
Abstract
End of life discussions frequently take place in surgical intensive care units, as a significant number of patients die while admitted to the hospital, and surgery is common during the last month of life. Multiple barriers exist to the initiation of these conversations, including: miscommunication between clinicians and surrogates, a paternalistic approach to surgical patients, and perhaps, conflicts of interest as an unwanted consequence of surgical quality reporting. Goal discordant care refers to the care that is provided to a patient that is incapacitated and that is not concordant to his/her wishes. This is a largely unrecognized medical error with devastating consequences, including inappropriate prolongation of life and non-beneficial therapy utilization. Importantly, hospice and palliative care needs to be recognized as quality care in order to deter the incentives that might persuade clinicians from offering these services.
Keywords
Introduction
A substantial amount of the deaths (29-39%) in the United States occur in a hospital, albeit an increasing trend of terminally ill people choosing to die at home, has been observed in the last decade. 1 Surgical care is common at the end of life, particularly in hospitalized patients. It is estimated that approximately 20% of patients undergo an operation during their last month of life. 2,3 Most people that die in an intensive care unit, do so after a decision has been made to limit life-supporting therapies. 4 These statistics underscore the importance of end-of-life (EOL) conversations between clinicians, patients and family members, that often occur in surgical intensive care units (SICU). Communication with patients in a SICU represent a special challenge, as commonly their ability to speak is diminished due to their illness or sedation. In this state, patients are incapacitated from expressing their wishes. Ideally, a document that describes in detail the wishes of the patient should be easily available (advance directive). However, it is known that there is a low prevalence of documented wishes of patients that are critically ill, 5 and that their utility is limited. 6 Consequently, clinicians often have to rely on surrogates to act as decision makers. This situation can lead to conflict between the patients’ surrogates, between surrogates and clinicians, and among clinicians themselves, further complicating EOL care.
Despite the importance of EOL care, medical literature only scarcely covers the topic, it constitutes only about 2% of the content of major medical specialty textbooks. 7,8 Notably, surgical books are among the most deficient. Concerningly, surgical patients are less likely to be offered palliative, and hospice care in comparison to medical patients in the last year of life. 9 Physicians in-training have also reported deficiencies in end-of-life care education during their critical care rotations, particularly in regard to the withdrawal of life sustaining therapies. 10 This can lead to overreliance on palliative care services to conduct these conversations, which is problematic since these services are a limited resource with projected shortages. 11,12 Subsequently, every clinician that cares for patients in the SICU should be familiar, and comfortable with EOL conversations.
Multiple barriers exist that impede the initiation of EOL conversations in the SICU, including: a paternalistic approach to surgical patients, deficits in communication, unresolved conflictive views between clinicians and between clinicians and families, and conflicts of interest that may arise as an unintended consequence of quality reporting. Inadequate EOL discussions can result in goal discordant care. This article introduces goal discordant care as a medical error with important consequences. Subsequently, it reviews the historical transition of the decision-making role from the physician to the patient. Lastly, it focuses on the barriers to high quality end of life care, which include: paternalism in surgical intensive care and the potential of deleterious effects of quality reporting.
Goal Discordant Care
Definition
Goal discordant care (GDC) is a medical error, 13 caused by a disagreement between the patient’s ultimate goals of care and the goals pursued by their health care providers. It is the result of multiple faults that occur simultaneously creating a chain of events that results in the adverse outcome. 14 This disagreement can have devastating consequences in EOL care. Such consequences are: inappropriate prolongation of life, unnecessary pain and distress, and increased healthcare costs. 15 Unnecessary, or non-beneficial therapies are unfortunately common at the end of life. It is estimated that during the last 6 months of life, up to 38% of the therapies that patients receive are considered non-beneficial. 15 The exact prevalence of GDC in surgical patients is unknown, and needs to be determined, an enterprise that is complicated by the lack of a standard method to measure patient-provider goals of care concordance. 16
Contributing Factors
Alike other medical errors, miscommunication is the primary cause of goal discordant care at the end of life. 17 The most reliable source of information regarding a patient’s wishes are the patients themselves, or an advance directive in case that the patient is incapacitated. Every patient that presents to the hospital for an operation should be asked if they have documented advance directives, and provided written information regarding how to arrange for them if they do not have them. This is a mandatory requirement for hospitals that care for patients that participate in Medicare, according to the Self Determination act. 18,19 Nevertheless, only between 13%-17% of patients undergoing high risk surgery (defined as > 1% mortality), have their wishes documented in the chart. 20,21 Notably, advance directives have several limitations, and the ability of this strategy alone to prevent GDC has been questioned, and not supported by high quality of evidence. 6 This is likely due to the difficulty of discussing and documenting complex decisions in advance, which is particularly challenging in the pre-operative setting. When an advance directive exists, it should be reviewed and included in the pre-operative conversation.
In the absence of a documented advance directive, clinicians have to rely on surrogates that know the patient well, and that are therefore in a position to voice their wishes. Family members usually serve that role. Regrettably, the communication between clinicians and families in the ICU is known to be suboptimal. 22 Table 1, provides a list of barriers that are known to complicate communication between clinicians and families, and that can complicate EOL conversations.
Barriers to Communication in the Surgical Intensive Care Unit, Adapted From. 23,a
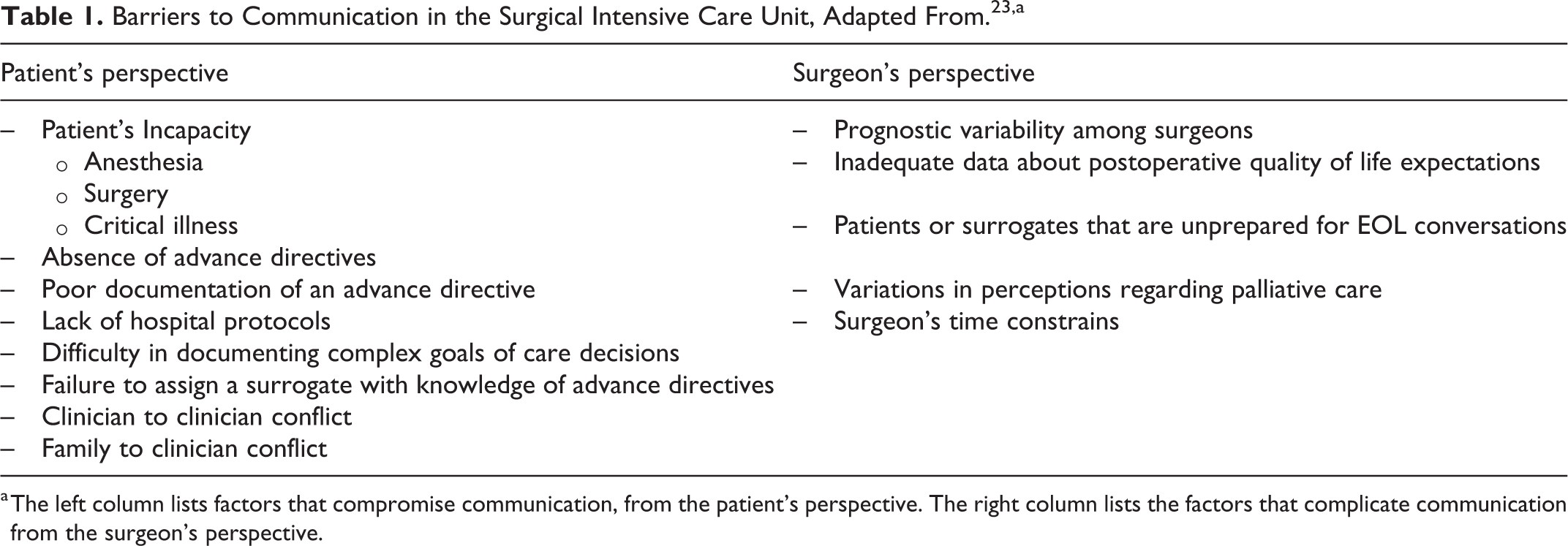
a The left column lists factors that compromise communication, from the patient’s perspective. The right column lists the factors that complicate communication from the surgeon’s perspective.
Prevention
Different efforts have been developed to improve communication between clinicians and families at the EOL. 3,24,25 Yet, the most important intervention is to have a preoperative conversation with patients that are considered high risk, and/or that will undergo a high risk surgery. This conversation should include the patient’s wishes regarding life-support if it becomes necessary. Patients can have different opinions regarding different therapies, so each should be discussed individually. Importantly, an assigned proxy should be identified and also documented. Clear and easily discoverable documentation of the conversation is imperative. In cases were an advance directive already exists, it should be reviewed and adapted to the context of the individual surgical intervention. This is important, as patients have reported not discussing their expressed wishes with their surgeons, but assuming instead that their wishes will be followed. 26 Even a brief preoperative discussion about goals of care led by an anesthesiologist, has shown to increase patient-proxy discussions regarding EOL wishes, and assignment of power of attorney. 27 Early involvement of a palliative care team should be considered in patients with terminal organ failure, to improve the quality of life initially and to facilitate EOL care. 28 Institutions should establish protocols that enhance proactive communication and early expert consultation. 29
Occasionally, clinicians that have a longitudinal relationship with a patient (e.g. a surgeon that has followed the patient for months), can have a different viewpoint from clinicians that have single phase patient relationships (e.g. SICU team). 24 This can result in conflicts that can, in turn, lead to GDC. Facilitators of communication between clinicians are: the development of established protocols, and the presence of surrogates that are well informed. 24 If necessary a hospital ethics committee can be consulted to help mediate the conflict. Similarly, when clinician to family conflict arises, it is essential to consult the ethics team early on. Figure 1 includes a management algorithm for EOL discussions in high risk surgical patients.
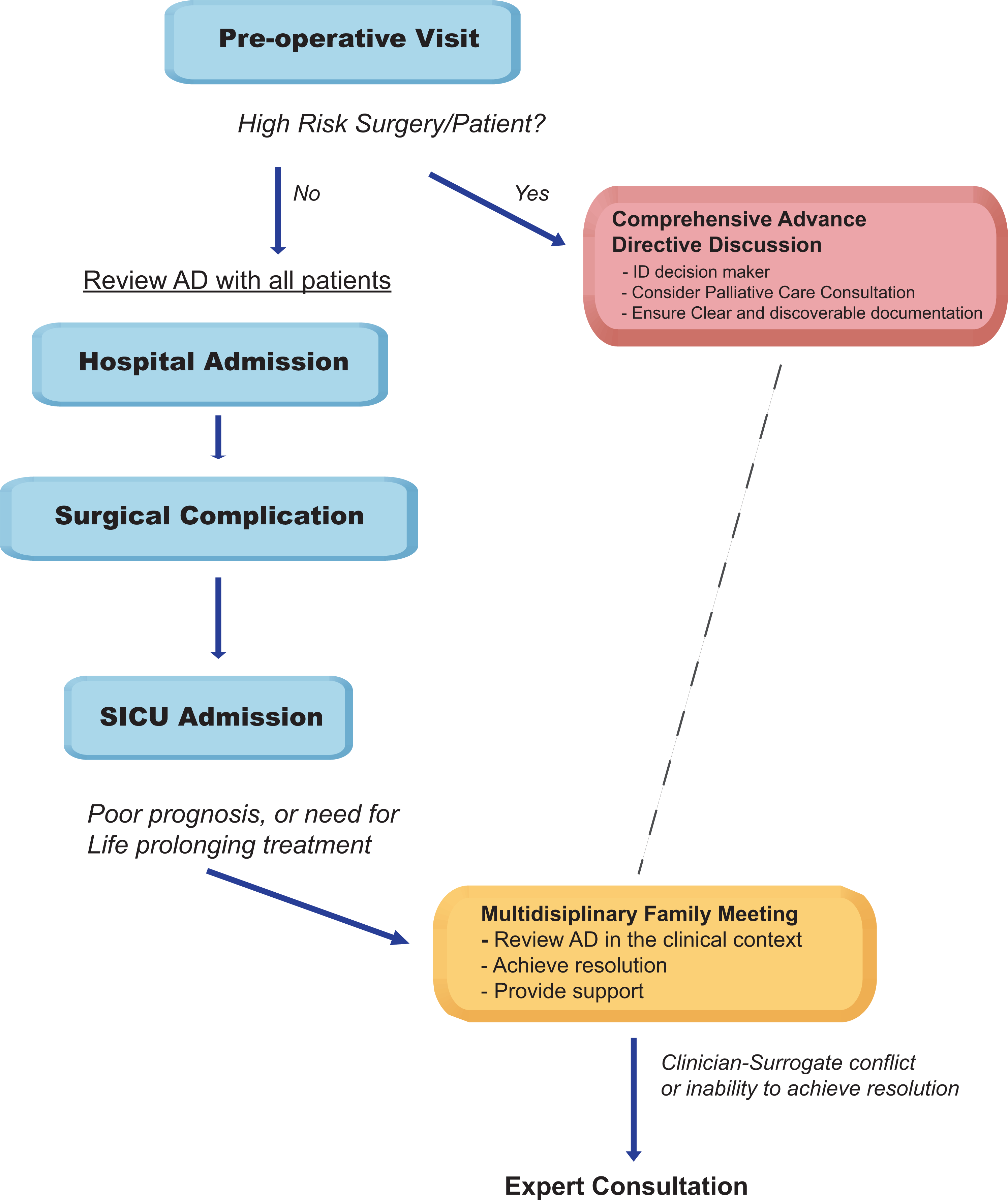
Algorithm for End of Life discussions in high risk surgical patients undergoing high risk surgical procedures. Once a patient or surgery is identified as high risk for death or for dependence on life support, a comprehensive conversation should be initiated. Ideally this conversation should be led by an independent party (e.g. palliative care provider). The goal of this conversation is to clarify advance directives, code status, and to identify a surrogate decision-maker. If a surgical complication deems the patient incapable of making decisions and the condition that he/she is in requires life support then a family meeting should be called to review the documented wishes and provide support. A resolution should be obtained an enacted. If unresolved conflict arises, expert consultation by an ethics committee is advised.
Evolution From Paternalism to Autonomy
The assignment of the authority figure that acts as patient-decision maker has evolved over time. In an earlier paternalistic approach, the physician used to dictate all decisions regarding the care of patients, this is evident in an extract from the American Medical Association code of ethics from 1847: “The obedience of a patient to the prescriptions of his physician should be prompt and implicit. He should never permit his own crude opinions as to their fitness, to influence his attention to them. A failure in one particular may render an otherwise judicious treatment dangerous, and even fatal.” The contemporary approach to patient-care is based in the principle of autonomy, in which patients, or surrogates (if the patient is incapacitated), are the ultimate decision-makers. 30 Correspondingly, the updated statement from the American Medical Association code of ethics reflects that principle: “A patient who has decision-making capacity may accept or refuse any recommended medical intervention.”
Today it is standard practice to engage in detailed descriptions of the discrete risks of surgical interventions with patients before surgery. However, specific discussions regarding treatment limitations in the case of a postoperative complication are often lacking. 26 This often leads to assumptions in regard to the extent of life sustaining therapies that the patient would agree to if asked specifically. The assumption that, patients that agree to surgery are also agreeing to all postoperative life-sustaining therapies, is prevalent in “buy-in” contracts. Buy-in contract is a loose term that describes an informal commitment, between a surgeon and a patient who is agreeing to a high risk surgery. 31,32 It comprises a conversation in which the patient is asked to agree to a “packet deal” that includes all postoperative care to continue for a certain period of time. 31 Notably, this agreement is often not clearly documented in the patient’s chart. Buy-in contracts, are common practice. In a national survey of cardiothoracic, vascular and neurological surgeons, 62% of respondents specified that they include a buy-in contract in their practice, 32 although this percentage could have been inflated by non-respondent bias. Two possible deleterious consequences of these contracts are: 1. The reluctance to offer surgery if the patient does not agree to the “packet-deal,” and 2. the reluctance from the surgeon to agree to withhold or withdraw life support in the postoperative period. 32,33 The latter can lead to inappropriate prolongation of life. This reluctance seems to be inversely correlated to the time that has passed after the surgery, and can occur even when patients or surrogates ask for the therapies to be withdrawn. 32 Surgical buy-ins should be considered overtly paternalistic, and therefore outdated. A better alternative to buy-in contracts is a pre-operative discussion, that is well documented in the chart, and that includes the possibility of the need for life supporting therapies. During these discussion the clinician should act, not as an authority figure, but as a source of information based on his knowledge and expertise that guides the patient to make an informed decision, a shared decision. 34,35
Autonomy, also has its limits, as patients and surrogates have the right to defer decision-making authority to clinicians in the ICU if they choose to do so. In fact up to 20% of surrogates decide to defer this authority to ICU physicians. 36 However, since only the minority of surrogates choose this route, this transfer of authority should never be assumed. Patients and surrogates should always be informed, and given the opportunity to participate in the decision making process.
Inappropriate Prolongation of Life as a Consequence of Quality Reporting
Surgical Mortality Reporting as a Performance Metric
The Center for Medicare and Medicaid Services (CMS) is the largest health care payer in the United States. Other insurance programs often follow CMS guidelines. Significant changes have occurred during the last 5 years in the CMS reimbursement model. One of the most notable changes is the Medicare Access and CHIP Reauthorization Act (MACRA), that was signed into law in 2015 with bipartisan support. This legislation replaced the Medicare sustainable growth rate (SGR), with the Quality Payment Program (QPP). This change was intended to shift reimbursement incentives from a volume-based, to a quality-based model. Quality care is defined by the institute of medicine as: “The degree to which health care service for individuals and for populations increase the likelihood of desired healthcare outcomes and are consistent with current professional knowledge.” 37 The “desired health care outcomes” are considered therapeutic by insurance providers in most circumstances. However, at the end of life it is conceivable that patients might opt for palliative care instead. Notably, palliative and hospice care quality metrics are not established yet, and this might impair the consideration of this therapies as “quality care,” particularly in regard to reimbursements. A consequence of this, is that procedures are valued over palliation of symptoms in terminally ill patients. In fact, Medicare reimbursements incentivize in-hospital procedures in place of other supportive care for patients at the end of life. 38
The QPP has 2 tracks to choose from: the merit-based incentive payment system (MIPS) and an advanced Alternative Payment Models (APMs). Currently most providers fall into MIPS. In this system physicians generate a report that includes specific quality metrics, and this generates a MIPS score. Based on the MIPS score penalties are given to half of the physicians with substandard scores, and rewards to the half of the physicians with positive scores. 39 Risk adjusted 30-day operative mortality is an important MIPS clinical quality measure. While it is clear that mortality is an undesirable health care outcome, there are growing concerns of unintended consequences of reporting mortality as a quality metric. The most consequential unintended consequence is the reluctance by physicians to initiate EOL discussions to avoid penalties, which can lead to inappropriate prolongation of life.
Reporting of 1 Year Transplant Mortality
In order to maintain program certification from CMS, transplant centers have been required to report quality metrics and have been expected to meet performance thresholds. 40 Failure to meet these metrics has led to severe consequences including the closure of programs, and halting of certain type of organ transplants, in which graft or patient survival are below expectations. 40 A program is deemed not-compliant when the number of patient deaths or graft failures within 1 year of transplant, exceeds 150% of the risk-adjusted expected number. CMS utilizes data from the Scientific Registry of Transplant Recipient post-transplant (SRTR), a required public-access registry with epidemiological and statistical data related to solid organ transplants outcomes. 41,42 The registry utilizes a simple scoring system intended to facilitate understanding of the data by patients and their families. Post-transplant outcomes have traditionally included patient and graft survival 1 year after surgery. Similar to the postoperative 30-day mortality quality metric, concerns exist that this quality reporting provides an incentive to prolong life inappropriately, to avoid penalties. Interestingly, this reporting system might undergo drastic changes in the near future due to a recent legislation. The Omnibus Burden Reduction rule, 43 includes a statue that will likely exempt transplant programs from the condition of reporting outcomes to maintain certification. However, the ruling states that Medicare will continue to monitor quality data, and that SRTR will still be publicly reported. The implications of this change of legislation in the 1-year mortality metric are unclear to date.
Unintended Consequences of Quality Reporting
Mandatory reporting of 30-day mortality potentially produces an incentive to withhold EOL conversations until the 30-day mark. This troublesome consequence gained national interest in 2015, when a case was reported in the media. 44 In that case, EOL discussions were inappropriately delayed in an elderly patient that had undergone surgery and was terminally ill, until the 30th day had passed. This was reportedly done with the intent of avoiding a negative mortality report. To date, 2 large studies have been conducted to address this issue. In a retrospective, cohort study conducted from 2008-2015 in Massachusetts and New York, the mortality daily hazard was followed in patients that had undergone a coronary artery bypass graft. 45 No increase in the daily hazard was observed immediately after the 30-day mark in either state, suggesting that no delays in withdrawal of life-sustaining therapies happened as an unintended consequence of mortality reporting. A larger study that included 19 types of major surgery and utilized Medicare data from 2011 to 2013, also did not find an increase in daily hazard of mortality at the 30 day mark. 46 Consequently, although to date there is no evidence to support 30-day quality reporting as causing inappropriate prolongation of life, these findings have to be interpreted with caution. The studies were designed to detect only an abrupt change in mortality after 30 days, and therefore they do not necessarily rule out inappropriate prolongation of life if this did not happened in an abrupt manner. Also, it is important to notice that they pre-date the passing of MACRA, with its rollout of increasing financial penalties linked to quality reporting that occurred from the year 2015 to the year 2019. It will be important to conduct updated studies, that directly address the issue of inappropriate prolongation of life in postoperative patients.
Solid organ transplant centers in the United States have been under significant pressure to report favorable quality metrics, of which, the 1-year-mortality is the most consequential. Inappropriate prolongation of life in order to meet a positive metric is also a potential consequence of this measure, and anecdotal reports have also been reported in transplant recipients. In a recent article in the media, 47 a case of inappropriate prolongation of life was described in a transplant recipient. This case detailed the alleged conversations of a multidisciplinary transplant team that decided to delay EOL conversations with the family of a patient that was in a vegetative state, until the 1 year mark. These revelations were met with shock by the family, and have triggered an investigation by the state of New Jersey. To address the issue of inappropriate prolongation of life in transplant patients, a large study has evaluated short-term mortality before and after the year mark after solid organ transplantation. 23 Although no significant difference in mortality was found in heart and liver recipients, there was an unexpected increase in the risk of mortality during the 30 days after 1 year in lung transplant recipients. This is a concerning finding that needs further attention. As it is the case in the 2 studies that addressed surgical mortality at the 30 day mark, this study design also lacks the ability to detect inappropriate prolongation of life that is not linked with an abrupt action at the 1 year mark, and thus other studies are warranted. Whether the new omnibus bill will eradicate any incentive for inappropriate life prolongation is yet to be determined.
Inappropriate prolongation of life is also a potential consequence of public reporting of mortality in itself. Public physician-performance reporting started in the 1990s in New York in an effort to reduce the mortality after CABG surgery. 48 This initiative is generally regarded as having a positive effect in quality and outcomes. 49 Understandingly, the public release of surgeon-specific mortality has been met unfavorably by surgeons and hospitals alike, due to concerns of misinterpretation of the data by the public. 50 About 50% of surgeons that perform high risk surgeries, have expressed concern about the emphasis on outcome measures and physician profiling in a national survey. 32 Neither clinicians or programs should be penalized or disincentivized from offering goals of care that deviate from therapeutics. Palliative and hospice care need to be recognized as quality care. In regard to this effort, a multi-society effort has initiated the development of benchmarks to define quality measures in the practice of palliative and hospice care. 51 This is a first step toward the development of quality measures that are specific to care at the EOL.
Conclusions
Clinicians that provide care in surgical intensive care units should be comfortable initiating and facilitating end of life conversations for patients whenever it is appropriate. Paternalism is still present in the care of these patients through buy-in contracts, and by behaviors that limit patient’s autonomy, with potentially devastating consequences. One of these consequences is goal discordant care, a medical error that is the result of miscommunication between patients and providers. Improvement in communication between clinicians, patients and family members is warranted and can be achieved through clinician education and institutional protocol implementation. Inappropriate prolongation of life is a potential consequence of surgical mortality reporting. To date, evidence of this occurrence is mainly anecdotal. Palliative and hospice care need to be recognized as quality care by clinicians, and by government agencies to eliminate the incentive to inappropriately prolong life.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.