
Abstract
Background:
Parents often suffer reduced mental health after their child’s death; however, the trajectory and risk factors are not well described.
Objective:
Describe the change in complicated grief, depression, and post-traumatic stress symptoms among parents between 6 and 13 months after their child’s death in a pediatric intensive care unit (PICU), and factors associated with 13-month symptoms.
Methods:
Parents whose children died in 1 of 8 PICUs affiliated with the Collaborative Pediatric Critical Care Research Network completed surveys 6 and 13 months after their child’s death. Surveys included the Inventory of Complicated Grief (ICG), the Patient Health Questionnaire-8 (PHQ-8) for depression, and the Short Post-Traumatic Stress Disorder Rating Interview (SPRINT). Parents provided sociodemographics. Charts were reviewed for child characteristics.
Results:
One-hundred and fifty seven parents of 104 deceased children completed surveys at both time points. Mental health symptoms declined over time (mean (SD)): ICG (33.8 (15.4) vs. 30.5 (15.2), p < 0.001), PHQ-8 (9.0 (6.4) vs. 7.3 (5.8), p < 0.001), and SPRINT (14.1 (8.3) vs. 12.0 (8.2), p < 0.001). After controlling for 6-month scores, higher 13-month ICG was independently associated with sudden unexpected death; higher PHQ-8 with Black race, insecure attachment style, and sudden unexpected death; and higher SPRINT with having a high school level of education (compared to college degree or higher).
Conclusion:
Mental health symptoms improve among parents during the first 13 months after their child’s death; however, symptoms persist for many. Black parents and those whose children die suddenly may be high risk for poor adjustment during bereavement.
Introduction
Although grief following the loss of a loved one is highly variable, normative grief typically diminishes over time as the reality of the loss is integrated into the bereaved person’s life. 1 Other normative patterns of grief have been recognized including resilience with low levels of distress throughout bereavement, chronic grief with persistent emotional pangs of sadness, and a distressed-improved pattern characterized by a sense of relief due to an end to suffering or caregiver burden. 1 Disordered patterns of grief such as prolonged or complicated grief also occur and are characterized by severe and persistent symptoms that interfere with daily functioning.2,3
Parental grief after the loss of a child has been shown to be more intense and prolonged than that experienced by adults after the loss of a spouse or parent.4,5 Researchers have suggested that parental grief may represent a distinct subtype of grief in which symptoms of anxiety, depression, post-traumatic stress disorder (PTSD) and complicated grief are common. 6 Rather than representing a pathological reaction, these adverse mental health symptoms may be expected among bereaved parents considering the close and enduring nature of the parent-child relationship. We previously demonstrated that 60% of bereaved parents screened positive for complicated grief 6 months after their child’s death in a pediatric intensive care unit (PICU), 52% for PTSD, and 43% for at least moderate depression.7,8 Whether normative or not, these symptoms reflect the intense suffering experienced by bereaved parents.
Few studies have evaluated changes in bereaved parents’ mental health symptoms over time.9-13 Available data suggest that mental health symptoms decline during the first year after a child’s death for many parents but not all. Our objective was to (1) describe the change in complicated grief, depression, and post-traumatic stress symptoms among bereaved parents between 6 and 13 months after their child’s death in a PICU, and (2) identify factors associated with parents’ mental health symptoms at 13 months. Better understanding of how mental health symptoms evolve in bereaved parents and the identification of risk factors for persistent symptoms may help to inform the timing of supportive interventions and the identification of parents at greatest risk of poor outcomes.
Methods
Design and Setting
The study was a multicenter survey conducted between September 2016 and March 2019 across 8 children’s hospitals affiliated with the Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network (CPCCRN). Parents were asked to complete surveys 6 and 13 months after their child’s death in a PICU. 8 The study was approved by the University of Utah Institutional Review Board (Protocol 00095029) serving as the central IRB for the CPCCRN. Consent was by written waiver for parents returning surveys by mail and verbal for parents completing surveys by telephone.
Participants
Parents, defined as biological parents and/or legal guardians, were eligible for participation if their child died in a PICU, were English or Spanish speaking, and at least 18 years of age. Only parents who returned surveys at both time points were included in the current analysis. Parents of 710 children were asked to complete a survey 6 months after their child’s death. 8 Of these, 235 parents of 158 deceased children (22% of eligible families) returned a 6-month survey. All 6-month respondents were asked to complete a 13-month survey. Of these, 157 parents of 104 deceased children returned a 13-month survey (15% of eligible families) and are the subjects of this report.
Data Collection
Parents were mailed surveys in English or Spanish at 6 and 13 months after their child’s death. If completed surveys were not returned within 1 month of mailing, telephone contact was attempted to offer the parents the option of completing the survey by telephone. If the household was successfully contacted by telephone but the survey was not completed, the parent was categorized as a refusal to participate. If the household could not be contacted by telephone after 3 or more attempts, the parent was categorized as unable to contact.
Surveys administered at 6 months asked parents to provide information on their age, gender, race, ethnicity, marital status, education level, relationship to the deceased child (i.e., biological or other), and number of surviving children. Surveys at 6 months included the Human Connection Scale (HCS), 14 the Revised Adult Attachment Scale (RAAS),15,16 the Inventory of Complicated Grief (ICG), 17 the Patient Health Questionnaire-8 (PHQ-8)18,19 and the Short Post-Traumatic Stress Disorder Rating Interview (SPRINT). 20 Surveys administered at 13 months were a subset of these including the ICG, PHQ-8, and SPRINT. Medical records of the deceased children were reviewed for child gender, age at time of death, cause of death, trajectory of death, mode of death, and PICU and hospital lengths of stay. Trajectory of death was categorized as sudden unexpected death, death from a potentially curable disease, death from a lethal congenital anomaly in the first few weeks of life, or death from a progressive condition with intermittent crises. 21 Mode of death was categorized as limitation or withdrawal of life support, brain death, or unsuccessful cardiopulmonary resuscitation.
Description of Instruments
The HCS is a 16-item measure originally designed to evaluate therapeutic alliance between adult cancer patients and oncologists. 14 The original scale assesses (1) physician understanding of patient concerns, (2) mutual caring and respect, (3) patient understanding of information, (4) patient trust in physician, and (5) collaboration. The HCS was adapted to assess therapeutic alliance between parents and their child’s PICU physicians by changing the phrase “your doctor” to “your child’s doctor(s) in the ICU” in each item. 8 Responses are reported on a 4-point scale from 1 (not at all) to 4 (a great deal). Summed scores range from 16 to 64; higher scores indicate greater therapeutic alliance. Cronbach’s α was 0.96 in our study population using 6-month survey data. 8
The RAAS is an 18-item measure that assesses adult attachment style.15,16 Respondents rate the extent that each item describes their feelings about close relationships on a 5-point scale ranging from 1 (not at all like me) to 5 (very much like me). Subscale scores reflect 2 dimensions of attachment, attachment-related anxiety and attachment-related avoidance. Subscale scores are a mean of the relevant items and range from 1 to 5; higher scores indicate more anxious or avoidant attachment. Cronbach’s α was 0.73 for attachment-related anxiety and 0.88 for attachment-related avoidance in our study population using 6-month survey data. 8
The ICG is a 19-item measure that assesses the frequency of complicated grief symptoms. 17 Responses are rated on a 5-point scale ranging from 0 (never) to 4 (always). Item responses are summed to obtain total scores that range from 0 to 76. Scores of 30 or greater at least 6 months after a death have been suggested as a positive screen for complicated grief. 22 Cronbach’s α was 0.99 in our study population using 6-month survey data. 8
The PHQ-8 is an 8-item measure that assesses the frequency of depression symptoms.18,19 Responses are rated on a 4-point scale from 0 (not at all) to 3 (nearly every day). Items are summed to obtain total scores that range from 0 to 24. Scores of 5, 10, 15 and 20 have been suggested as positive screens for mild, moderate, moderately severe, and severe symptoms, respectively. Cronbach’s α was 0.995 in our study population using 6-month survey data. 8
The SPRINT is an 8-item measure that assesses the frequency of post-traumatic stress symptoms. 20 Responses are rated on a 5-point scale from 0 (not at all) to 4 (very much). Items are summed to obtain total scores ranging from 0 to 32. Scores of 14 or greater have been suggested as a positive screen for PTSD. 20 Cronbach’s α was 0.997 in our study population using 6-month survey data. 8
Statistical Analysis
Data are summarized using frequencies and percentages for categorical variables, and means and standard deviations for continuous variables. Responders and non-responders to the 13-month survey were compared using t-tests for continuous variables, Fisher’s exact tests for categorical variables and Cochran-Armitage trend test for discrete ordinal variables. The 3 outcomes of interest: ICG, PHQ-8 and SPRINT were first examined by measuring the change in score between 6 and 13 months with significance of changes over time assessed using linear mixed models (these included a random effect to account for correlation between parents of the same child). The proportion of parents exceeding appropriate screening cut-off values for each outcome at 6 months versus 13 months was compared using mixed effects logistic regression models (these included random effects to model correlation between each individual parent’s responses at the 2 time points, as well as to account for between-2-parent correlation). In order to model the change in scores over time, while also taking into account correlation between parents of the same child, linear mixed models were used with child as the random effect and 6-month score being one of the covariates. For each of the 3 outcomes, each potential predictor was modeled with 6-month score as a covariate and 13-month score as the outcome. Variables with p-values <0.2 in these “screening” models were then considered for inclusion in the multivariable model. Multicollinearity was assessed for all candidate predictors; where 2 candidate predictors had high correlation (>0.7), the most clinically relevant variable was included in the full model. To construct the final models, manual backward selection was performed on each multivariable mixed model containing candidate predictors until all remaining predictors had a p-value <0.1. We also report the proportion of variance explained by our multivariable models, which include fixed as well as random effect for individual, using 2 approaches following Nakagawa et al: 23 variance explained by fixed effects alone (termed marginal R-squared), and variance explained by the fixed and random effects in the model together (termed conditional R-squared). The R-squared statistics were calculated in R 24 using library MuMIn. 25
Results
Of 235 parents of 158 children (22% of eligible families) completing 6-month surveys, 157 parents of 104 children (15% of eligible families) completed 13-month surveys, 28 refused and 50 could not be contacted. Six-month survey respondents included 77 couples and 13-month survey respondents included 53 couples. Parents responding to the 13-month survey were more likely to be married and less likely to screen positive for complicated grief at 6 months than non-responders (Table 1). Other parent and child characteristics (Table 2) were similar between responders and non-responders.
Parent Characteristics by 13-Month Survey Response.
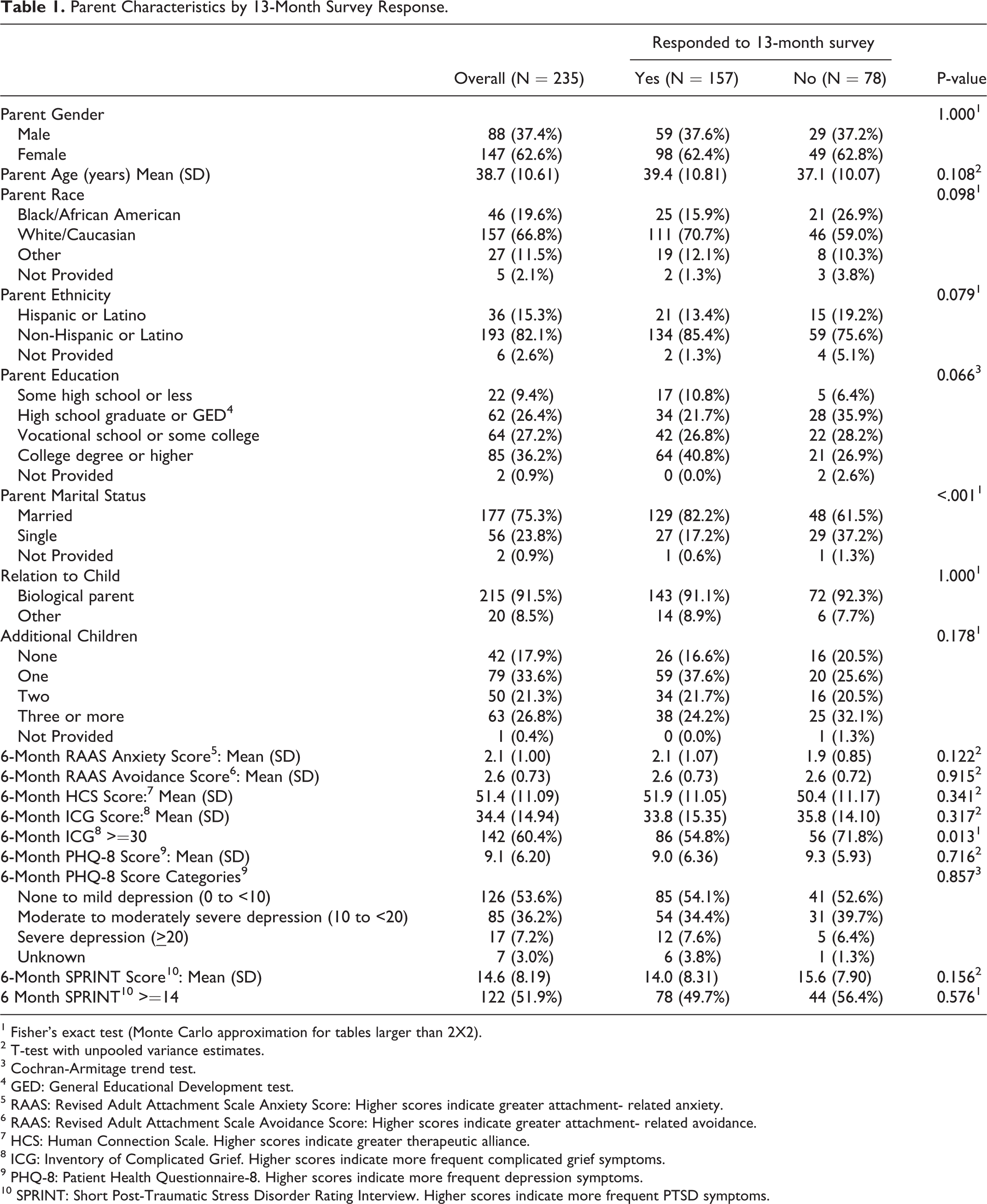
1 Fisher’s exact test (Monte Carlo approximation for tables larger than 2X2).
2 T-test with unpooled variance estimates.
3 Cochran-Armitage trend test.
4 GED: General Educational Development test.
5 RAAS: Revised Adult Attachment Scale Anxiety Score: Higher scores indicate greater attachment- related anxiety.
6 RAAS: Revised Adult Attachment Scale Avoidance Score: Higher scores indicate greater attachment- related avoidance.
7 HCS: Human Connection Scale. Higher scores indicate greater therapeutic alliance.
8 ICG: Inventory of Complicated Grief. Higher scores indicate more frequent complicated grief symptoms.
9 PHQ-8: Patient Health Questionnaire-8. Higher scores indicate more frequent depression symptoms.
10 SPRINT: Short Post-Traumatic Stress Disorder Rating Interview. Higher scores indicate more frequent PTSD symptoms.
Child Characteristics by 13-Month Survey Response.
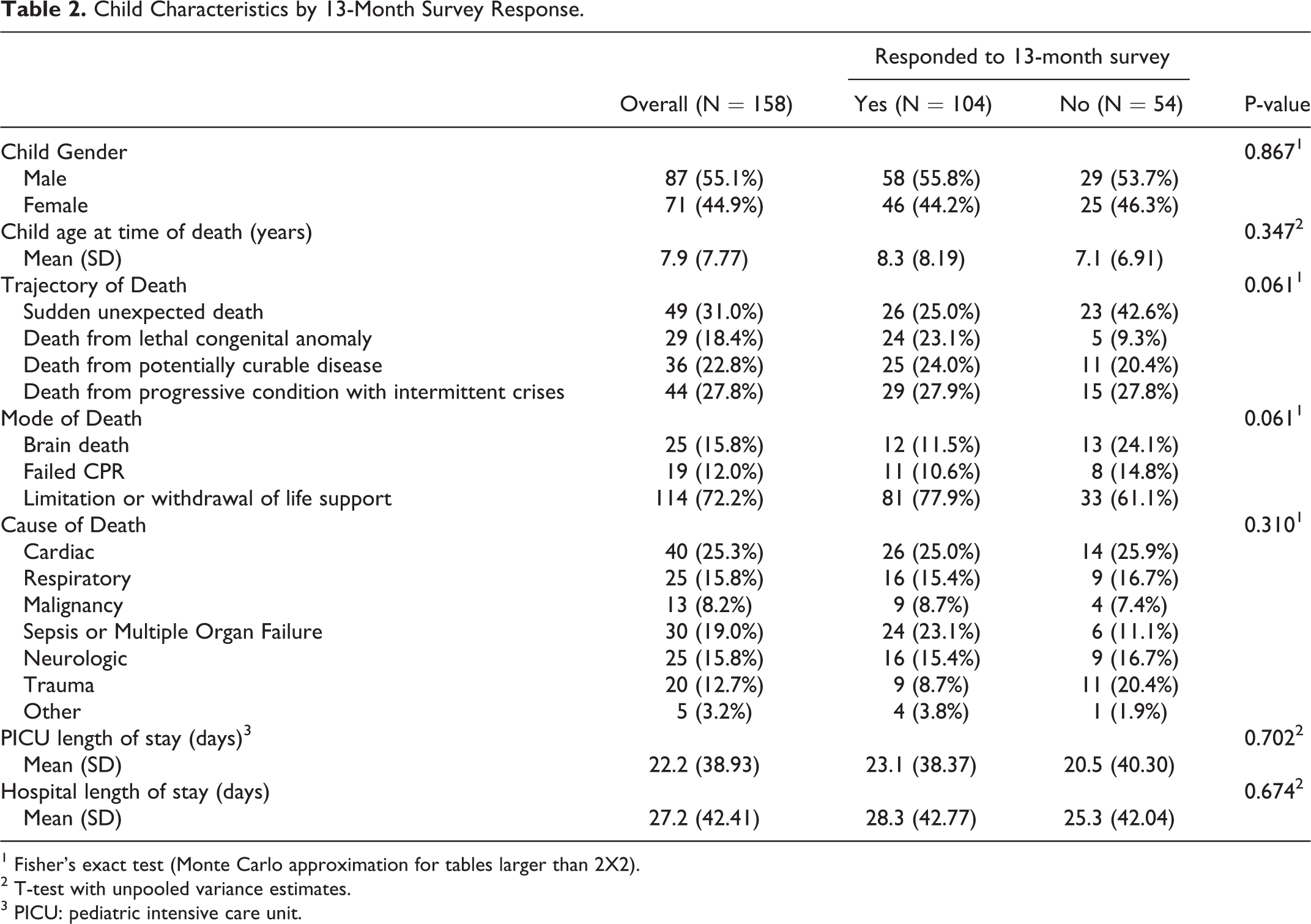
1 Fisher’s exact test (Monte Carlo approximation for tables larger than 2X2).
2 T-test with unpooled variance estimates.
3 PICU: pediatric intensive care unit.
Mental health symptoms decreased among parents at 13 months compared to 6 months (Table 3). Complicated grief symptoms, as measured by the ICG, decreased by 3.2 (8.7) points (p < 0.001). However, ICG scores were
Mental Health Outcomes at 6 Months, 13 Months and Change in Scores.
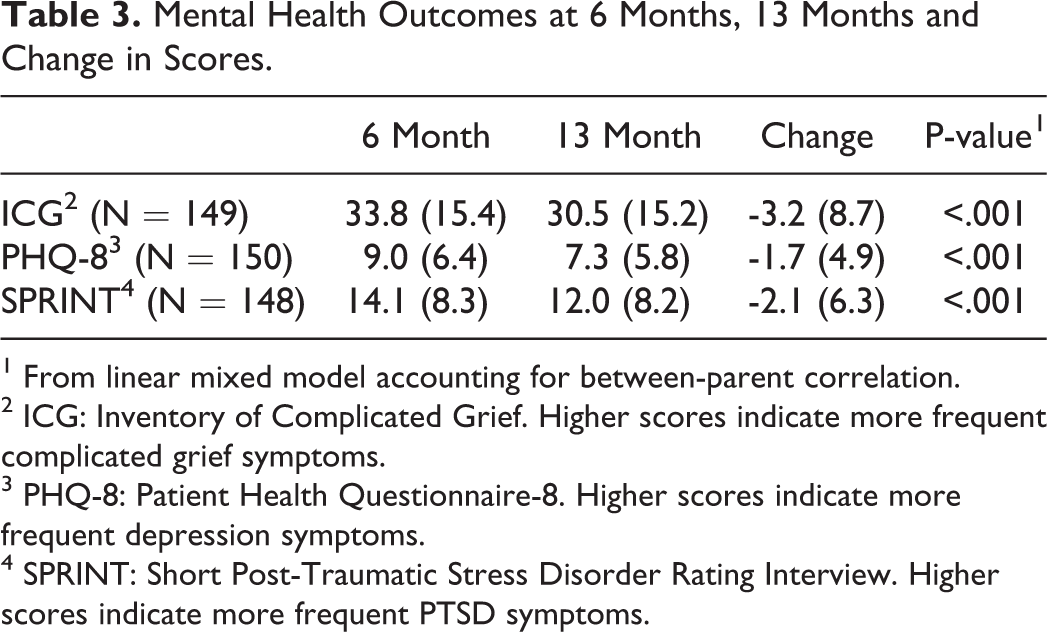
1 From linear mixed model accounting for between-parent correlation.
2 ICG: Inventory of Complicated Grief. Higher scores indicate more frequent complicated grief symptoms.
3 PHQ-8: Patient Health Questionnaire-8. Higher scores indicate more frequent depression symptoms.
4 SPRINT: Short Post-Traumatic Stress Disorder Rating Interview. Higher scores indicate more frequent PTSD symptoms.
Univariable associations between parent and child characteristics and 13-month mental health scores (ICG, PHQ-8, SPRINT) adjusted for 6-month scores are shown in Supplemental Material 1. Candidate predictors of 13-month ICG scores included parent age (p = 0.180), trajectory of death (p = 0.037), PICU length of stay (p = 0.151), and hospital length of stay (p = 0.076). PICU and hospital length of stay were highly correlated and thus only PICU length of stay was considered for the multivariable model. Candidate predictors of 13-month PHQ-8 scores included parent race (p = 0.027), parent education (p = 0.064), marital status (p = 0.005), relationship to child (p = 0.046), 6-month RAAS anxiety score (p = 0.116), 6-month RAAS avoidance score (p = 0.139), trajectory of death (p = 0.041) and mode of death (p = 0.117). Candidate predictors of 13-month SPRINT scores included parent race (p = 0.115), parent education (p = 0.017), marital status (p = 0.049), relationship to child (p = 0.132), and 6-month HCS score (p = 0.059).
Multivariable models for 13-month mental health scores (ICG, PHQ-8, SPRINT) are shown in Table 4. All models were adjusted for the corresponding 6-month mental health score. Higher 13-month ICG score was independently associated with sudden unexpected child death (compared to death from a congenital anomaly). Higher 13-month PHQ-8 score was independently associated with Black race (compared to White), higher RAAS anxiety score, and sudden unexpected death (compared to death from congenital anomaly or progressive condition). Higher 13-month SPRINT score was independently associated with parents having a high school education (compared to college degree or higher). Regarding the variance explained by only the fixed effects in these models, the R-squared is 0.70 for the ICG outcome, 0.53 for the PHQ-8 outcome, and 0.50 for the SPRINT outcome. Also including the variance explained by the random effects for individual, the R-squared is 0.81 for the ICG outcome, 0.60 for the PHQ-8 outcome, and 0.71 for the SPRINT outcome.
Multivariable Linear Mixed Models of Parental Health Outcomes at 13 Months.
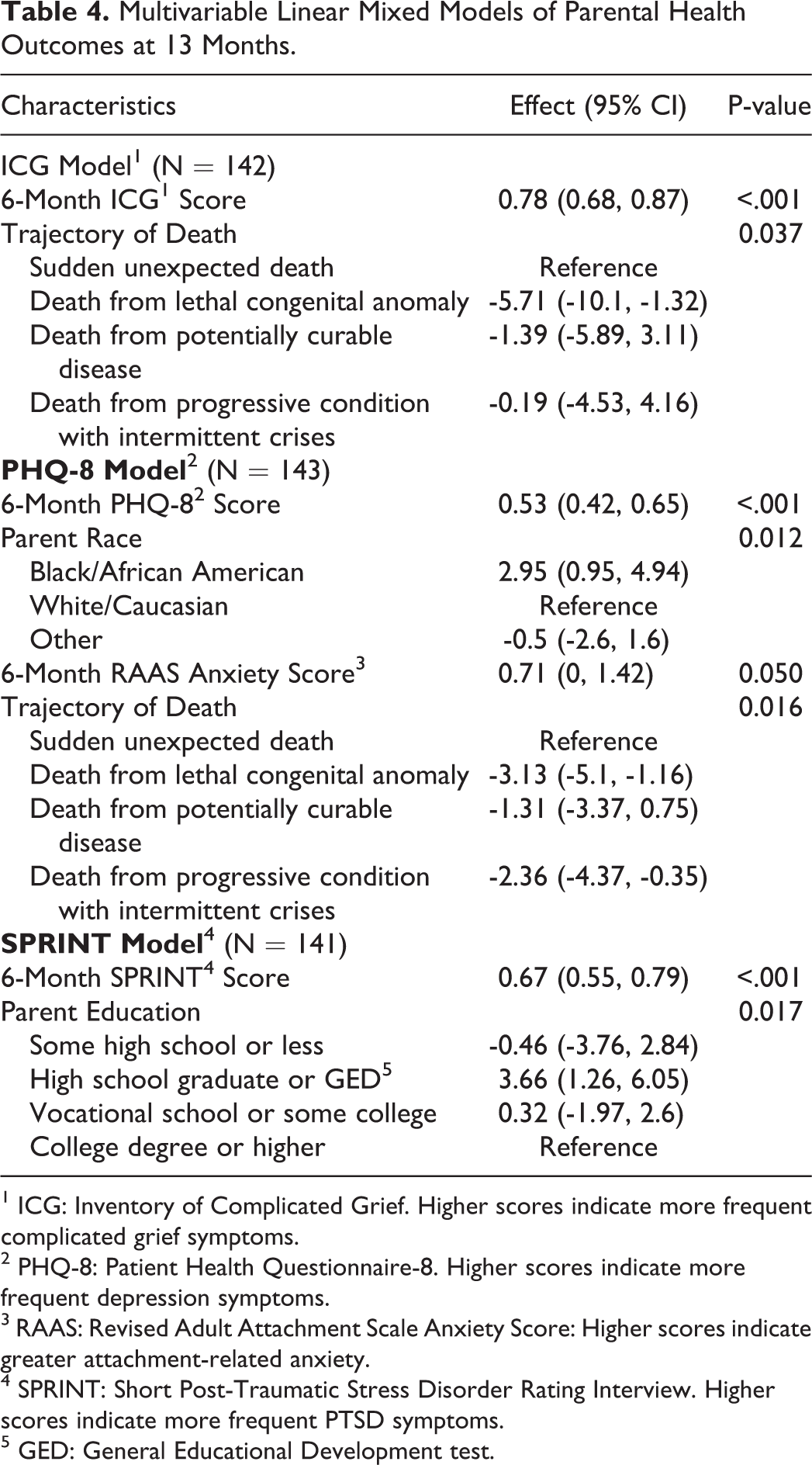
1 ICG: Inventory of Complicated Grief. Higher scores indicate more frequent complicated grief symptoms.
2 PHQ-8: Patient Health Questionnaire-8. Higher scores indicate more frequent depression symptoms.
3 RAAS: Revised Adult Attachment Scale Anxiety Score: Higher scores indicate greater attachment-related anxiety.
4 SPRINT: Short Post-Traumatic Stress Disorder Rating Interview. Higher scores indicate more frequent PTSD symptoms.
5 GED: General Educational Development test.
Discussion
Our study demonstrates a decrease in adverse mental health symptoms among bereaved parents between 6 and 13 months after their child’s death in a PICU. Although ICG scores declined, about half of parents (52.3%) screened positive for complicated grief at 13 months. Similarly, PHQ-8 and SPRINT scores decreased over this interval; however, 32.7% parents screened positive for at least moderate depression and 43.9% for PTSD 13 months after their child’s death.
Complicated grief is an unusually severe form of grief that persists beyond typical social and cultural norms and leads to impairment in daily functioning. Symptoms include intense yearning or longing for the deceased, inability to accept the reality of the death, preoccupying thoughts of the deceased, avoidance of reminders of the loss, and feeling that life is meaningless without the deceased person.2,3 Complicated grief is estimated to occur in about 7% of bereaved individuals. 26 However, consistent with other studies, our findings suggest that complicated grief occurs with higher frequency among parents who have lost a child.7,13,26
We previously demonstrated in our parent cohort that at 6 months after a child’s death symptoms of complicated grief were independently associated with greater parental attachment-related anxiety and avoidance, lesser therapeutic alliance between parents and their deceased child’s physicians, and shorter PICU lengths of stay. 8 Attachment-related anxiety is characterized by a negative self-image and fear that others will not be available in times of need whereas attachment-related avoidance is characterized by a negative view of others and discomfort relying on others.27,28 Both are insecure forms of attachment and have been associated with poor adaptation to loss. 29 Therapeutic alliance reflects the strength of the collaborative bond between parents and physicians and may have a positive impact on parents’ early grief symptoms. 8 In contrast to our findings at 6 months, only the trajectory of death independently predicted complicated grief symptoms at 13 months when adjusting for 6-month symptom scores. Parents whose children died suddenly and unexpectedly had higher levels of complicated grief symptoms than those whose children died of congenital anomalies in the first few weeks of life. Prior research estimates the prevalence of complicated grief in individuals bereaved suddenly by accidents, homicides or suicides to range from 12.5-78%. 30 Although not all sudden death is due to such violent causes, factors proposed to contribute to complicated grief in these situations include a lack of preparedness for the death, social stressors, the feeling of being judged by others, self-blame, and failure to make sense or find meaning in the loss.30,31
Depression is commonly reported among bereaved parents.9,32,33 We previously found that attachment insecurity, being a mother, and the death of an older child were independently associated with increased depression symptoms in our parent cohort 6 months after a child’s death. 8 At 13 months, we found attachment-related anxiety continued to be independently associated with depression symptoms. Insecure attachment may contribute to depression during bereavement because of a perceived lack of reliable social supports in those with high attachment-related anxiety, or failure to utilize social supports in those with high attachment-related avoidance. 29 In our cohort, sudden unexpected death was also independently associated with greater parental depression at 13 months compared to death from congenital anomalies or progressive conditions. Sudden unexpected death may be perceived as preventable, leading to feelings of self-blame. Guilt among bereaved individuals who experience sudden loss by accident, suicide or homicide has been suggested to contribute to depression symptoms. 34 Black race was independently associated with increased depression symptoms in our parent cohort 13 months after a child’s death. In the general U.S. population, Black Americans exhibit lower or equivalent rates of major depressive disorder than non-Hispanic Whites. 35 However, higher rates of moderate to severe depression have been reported among Black mothers compared to White mothers 6 months after a child’s death. 12 These findings may be due to numerous psychosocial stressors that compound grief for some bereaved Black parents including economic hardship, untimely deaths of significant others and perception of unfair medical treatment.36,37
Anxiety is a natural reaction to bereavement. 35 However, for some individuals, anxiety can become severe and manifest as PTSD, generalized anxiety disorder or panic disorder. 38 Attachment insecurity, being a mother, and sudden, unexpected death were independently associated with greater PTSD symptoms in our parent cohort 6 months after a child’s death 8 consistent with other reports.9,32,39,40 At 13 months, only parent education was independently associated with PTSD symptoms when adjusting for 6-month symptom scores. Parents with a high school education had significantly more PTSD symptoms than parents with a college degree or higher. However, an increase in PTSD symptoms was not observed for parents with less than a high school degree when compared to those with a college degree or higher. An explanation for why parents with high school education had the greatest increase in PTSD symptoms is not readily discernible from our data. Less education and lower income have more often been associated with PTSD. 41
Strengths of our study include multicenter recruitment, racial and ethnic diversity of participants, and the longitudinal study design. Limitations include our low overall participation rate. Only 158 of 710 (22%) total eligible families completed surveys at 6 months, and 104 (15%) of total eligible families completed surveys at 13 months. The low response rate may be due to bereavement-related distress and the added burden of participating in research. The information sheet distributed with the mailed surveys informed parents that the surveys were expected to take less than 60 minutes to complete. This time commitment could have dissuaded parents from participating. The extent to which parents who completed 6-month surveys were representative of all eligible parents is unknown because only parent inclusion criteria (i.e., child died in a PICU, English or Spanish speaking, at least 18 years of age) and contact information was collected from the medical records of children whose parents did not participate. More detailed review of children’s medical records was only performed for participating parents. Responders and non-responders to 13-month surveys were similar for most variables evaluated except that responders were more likely to be married and have lower levels of complicated grief symptoms 6 months after their child’s death. The potential for spousal support and less complicated grief symptoms among 13 month respondents may bias our results leading to underestimation of the mental health symptoms experienced by parents at 13 months. It is noteworthy that the predictive associations found at 6 months after a child’s death did not seem to persist at 13 months. Although the change in mental health scores between 6 and 13 months were statistically significant, the magnitude of change was relatively small; thus the inclusion of 6-month scores in the multivariable models contributed to most of the models’ prediction. It is also possible that parents’ mental health outcomes are influenced more by parents’ subjective experience and appraisal of their child’s death, coping mechanisms, social support, and other resources rather than by the sociodemographics or objective medical features evaluated in this study. All parents in this study experienced the death of their child in a large academic PICU. Although many childhood deaths in the U.S. occur in intensive care units, our findings may not be generalizable to parents whose children die in other locations such as hospital wards or home hospice care. The surveys used in this study to measure mental health symptoms were screening tools and are not diagnostic for complicated grief, depression or PTSD.
Conclusions
Mental health symptoms improve among parents during the first 13 months after their child’s death in a PICU; however, high symptom levels persist for many. Risk factors for high levels of mental health symptoms at 13 months include the extent of symptoms at 6 months, insecure attachment styles, sudden unexpected death of the child, and Black race. Findings suggest supportive interventions should be offered to parents for at least the first year after their child’s death with emphasis on the needs of Black parents and those whose children die suddenly.
Supplemental Material
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211015913 - Complicated Grief, Depression and Post-Traumatic Stress Symptoms Among Bereaved Parents following their Child’s Death in the Pediatric Intensive Care Unit: A Follow-Up Study
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211015913 for Complicated Grief, Depression and Post-Traumatic Stress Symptoms Among Bereaved Parents following their Child’s Death in the Pediatric Intensive Care Unit: A Follow-Up Study by Markita Suttle, Mark W. Hall, Murray M. Pollack, Robert A. Berg, Patrick S. McQuillen, Peter M. Mourani, Anil Sapru, Joseph A. Carcillo, Emily Startup, Richard Holubkov, J. Michael Dean, Daniel A. Notterman, Kathleen L. Meert and for the Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network (CPCCRN) in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
We thank Whit Coleman, MSRA, BSN, RN, CCRC, University of Utah; Stephanie Dorton, BSN, RN, CCRP, University of Utah; Nael Abdelsamad, MD, University of Utah; Kylee Arbogast, BS, RN, University of Utah; Kristi Flick, BS, MPH, University of Utah; Ann Pawluszka, BSN, RN, Children’s Hospital of Michigan; Melanie Lulic, BS, Children’s Hospital of Michigan; Carolann Twelves, RN, BSN, CCRC, Children’s Hospital of Philadelphia; Mary Ann DiLiberto, BS, RN, CCRC, Children’s Hospital of Philadelphia; Elyse Tomanio, BSN, RN, Children’s National Medical Center; Katherine Stone, Children’s National Medical Center; Kathryn Malone, Children’s Hospital Colorado; Diane Ladell, MPH, CCRC, Children’s Hospital Colorado; Ruth Grosskreuz, MD, CCRC, Children’s Hospital Colorado; Lisa Steele, RN, BSN, CCRC, CCRN, Nationwide Children’s Hospital; Maggie Flowers, BSN, Nationwide Children’s Hospital; Anna Ratiu, MPH, University of California, Los Angeles; Tanaya Deshmukh, MS, University of California, Los Angeles; Anne McKenzie, BSN, CCRN, University of California, San Francisco; Yensy Zetino, University of California, San Francisco; and Leighann Koch, BS, BSN, RN, University of Pittsburgh Medical Center.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by cooperative agreements from the Eunice Kennedy Shriver National Institute of Child Health and Human Development: UG1HD083170, UG1HD049981, UG1HD63108, UG1HD083166, UG1HD083171, UG1HD049983, U01HD049934, UG1HD050096.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.