
Abstract
Background:
Given the lack of empiric recommendations for vascular access for palliative chemotherapy, we aimed to analyze survival and complications after placement of central venous access ports for palliative chemotherapy.
Methods:
We performed a retrospective chart review of 135 patients undergoing port placement for palliative chemotherapy at a single institution from January 2015 – July 2020.
Results:
The median age was 68 (range 47-91). Median overall survival was 7.7 months (95% CI, 6.5-8.9 months). The rate of port-related complications was 11.1% (15 of 135). Patients who developed port-related complications required corrective surgery in 73.3% (11 of 15) of cases. Results were similar among all patients, regardless of their primary diagnoses or central venous access sites.
Conclusions:
Increased awareness about the limited survival of patients after port placement for palliative chemotherapy, and their significant complication risk could be used to help patients and their providers make value-aligned decisions about vascular access.
Keywords
Introduction
Centrally inserted totally implanted vascular access ports and peripherally inserted central catheters (PICCs) are the most commonly used central venous devices for the administration of chemotherapy.
PICCs can be left in place for weeks or months. They are easily inserted and removed but must be kept dry at all times and require cleaning and maintenance flushing at least once a week. Because they can be placed quickly by specially trained nurses outside the operating room, PICCs have the advantage of avoiding delays in chemotherapy administration and reducing procedural costs. 1 On the other hand, the insertion and removal of ports is invasive and thus carries the risk for serious procedural complications such as arterial or thoracic duct injury, pneumo/hemothorax, or cardiac tamponade, which may require additional surgical interventions. 2 However, ports require less maintenance (only once-a-month flushing), can remain in place for months or years, and may lead to higher patient satisfaction. 3
Studies comparing cost analysis of PICCs vs. ports have produced inconsistent results, reflecting healthcare system and institutional differences in costs associated with device implantation, maintenance, complications, and removal.4-6 However, implantation costs for ports are consistently reported to be higher than those of PICCs.3,5,7
Some studies have shown a higher rate of complications (especially catheter-associated thrombosis) among patients receiving chemotherapy via PICCs versus ports. 4 , 8 However, there is insufficient evidence to routinely recommend a specific type of vascular device for all cancer patients. As a result, both the European Society of Medical Oncology and the American Society of Clinical Oncology do not recommend one device over the other for the administration of adjuvant chemotherapy.9,10 Furthermore, guidelines suggest that there is no clear preference between PICCs and ports when the proposed duration of therapy is longer than 1 month.11,12
Empirically in many institutions, for long term use (>6 months) a port is usually preferred, whereas for short-term chemotherapy treatments (<6 weeks) a PICC line is used.
While deciding which device should be used for cancer patients receiving curative chemotherapy is important, the choice between PICCs and ports has an even greater significance for oncologic patients undergoing palliative chemotherapy. While palliative chemotherapy is focused on prolonging life and promoting the quality of life, 13 there is also evidence suggesting that terminal cancer patients who receive palliative chemotherapy are more likely to undergo invasive medical procedures during the last months of life and are less likely to die where they wish. 14
The purpose of this study was to retrospectively analyze the survival of cancer patients following placement of ports for palliative chemotherapy and their port-related complications. We hope to provide important findings that could help avoid unnecessary risks for terminal cancer patients and facilitate more informed, patient-centered decisions when selecting the adequate vascular access device for palliative chemotherapy.
Methods
After institutional review board approval, we conducted a retrospective review of electronic medical records of all patients who underwent palliative port placement at our institution over a 5-year period (January 2015 – July 2020).
We identified patient demographics, indications for the surgery, and intra-operative and post-operative complications. Patient information and the name of the surgeon performing the procedure were anonymized before the data were analyzed.
Overall survival was measured from the time of port placement to the time of death and, for patients who did not die, was censored at the time of our chart review. The distribution of the overall survival was estimated by the Kaplan-Meier method. 15 The log-rank test was performed to test the difference in survival between groups. 6
Data analysis was performed from October 10-18, 2020. Statistical significance was set at P < 0.05. All analyses were conducted using SAS software, version 9.4 (SAS Institute Inc).
Results
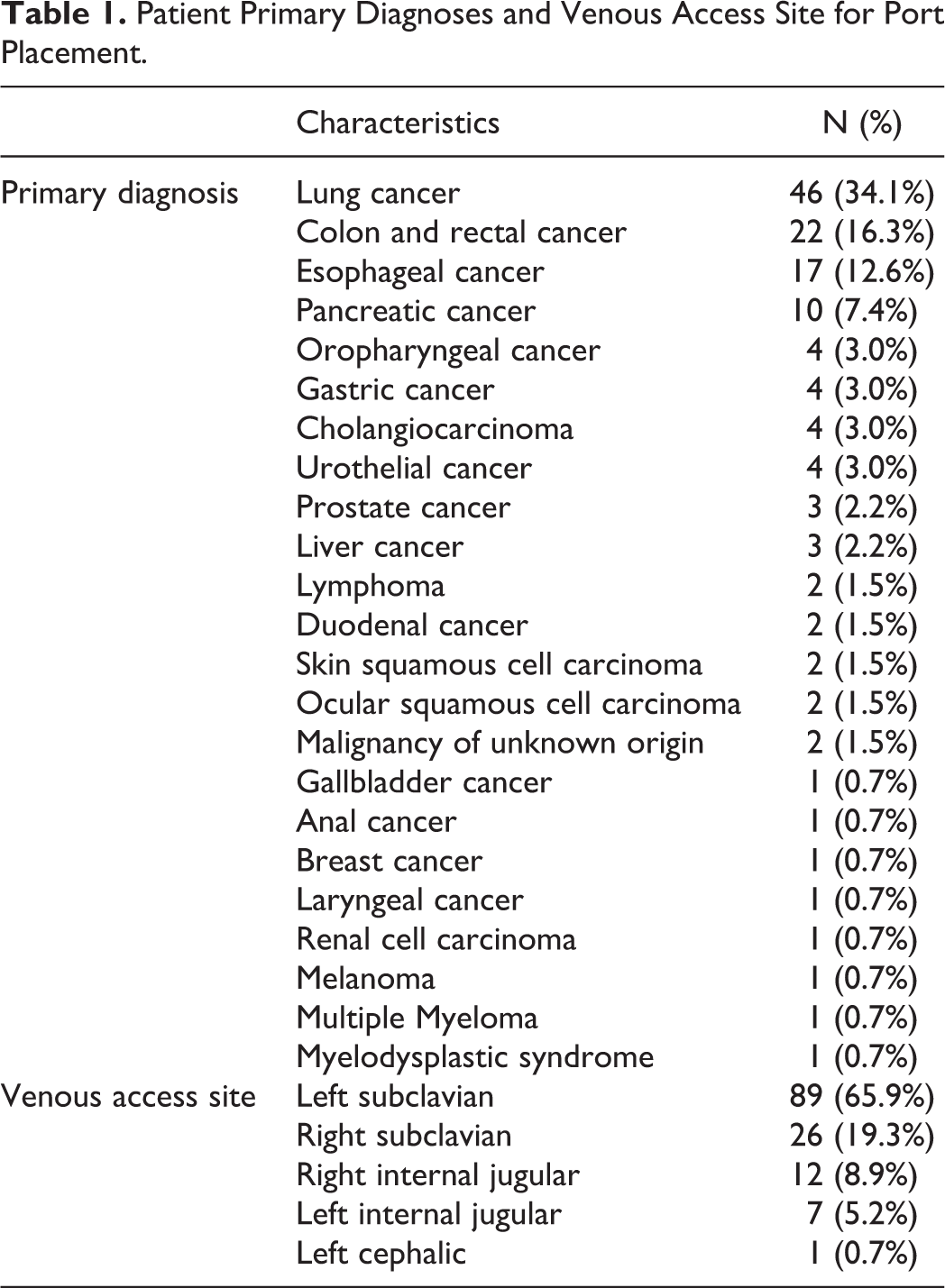
Between January 2015 and July 2020, 135 patients underwent palliative port placement under fluoroscopic guidance at the VA Boston Healthcare System. The median (range) age of patients at the time of the operation was 68 (47-91) years. Most patients were male (132 [97.8%]), consistent with the patient demographics at our institution. Patient primary diagnoses and central venous access sites for port placement are shown in Table 1. The most common diagnosis was lung cancer (n = 46, 34.1%). Port placement was most often performed by accessing the left subclavian vein (n = 89, 65.9%).
Patient Primary Diagnoses and Venous Access Site for Port Placement.
The survival rates following palliative port placement are shown in Figure 1. Median overall survival was 7.7 months (95% CI, 6.5-8.9 months) for the entire patient cohort; 4.8 months (95% CI, 1-8.6 months) in pancreatic cancer patients; 7.3 months (95% CI, 4.5-10.1 months) in lung cancer patients; 8.8 months (95% CI, 6.3-11.3 months) in esophageal cancer patients; and 10.8 months (95% CI, 6.9-14.7 months) in colorectal cancer patients.
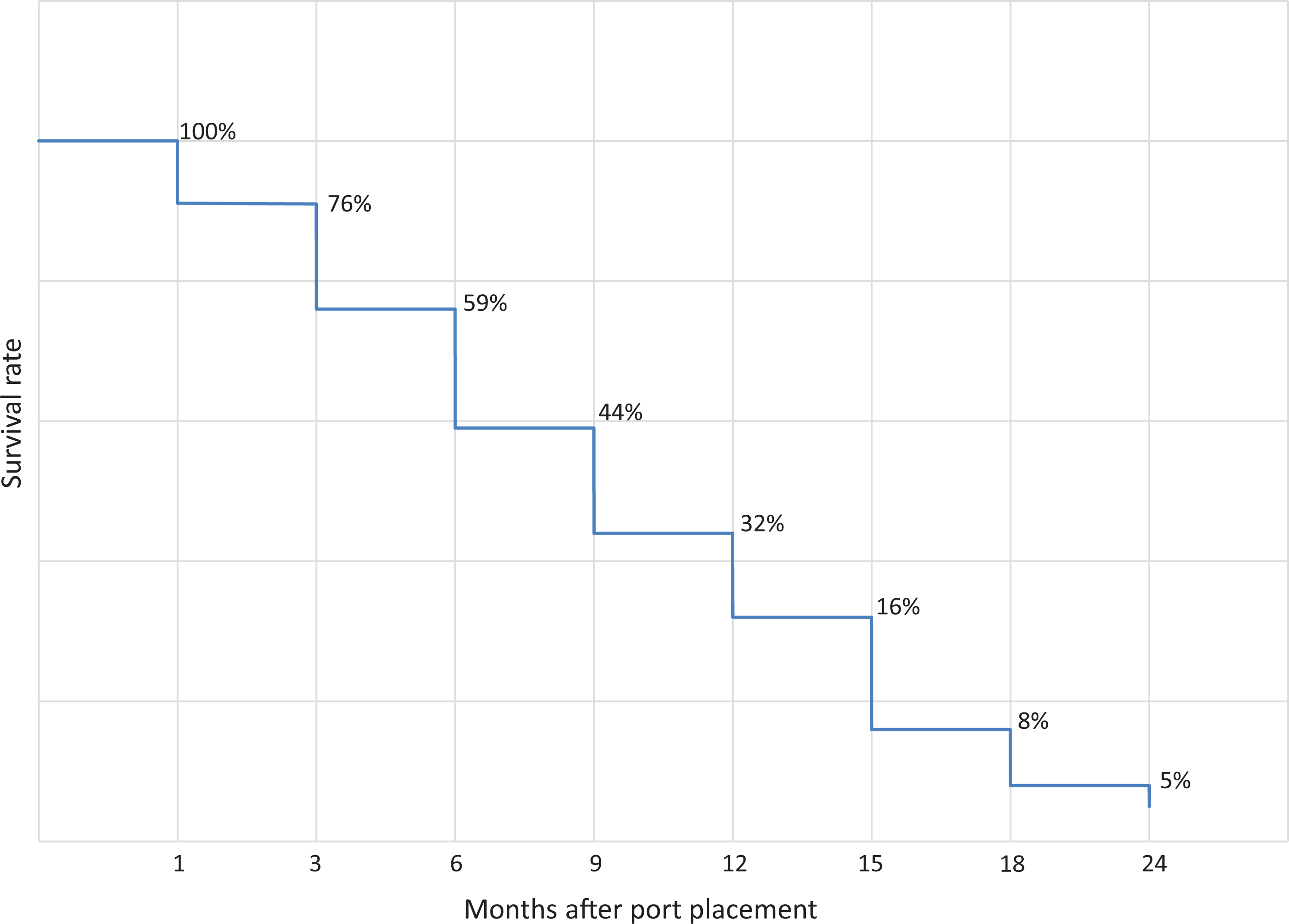
Survival Curve of Patients Following Port Placement for Palliative Chemotherapy.
The median overall survival was statistically similar (P > 0.05) among all patient primary diagnoses and central venous access sites for port placement. No autopsy examinations were performed on any of the patients who died.
The complications that occurred following port placement are listed in Table 2. The overall rate of port-related complications was 11.1% (15 of 135). Intra-operative complications occurred in 4 (3.0%) patients and consisted in technical difficulties resulting in attempted cannulation of multiple venous access sites in 3 patients. One patient suffered a right subclavian artery perforation requiring median sternotomy for repair and abortion of port placement.
Port-Related Complications.
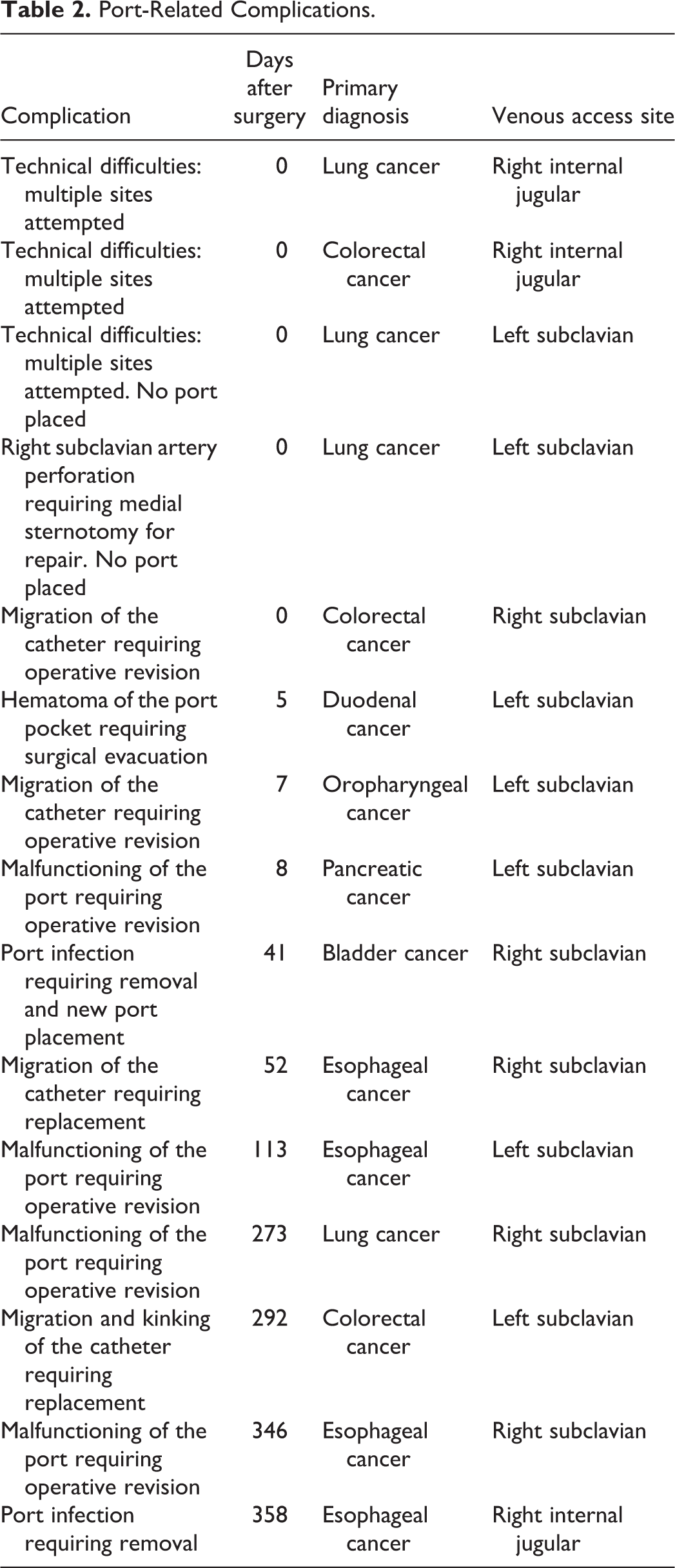
Eleven patients (8.1%) developed post-operative complications that included malfunctioning of the port requiring operative revision, 4 migration and/or kinking of the catheter requiring operative revision, 4 port infection requiring removal, 2 and hematoma of the port pocket requiring surgical evacuation. 1 Overall, patients who developed port-related complications required corrective surgery in 73.3% (11 of 15) of cases.
Discussion
To our knowledge, this is the first study to assess survival and complications after port placement for palliative chemotherapy. We demonstrate a median survival time after port placement of just over 6 months with no significant differences in survival time by diagnosis. Over 10% of patients suffered port related complications that required corrective surgery in over 70% of cases. This information can be used to help patients undergoing palliative chemotherapy and their providers make value-aligned decisions about vascular access.
PICCs and ports are the most common types of venous access for cancer patients undergoing chemotherapy. In patients who are undergoing long-term chemotherapy or for early stage disease, having durable and long-term access is a priority; therefore, port is widely agreed upon as a safer and less expensive option. 16 Though ports require a surgical procedure including anesthesia, they are longer-lasting, lower maintenance, tend to bother patients less, and are associated with lower incidence of catheter-related deep venous thrombosis.3,17,18 Importantly, the port-related complications in our study required corrective surgery in the majority of cases. PICC is a less invasive option that is generally optimal for treatments lasting 6 months or less. 19 The median survival in our study was just over 6 months, which suggests that PICC could be a less invasive and preferable option in many patients receiving palliative chemotherapy . Though our study was likely underpowered to demonstrate a statistically significant difference in survival by diagnosis, there was a non-significant trend toward poorer survival in pancreatic and lung cancer patients (4.8 months and 7.3 months, respectively) after port placement for palliative chemotherapy. These subgroups of patients may be better served by PICCs rather than ports.
Deciding on access for palliative chemotherapy should be a preference-sensitive decision, particularly because there are no empiric recommendations. When the intent of chemotherapy is palliative, it lacks survival benefit and is administered for the purpose of reducing tumor burden and decreasing symptoms.13,20 For this reason, providers should consider the invasiveness of the access and the risk of complications weighed against the prognosis. In our study, the mean survival time was just over 6 months, but many of these patients were not likely receiving chemotherapy until the day they died, so may have needed venous access for less than 6 months. This is supported by evidence suggesting that, while PICCs are removed immediately after completion of chemotherapy, there is a tendency for ports to be left in situ afterward. 17 This subset of our patients may have been better served with less invasive PICCs, particularly when accounting for the significant rate of port-related complications and subsequent corrective surgeries. PICCs for this group of patients would also be more cost-efficient than ports, because evidence suggests that when vascular access devices are used for less than a year, costs are lower with PICCs. 3
Our study has several limitations that must be highlighted. First, while our study benefits from being the first of its kind, it was performed at a single institution. While single-center studies are important in generating hypotheses and are widely used in oncologic research, their most obvious disadvantage is a potential limitation in its external validity. Some unique institutional aspects that might reduce the generalizability of our findings to a broader population could include patient age, gender, and comorbidities; surgeon considerations regarding the logistics of timely port insertion; operative technique for port placement; and institutional culture of end-of-life care.
Second, as a retrospective review of electronic medical records, our study is prone to recall bias, misclassification bias, and confounding risk factors that may be present but were not measured.
Third, our study included patients with a wide range of cancers receiving palliative chemotherapy. Because of the small sample sizes of subgroups within our cohort, interpretation of the results with regard to specific oncologic diagnoses is limited. Studies with larger sample size would allow more precise stratification analysis to determine which cancer patients would benefit from port placement for their palliative chemotherapy.
Fourth, by only analyzing overall survival and complications in patients undergoing port placement for palliative chemotherapy, we are not able to make comparisons with patients using PICCs for their palliative chemotherapy. Therefore, we cannot draw definitive conclusions regarding the complication profile of ports vs. PICCs in our patient cohort.
Fifth, given the unavailability of complete information on the duration of chemotherapy in our patients, we could not perform a review the port utilization times. This would have allowed us to identify the patients that may have required venous access for shorter durations of chemotherapy treatment, and as result could have been better served with less invasive and more cost-efficient PICCs.
Notwithstanding the above limitations, we believe that our findings provide useful and relevant information that should be considered in a multi-disciplinary approach by oncologists, palliative care specialists, and vascular access clinicians when advising patients on the choice of vascular access device for palliative chemotherapy.
Furthermore, our study underscores the need for larger, multi-center, prospective randomized studies comparing the risks and benefits of ports vs PICCs in patients undergoing palliative chemotherapy.
Conclusions
Our study shows that a significant number of patients undergoing port placement for palliative chemotherapy develop complications requiring corrective surgery. The median survival of our patients was just over 6 months, which is within the window that one could consider less invasive vascular access options, such as PICCs. Further research is required to analyze the risks and benefits of different types of vascular access devices in palliative chemotherapy patients, and ultimately develop clearer guidelines to help palliative patients decide what type of vascular access device is best for their needs.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.