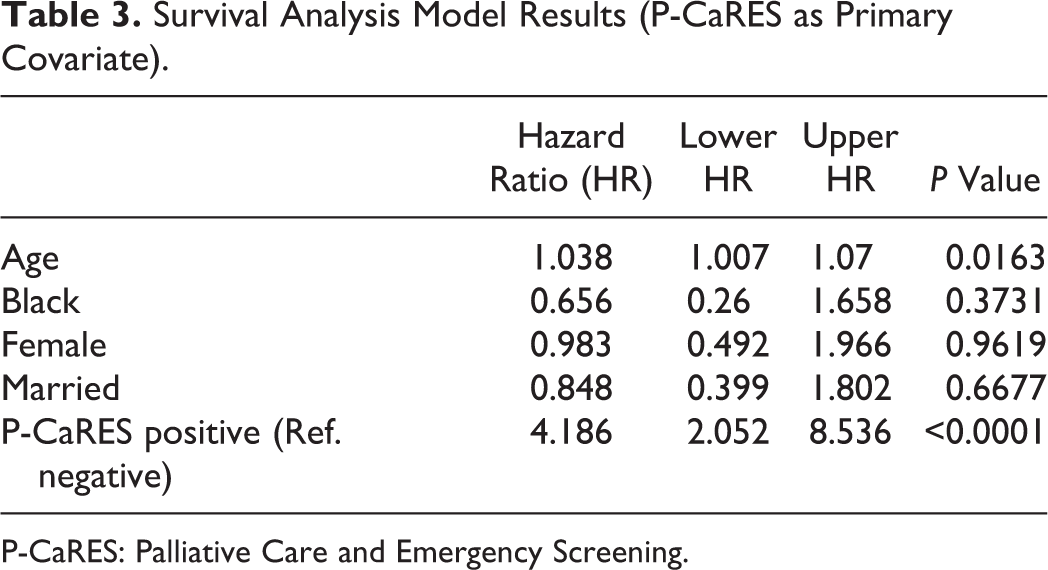
P-CaRES: Palliative Care and Emergency Screening.
The multivariable analyses confirmed the significant increase in mortality associated with the PPS 10-50 group (Table 4). From this model, the inferred hazard ratio (HR) of the PPS 10-50 group, as compared to the PPS 60-100 group was 3.003 (95%CI (1.475, 6.112) p = 0.0024), implying that the risk of dying is roughly 3 times greater for the PPS 10-50 group than the PPS 60-100 group. Similar to the P-CaRES model, older aged patients tended to have slightly higher mortality rates than younger patients (p = 0.0036). The Kaplan-Meier survival curves by PPS group are shown in Figure 3 with survival measured in days from time of admission to death or up to 180 days. The results are supportive of those from the univariate and multivariable mortality results suggesting that PPS 60-100 groupings have lower mortality through time.
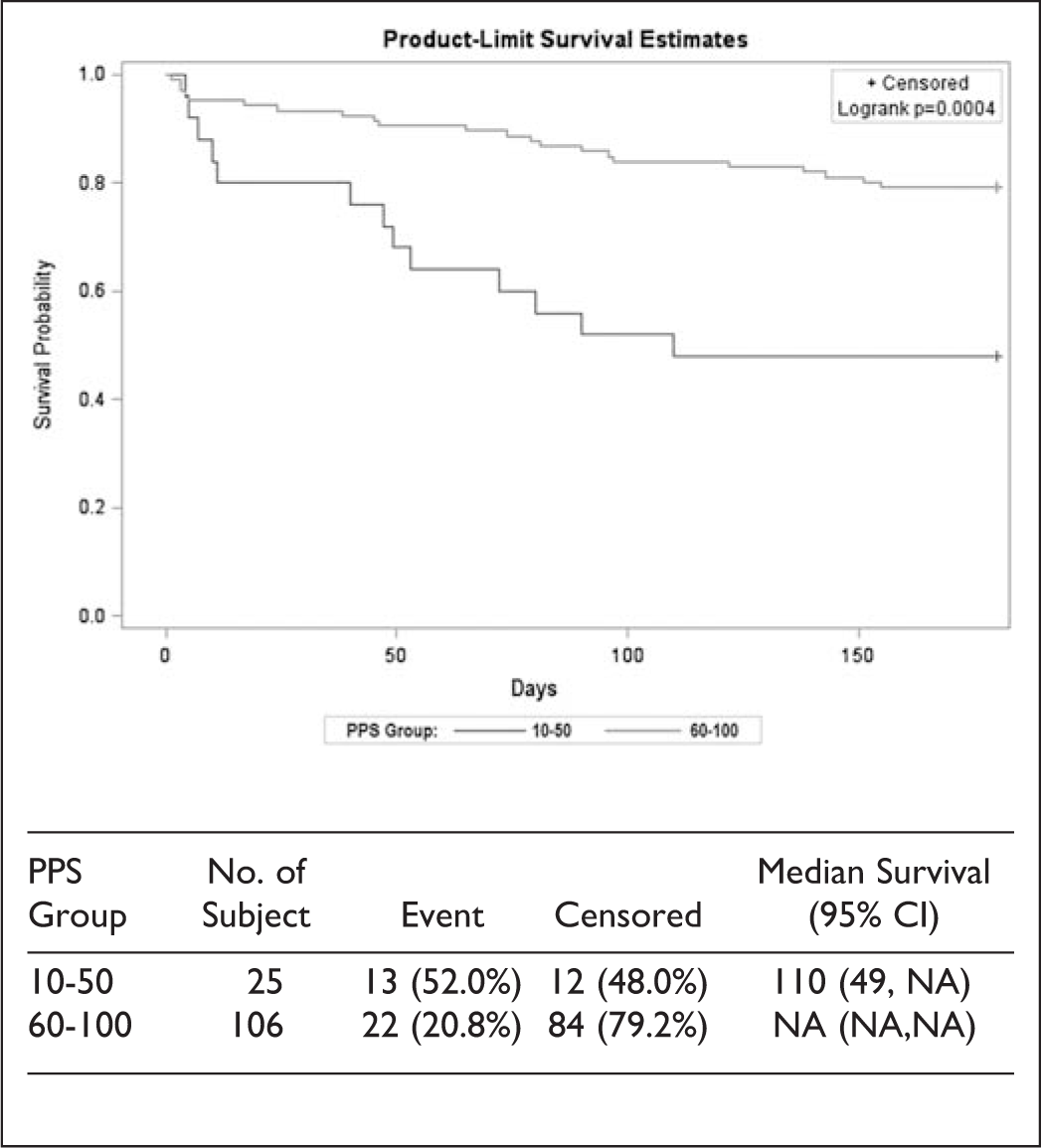
Kaplan-Meier plot by PPS group.
Survival Analysis Model Results (PPS as Primary Covariate).
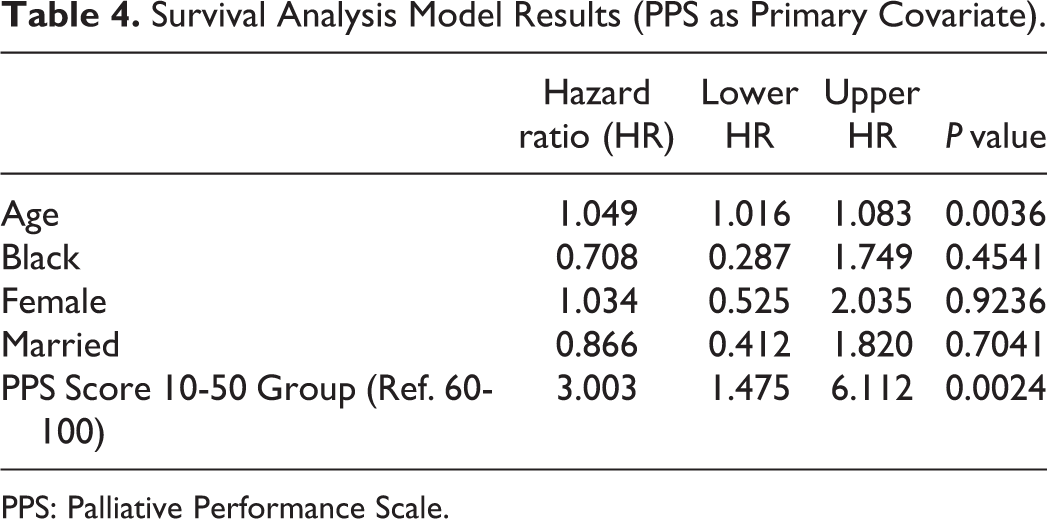
PPS: Palliative Performance Scale.
Discussion
Our findings demonstrate that lower baseline PPS scores are predictive of death within 6 months, which is in agreement with prior studies of this clinical setting. 14,15 Specifically our data suggest that patients who, at most, mainly sit or lie and are unable to do any work at baseline (PPS ≤50) are 3 times more likely to die within 6 months compared to those less debilitated. Similarly, patients meeting criteria for inpatient palliative care consultation based on the P-CaRES tool were 4 times more likely to die within 6 months compared to those not meeting criteria. The median survival for patients with a baseline PPS of 50 or less was 110 days and 122 days for those who were P-CaRES positive. Increasing age independently predicted 6 month mortality, but there were no differences in PPS groups by race, gender, marital status.
The prior studies of PPS for prognostication of ED patients had limited generalizability because of racial homogeneity. 14,15 A benefit of our study was that it was conducted at an urban academic medical center where the rate of black participants more closely mirrored the state percentages than Babcock et al. (27.5% vs 29.7% in SC compared to 4.9% vs 12.0% in CT) 14 This point is noteworthy because minorities have been shown to have lower quality care near the end of life in regard to pain management and satisfaction with care and clinician communication. 16
Baseline PPS and P-CaRES status were too closely correlated to be able to evaluate their utility in predicting survival in combination compared to either measure individually. Nevertheless, our demonstration that the P-CaRES tool and PPS are highly correlated in their prediction of 6 month survival supports the concurrent validity of P-CaRES tool prognostication with that of the previously validated PPS. We found that they are both helpful in identifying those at increased risk of dying within 6 months, but they have their own utility. P-CaRES is validated for identifying those patients with pre-existing conditions who have significant unmet palliative care needs and thus may facilitate ED clinicians to initiate primary or specialty palliative care. Our study now demonstrates that those patients screened positive by P-CaRES have decreased survival, a fact that may facilitate goals of care conversation. Future studies could expand the concurrent prognostic validity of P-CaRES by combining assessment with disease specific prognostic tools (FAST scale in dementia patients, GO-FAR tool for in-hospital cardiac arrest).
While the PPS cannot identify specific unmet needs, it does have the advantage of being a more rapid assessment tool and ED clinicians may consider using the PPS scale alone to aid in their prognostication based on our findings. To further simplify the categorization of those patients with a PPS of 50 or less, this group may be identified by a single question of the following, “At baseline, do you normally sit or lie down during the day, and are unable to do any kind of work?” Furthermore, in other settings a PPS of 10 has been shown to predict survival to just several days 13 and thus may have more specificity in identifying those who might benefit from direct referral to hospice and forego admission. Future studies are needed to further evaluate this method of assessment.
Limitations
Limitations of the current study are that it only includes a single site and enrollment occurred over a 6-week period and thus is subject to site specific and time of year bias, respectively. In addition, 3 different co-investigators collected data and there was no assessment of intra-rater reliabilit
Conclusions
In addition to identifying patients with unmet palliative care needs who might benefit from an inpatient palliative care consultation, the P-CaRES tool can predict 6 month survival and is highly correlated with prognostication using the PPS. Future randomized clinical trials of P-CaRES tool implementation with larger sample size are needed to confirm the findings of our prospective cohort.
Footnotes
Authors’ Note
The views expressed in this manuscript are the authors alone and not an official position of the authors’ respective institutions. Preliminary findings were presented by S. DeWitt as a poster presentation at the American Academy of Hospice and Palliative Medicine Annual Assembly in Orlando, Florida, from March 13-16, 2019.
Acknowledgments
The authors thank Patrick Maudlin, PhD, and Jingwen Zhang, MS, for their statistical support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.