
Abstract
Background:
Despite some insurance plans now paying for home-based palliative care, recent reports have suggested that insurance coverage for palliative care may be insufficient in expanding patient access to home-based palliative care.
Aim:
To identify patients’ and caregivers’ perceived barriers to home-based palliative care and their recommendations for overcoming these barriers.
Design:
We conducted a qualitative study using semi-structured individual interviews. Our interview protocol elicited participants’ perspectives on home-based palliative care services; positive and negative aspects of the palliative program explanation; and suggestions for improving messaging around home-based palliative care.
Setting/Participants:
Twenty-five participants (patients, proxies, and their caregivers) who were eligible for a randomized controlled trial of home-based palliative care were interviewed by telephone.
Results:
Themes related to home-based palliative care referral barriers included reluctance to have home visits, enrollment timing, lack of palliative care knowledge, misconceptions about palliative care, and patients’ self-perceived health condition. Themes related to recommendations for overcoming these obstacles included ensuring that palliative care referrals come from healthcare providers or insurance companies and presenting palliative care services more clearly.
Conclusion:
Findings reinforce the need for additional palliative care education among patients with serious illness (and their caregivers) and the importance of delivering palliative care information and referrals from trusted sources.
Keywords
Introduction
Numerous studies have shown that palliative care decreases patient symptom burden, improves the quality of life of patients and their caregivers, and reduces hospitalizations.1-5 Palliative care is defined as “specialized medical care for people with serious illness. It is focused on providing relief patients with relief from the symptoms, pain and stress of serious illness.” 6 According to the World Health Organization, about 40 million people are in need of palliative care; however, only about 14% receive it. 7 Moreover, some research suggests that patients who can benefit from palliative care are identified too late in the disease trajectory to fully benefit from the care. 8
In the last decade, palliative care has expanded internationally in hospitals and outpatient settings, enabling more individuals to access palliative care. 9 Despite this growth, community and home-based palliative care (HBPC) remains unavailable to many seriously ill patients. 10 In recent years, however, some insurance plans have begun paying for HBPC,11,12 thus ostensibly eliminating a financial obstacle to accessing HBPC among seriously ill patients. Yet recent reports suggest that insurance coverage for palliative care may be insufficient to expanding patient access to HBPC.12,13
Previous research examining obstacles to the delivery of palliative care among healthcare professionals helps explain the persistent lack of patient referral and subsequent enrollment in HBPC programs.14,15 In this study, we explored palliative care barriers from the perspective of patients and their caregivers who had been previously recruited and were eligible for palliative care under a randomized controlled trial (RCT). 16 The objective of this study was to identify patient, proxy, and caregiver perceived barriers to HBPC enrollment and their recommendations for overcoming these challenges.
Methods
We conducted semi-structured, individual telephone interviews among community dwelling seriously ill patients, their proxies, and their caregivers who were recruited to participate in a RCT of HBPC.
Original RCT Recruitment
Patient eligibility criteria for the original RCT included the following: being 18 years of age or older; having a diagnosis of congestive heart failure, chronic obstructive pulmonary disease (COPD), or advanced cancer; having 1 or more hospitalizations or emergency department visits in the previous year; and having an Australia-modified Karnofsky Performance Scale score of <70%. 16 If the patient lacked capacity to consent, the research assistant (RA) interviewed the proxy. Among proxies interviewed, all were family members and 1 also identified as a caregiver. Caregiver eligibility criteria included: being 18 years of age or older; being able to provide consent; and being an informal caregiver for a patient who had consented to participate in the study. 15 Further information on the RCT methodology has been published elsewhere. 16
Current Palliative Care Study Participant Identification and Recruitment
For the current study and separate from the previous RCT, we used purposive sampling to intentionally identify and recruit both those who enrolled in the RCT and those who were eligible but refused to participate. We purposively sought the opinions of palliative care-eligible participants and their caregivers on barriers to palliative care and their recommendations for overcoming these challenges. RAs first sent a study information sheet to potential participants, informing them of the aim of the research. This was followed by a telephone call from a RA to review the aims of the study and obtain verbal consent from the study participant. Our minimum targeted sample for this study was 10 participants enrolled in the original RCT and 15 who were preliminarily eligible for the RCT but refused participation, numbers predetermined by our funder.
Interview Protocol
We conducted telephone-based, audiotape-recorded individual interviews that lasted between 10 and 35 minutes. We used a semi-structured protocol to elicit participants’ perspectives on HBPC services. We asked all respondents to identify both positive and negative aspects of HBPC and elicited participant suggestions for improving the way HBPC was introduced to them and the messaging around HBPC. We also asked all participants whether they had previously heard about palliative care and asked for reasons why they or others might decline HBPC services. Each participant received a $50 gift card for participating. Interviews were conducted by a study manager with a Master of Public Health degree and more than 10 years of research experience, including qualitative interviewing. The interviewer disclosed her role on the research study to study participants. The study was approved by the (blinded)’s Institutional Review Board.
At the end of the interview, we collected participant demographic information, including age, gender, ethnicity, marital status, education, work status, and current medical conditions.
Analysis
Audio-taped recordings were transcribed verbatim by trained graduate RAs and transferred to a spreadsheet program. Using grounded theory analysis, 2 researchers (VC, YZ) initially open-coded participants’ responses to generate concepts that described and interpreted the data. From these rudimentary codes, we generated core themes that identified barriers and recommendations to overcome identified challenges to HBPC. Once themes were identified, the same researchers (blinded) individually coded the transcripts, comparing codes and categories throughout the process. They then compared and reconciled their final coding until they reached 100%. Although we reached thematic saturation by the 15th interview, we continued to code all transcripts, according to our contract with our funder.
Results
From October 2019 to May 2020, we interviewed 17 patients and 8 caregivers/proxies. Of these individuals, 15 were recruited from among 109 RCT-eligible participants who refused to participate in the RCT, and 10 were recruited from among 28 RCT-eligible participants who enrolled in that RCT. Of these 10 participants, 6 were randomized to HBPC while the remaining 4 received usual care.
Participant Demographic Characteristics
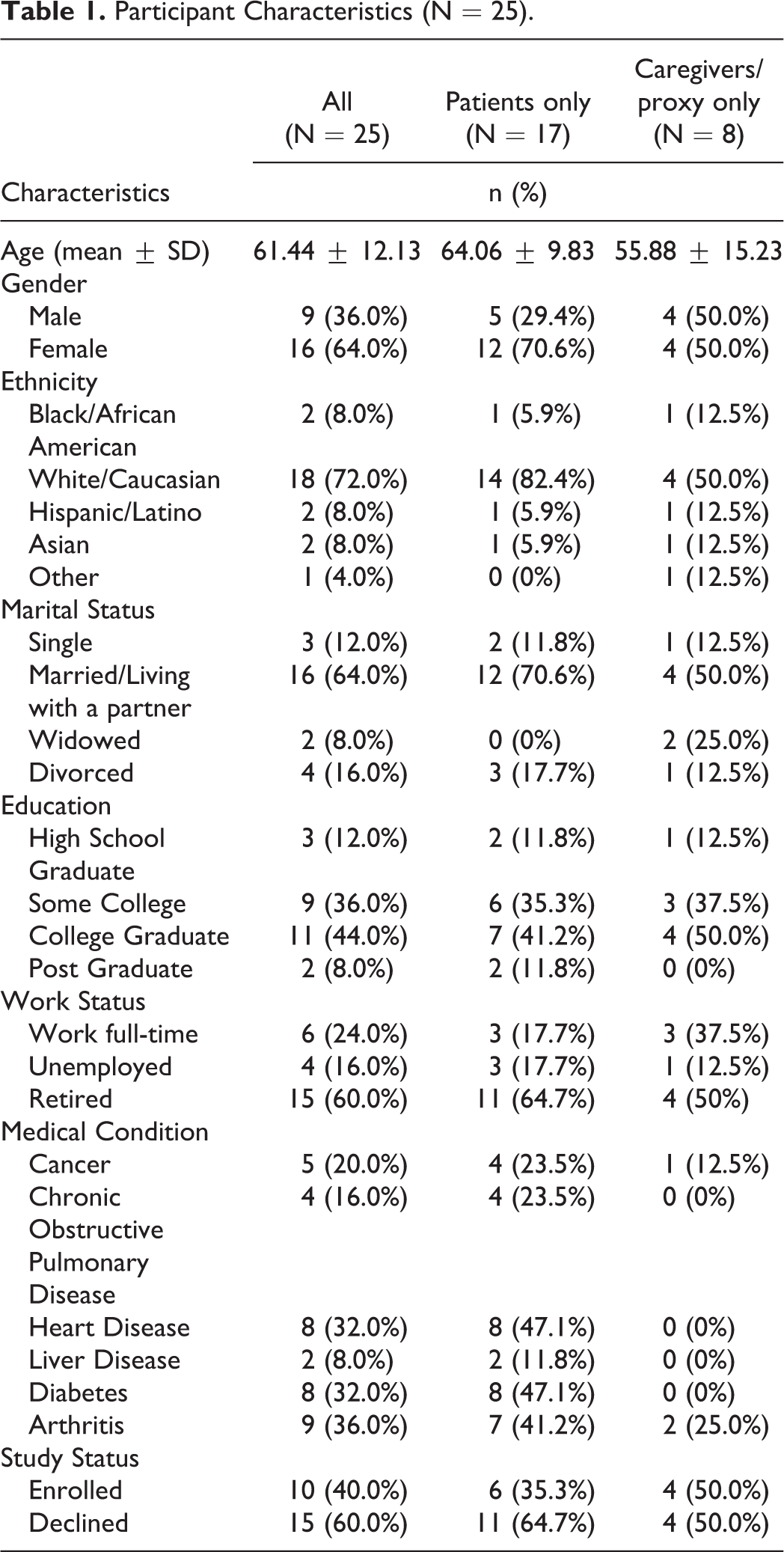
Table 1 presents demographic characteristics for patients, caregivers, and proxies. Of the 17 patient participants, most were female (70.6%), white (82.4%), and married (70.6%). Patients reported an array of health conditions. Of the 8 participating caregivers and proxies, half were male (50.0%), white (50.0%), married (50.0%), college graduates (50.0%), and retired (50.0%).
Participant Characteristics (N = 25).
Themes
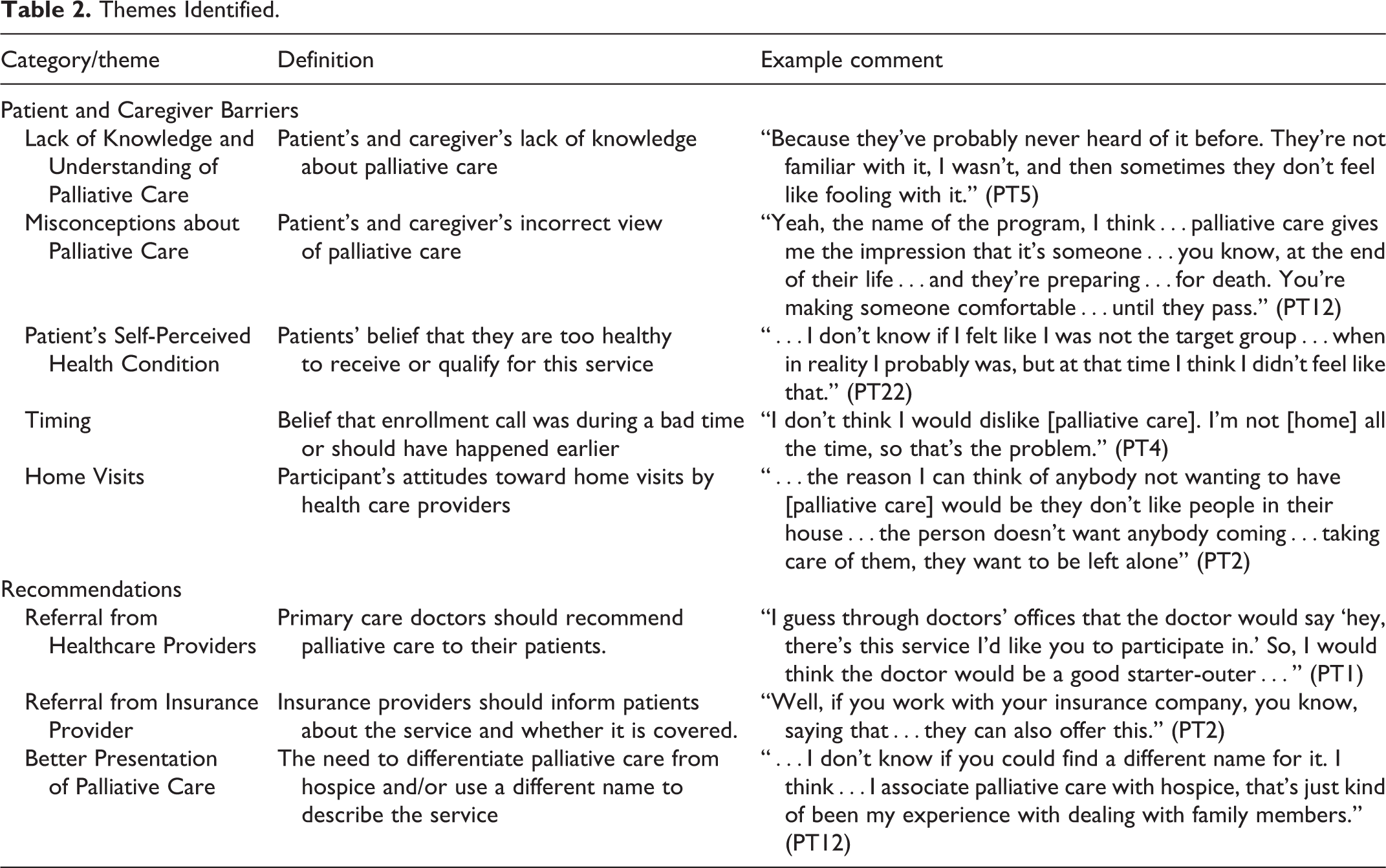
From the transcripts, we identified 5 themes related to barriers to HBPC and 3 themes related to recommendations for overcoming these obstacles. Themes are presented below and defined in Table 2.
Themes Identified.
Patient and Caregiver Barriers to HBPC
Lack of knowledge and understanding of palliative care
Nearly all participants in this study mentioned that they had never heard of palliative care prior to being recruited for the RCT study. One caregiver (#18) shared that she first learned about palliative care during the RCT study recruitment process: “It was the information that I received from you when you made the first call…you explained to me what it was. That’s when I learned that there was this kind of service. We had no idea before.”
Misconceptions about palliative care
Additionally, some participants shared their misconceptions about the HBPC service, expressing the mistaken belief that palliative care is offered only at end-of-life and is synonymous with hospice. One enrolled patient (#8) discussed what others may believe and what she initially thought about palliative care: “Because I think they look at palliative care as being…part of hospice and it’s going to end their life, which isn’t true at all. That was what I always thought too.”
Patient’s self-perceived health condition
Several participants believed they were too healthy for palliative care and did not understand how they qualified for palliative care. Some reported that they felt their health had been improving. Others were still working and did not need help, and some took offense to the palliative care recruitment call. A participant who declined RCT participation (#12) reported these initial thoughts: “…at first I was kind of taken aback by [the recruitment call] because I was doing better, so I didn’t see how, at first, I was qualified for this…because I wasn’t as sick as I was in years before.”
Timing
Some participants told us that the invitation to receive palliative care came at a bad time or too late in their disease trajectory. Some participants who declined palliative care shared that the call occurred at a time when they felt overwhelmed with their own care or that of their family member and could not attend to the call. “It was the timing that…we got the call. And we were going through all kinds of stuff with…his care, and…the doctors…and everything. It was just too much at once. It was becoming not manageable for me.” (CG15) “I’ll be honest, this kind of call needed to happen a year ago.”
Home visits
Several participants, both those who declined and those who enrolled in the RCT, mentioned potential hesitancy about having healthcare professionals come into their homes and the added stress these visits could bring. According to 1 participant who declined RCT enrollment (#22): “…there’s someone that’s gonna come over who I don’t know. And then…are they gonna bring more…germs into the house? Or…do I have to clean up the house?…I felt like it was…an additional burden.”
Recommendations
Referrals from healthcare providers
Some participants recommended that researchers should mention their (the participants’) healthcare provider during recruitment or have their doctor recommend the service to them. As mentioned by 1 participant who declined RCT enrollment (#11): “If you had worked with any of the doctors or could name any of my doctors…it would have…perked my interest a bit.”
Referral from insurance provider
Several enrolled and declined patients recommended that we recruit through their insurance company and mention that palliative care is free of charge. One enrolled patient (PT8) shared how this strategy worked for her: “I made the call [to the research team] because [the insurance company] had sent me a letter asking me if I would participate, and I knew it was a legitimate letter, so that’s when I reached out and called the number where you guys are from.”
Better presentation of palliative care
Participants who enrolled in the larger RCT recommended that palliative care be explained better by healthcare providers so that patients and their caregivers fully understand the term. Some participants even suggested replacing “palliative care” with a different name. An enrolled patient (PT2) mentioned: “…if you explain to them it’s not hospice…explain to [them] exactly what it is, I think most people would, you would do it. You know? I couldn’t understand why anybody wouldn’t.”
Discussion
This study explored obstacles to enrollment in HBPC and recommendations for overcoming these challenges from the perspective of HBPC-eligible patients and their caregivers. Participants identified obstacles related to palliative care knowledge, their perceptions of need for HBPC, enrollment timing, and home visits. Participants’ recommendations for improvement centered on referral sources and messaging, with implications for how HBPC is marketed.
In keeping with findings from previous research, 13 our findings showed that patients and caregivers’ lack of palliative care knowledge was a barrier to HBPC use. It should be reiterated that all patients eligible for this study (and the earlier RCT) were diagnosed with cancer, COPD, or congestive heart failure, reported significant functional decline, and reported a recent emergency room or hospital admission. In other words, they qualified for insurance-covered HBPC. Yet, nearly all participants had never heard of palliative care prior to the RCT enrollment call. Moreover, more than a year after the first RA contact, many participants still did not understand palliative care. Just 3 of this study’s 25 participants were knowledgeable about palliative care and all 3 had enrolled in the RCT (1 was randomized to HBPC), and all 3 participants had different levels of education and medical conditions. In addition to their lack of knowledge, participants often assumed palliative care equates to hospice. This finding is consistent with that of a study of heart failure patients, where the majority of respondents eligible for palliative care had limited knowledge that palliative care was a recommended component of their care and conflated it with hospice. 17
Lack of knowledge and misconceptions about palliative care are common throughout the world.18-20 In a nationally representative survey, about 34% of respondents said they had some knowledge of palliative care and, among these, just 41% were able to answer 3 basic palliative care knowledge questions correctly. 18 Similarly, in a Canadian survey of patients with stage 5 chronic kidney disease, about 63% of respondents stated they were familiar with palliative care, however only 22.2% of these were able to correctly describe palliative care. 19 In these studies, the most common misconception was that palliative care equates to hospice.
Several patients who qualified for but declined to participate in the RCT cited their current health condition as a reason for refusing HBPC. Some participants felt they were too healthy for and therefore did not need HBPC. Misconceptions about palliative care and patients’ lack of palliative care knowledge may have influenced their receptivity to receiving this service. 21 Patients may not know that palliative care can be an option early in the course of an illness. Another possibility is that some patients may have been reluctant to acknowledge the extent of their illness.
Another obstacle to enrolling patients in HBPC was the timing of recruitment. Some participants were overwhelmed with health-related matters at the time the RAs called to discuss palliative care. Seriously ill patients and their caregivers often face substantial burdens, such as financial hardships, emotional burdens, and social sigma.22,23 While palliative care can improve patient and caregiver quality of life,5,24,25 palliative care teams need to find ways to approach overburdened patients and caregivers. On the contrary, and in agreement with the participants who said the invitation to access HBPC came too late, research has shown late timing in palliative care referrals.8,26
Finally, some participants who declined RCT enrollment told us they were reluctant to have healthcare professionals provide care in their homes. In recent research, primary care providers also have identified this reluctance as a potential patient barrier to receiving HBPC. 13 Home healthcare agencies have cited invasion of privacy, fear of the unknown, and managing care at home as the most common reasons for refusing care at home. 27 Notably, the recruitment for the larger RCT took place prior to the start of COVID-19 as did the majority of the interviews for the current study, therefore COVID-19 most likely did not influence responses.
Some participants suggested it would be better to introduce palliative care to patients by clearly differentiating it from hospice and end-of-life care or using a different name for the service. Others have offered similar recommendations,28,29 which have contributed to an ongoing debate about the branding of palliative care.
While acknowledging that palliative care’s close association with end-of-life care scares many patients, some palliative care advocates have argued that rebranding palliative care (e.g., “supportive care”) is unnecessary, intellectually dishonest, and ultimately will not work. 30 Rather than abandon the term, the Center to Advance Palliative Care (CAPC) has recommended carefully framing it. CAPC advocates that providers refrain from mentioning “hospice care” when introducing palliative care, even to help explain what it is not (e.g., “it is not hospice care”), for fear that doing so will create a positive association between the terms in the listener’s mind. 31
Persistent resistance to palliative care by patients, however, has prompted a growing number of palliative care programs, many of them offshoots of hospice programs, to rebrand their services. Results have been promising. When the palliative care program at The University of Texas M.D. Anderson Cancer Center rebranded itself as supportive care, the number of patient consultations increased by 41% and led to earlier referrals. 32 In another study, when patients with pulmonary arterial hypertension were asked if they would be more accepting of palliative care if it were called supportive care, more agreed (31%) than disagreed (22%), although most (47%) were indifferent to the name change. 33
Our study’s findings corroborate persistent research findings that patients and their caregivers are confused about what palliative care is and fearful it equates with hospice care. Given this, we believe the onus is on healthcare providers to clarify the differences between palliative care and hospice and build trust with patients and their caregivers during the referral process.
Some study participants recommended that HBPC referrals and information about palliative care come from their doctor or insurance provider. The preference for a physician referral is consistent with recommendations made by other patients and caregivers.13,34 Such referrals could address some of the barriers to HBPC enrollment identified in this study. During the referral process, physicians could educate patients about palliative care and discuss with them the reason for the referral and its timing. Such consultations would help mitigate enrollment barriers related to lack of palliative care awareness, poor referral timing, and patient perception of service need.
In practice, however, physicians, have been slow to refer their patients to palliative care. 12 A recent survey by the CAPC found that, while most physician respondents were comfortable referring their patients to palliative care, on average, they reported they were “not always referring their patients with serious illness to palliative care, or talking with their patients or their families about palliative care.” 31 Most said they tended to refer patients to palliative care when they had a terminal diagnosis or no viable treatment options, essentially using the same criteria used for hospice referrals. 31
In the present study, some participants viewed an insurance-driven referral process favorably. Among insurance companies that provide a palliative care benefit to subscribers, a growing number are using the data they collect to identify patients who might benefit from HBPC and then giving that list to palliative care providers so that they can reach out directly to the patients. While this outreach strategy can be effective, it lacks the “warm hand-off” between providers that some patients—and healthcare providers—prefer. 34 As the HBPC industry continues to expand, researchers and other key stakeholders should continue to evaluate the effectiveness and acceptability of referral processes used to identify and enroll patients in HBPC programs.
Strengths and Limitations
This is one of few studies that examines perspectives of patients and caregivers on referral to palliative care, and the first that specifically examines perspectives of HBPC. Our study’s findings are based on the perspectives of a purposive sample of RCT and HBPC-eligible participants. Responses may have been influenced by the combined introduction to HBPC and the RCT.
Conclusion
This study demonstrated the lack of awareness of palliative care among palliative care-eligible patients (and caregivers). Study findings reinforce the need for additional palliative care education among patients with serious illness (and their caregivers) and the importance of ensuring that trusted sources refer patients to HBPC as strategies for improving palliative care utilization. Findings also support studies examining the need for improved messaging around palliative care services.
Footnotes
Acknowledgments
The authors would like to thank the patients and caregivers who participated in our study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded through a Patient-Centered Outcomes Research Institute (PCORI) Award IHS-1602-34070. The opinions presented in this manuscript are solely the responsibility of the authors and do not necessarily represent the views of the PCORI, its Board of Governors, or MethodologyCommittee.