
Abstract
Introduction:
Well-being and turnover intent represent key aspects to the promotion of a healthy workforce. Alarming levels of burnout and low levels of well-being have been documented in health professionals across care settings. Not only do high levels of burnout, low well-being and high turnover affect health professionals, but they are associated with poor patient care. However, limited research has investigated this topic specifically in hospice interdisciplinary team (IDT) members, nurses, chaplains, social workers. Thus, the purpose of this study was to explore hospice IDT members’ well-being, and turnover intent.
Methods:
This observational, pilot study used quantitative surveys to examine the well-being, and turnover intention at baseline and at 3 months. Twenty-five hospice IDT members at one site participated.
Results:
Paired t-tests and percent change demonstrated significant decreases in compassion satisfaction (44.5 vs. 42.1, p = 0.04) and secondary traumatic stress score (18.5 vs. 13.3, p = 0.0001) and a significant increase in burnout score (17.6 vs. 20.5, p = 0.03) from baseline to follow up. Employee turnover slightly decreased from baseline to follow-up.
Conclusions:
In this pilot study, hospice IDT members had low levels of well-being at baseline that worsened over 3-months indicating a higher potential risk for burnout. Moreover, given the COVID-19 pandemic, this may be an ominous sign of what lies ahead for hospice providers regarding turnover, leading to significant long-term staffing problems in the field. If these results hold true in a larger sample, it could necessitate developing and testing further strategies to ensure a healthy and stable workforce.
Keywords
Introduction
The complexity of care has increased substantially in hospice over the past 15 years due to demographic and clinical changes, i.e. the increased rates of non-cancer diagnoses 1 and changes in hospice referral patterns. 2 This increase in care complexity is primarily due to increased longevity and presence of multiple chronic conditions among Americans, and the fact that hospices are expanding care beyond their original focus on caring for individuals with cancer at the end of life. For example, in 2018 cancer represented the highest single primary diagnosis comprising 27.2% of Medicare hospice patients; however, the next highest diagnostic groups were cardiovascular disease and dementia, representing a combined 36.7% of the hospice population. 2 Even before the COVID-19 pandemic added an additional layer of burden to hospice workers, as a result of the changing work environment in hospice care, these individuals were at risk for burnout, poor well-being, and job turnover.
Burnout, a subcategory of professional quality of life, is defined as emotional exhaustion, cynicism, and professional inefficacy 3 and may be especially problematic due to the complexity of care and compassion needs in hospice. The gold standard in measuring burnout was defined by Maslach and colleagues including 3 subscales: high emotional exhaustion, depersonalization, and low personal accomplishment. 4 A review of research studies examining professional quality of life in hospice and palliative care staff showed that they experience increased rates of suicidal ideation, burnout and stress as well as increased use in alcohol and drugs, anxiety, depression and decreases in compassion satisfaction as well as struggle in dealing with death and dying, compared to professionals in many other settings. 5
Turnover can be described by a healthcare delivery organization as an event where an employee leaves their position. There are significant costs to agencies in replacing staff when turnover occurs, and hospices already experience a deficit in trained staff members.6-8 High turnover can lead to inadequate staffing resulting in decreasing quality of care, which results in a vicious cycle of higher rates of burnout and turnover.9,10 In addition to costs, burnout and turnover are of significant concern for both health professionals’ well-being and patient outcomes.11-14 Multiple studies have shown that turnover rates and burnout can be detrimental to patient outcomes in other settings, particularly care quality15-17 and patient safety.18,19
High rates of burnout and poor well-being in hospice and palliative care are related to issues such as the need for advanced technical knowledge, involvements in ethical decision making, and the frequency with which they encounter suffering and death. 20 Research demonstrates burnout is not being resolved. Burnout amongst physicians has increased by 10% from 2011 to 2014,21,22 and is especially problematic for palliative care clinicians.
Given the nature of hospice and palliative care services, members of an interdisciplinary team (IDT) including social workers, nurses, nursing aides, chaplains, and physicians are routinely exposed to end-of-life experiences, patient and family suffering, and may therefore be especially vulnerable to poor well-being outcomes, and turnover intention. Burnout is especially high among those nurses, social workers, and physicians working in home hospice settings versus hospice inpatient settings. 23 Burnout is prevalent across hospice and palliative care clinicians,11-14 with some rates of burnout reported as high as 62%. 15 A recent systematic review established that 27% of social workers demonstrated burnout, while 15.1% of physicians and 18.6% of nurses experienced burnout. 20
However, limited work has compared the change of well-being, and turnover intent amongst an IDT of hospice workers at baseline and at 3-months. The body of literature discussing hospice workers uses multiple terms to address quality of life or well-being at work. Burnout is one term used to describe a negative outcome associated with well-being or a lack thereof in the measurements utilized in this study. This paper is specifically addressing health and wellness from a career standpoint. When well-being is discussed in relation to the careers of health worker it can be used interchangeably with or also described as Professional Quality of Life. While multiple studies examine elements of well-being among palliative care and hospice clinicians11,15,21 a lack of research exists that examines nurses, social workers and chaplains as part of the IDT, who are a crucial part of the workforce that jointly are responsible for outcomes produced in hospice care settings. This pilot study took an innovative approach to examining feasibility of implementing instruments measuring well-being and turnover in a hospice IDT, i.e. chaplains, nurses, social workers, home health aides (HHAs), and physicians5,23 as part of a pilot for a larger embedded pragmatic clinical trial in hospice.
Methods
Research Design
This pilot observational study utilized a longitudinal survey design, describing well-being of hospice workers at 2 points in time, to assess the feasibility of inserting measures of well-being in hospice IDTs into the parent trial. Quantitative survey instruments examining well-being, and turnover intentions were administered to hospice IDT members.
Sample and Setting
Sample
A sample size of hospice IDT members was used to do the final analyses. This IDT included registered nurses, social workers, chaplains, HHAs, and physicians.
Recruitment and Incentivization
Participants were recruited from a a single hospice in southern California in the Phase I Exploratory/Developmental stage for an embedded pragmatic clinical trial that examined the effectiveness of the Aliviado Dementia Care program on dementia symptom management of an interdisciplinary hospice workforce. 24
Those who participated in the Aliviado Dementia Care program were asked to complete an optional survey on professional quality of life. Participants were incentivized by mailing them a $25 gift card upon completion of the surveys. This study was approved by the NYU School of Medicine Institutional Review Board. IRB approved waiver of consent for participants. Surveys were voluntary and a heading was including prior to accessing the survey for the study.
Instruments
Demographic measures were collected including age, ethnicity, sex, years of experience, marital status, number of dependents, and employment status. Professional quality of life, well-being, and turnover intent were measured using valid and reliable instruments, including: Professional Quality of Life (ProQOL-5), 25 9-item Well-being Index (WBI),26,27 and one question about employee turnover asking participants whether they are planning to continue working for their employer in the coming year.
The WBI is a validated screening tool used for several clinician populations (e.g. nurses, physicians) and the general working population. The WBI includes 9 questions spanning domains of fatigue, burnout, depression, anxiety, and mental and physical quality of life. WBI scores each question that was answered yes as a point, except the eighth and ninth question. The eighth and ninth question is given -1, 0 or 1 point depending the score picked on the seven-point Likert score. Individuals that score 1.2 or greater are at risk of distress contributing to a personal or professional consequence according to the well-being index. Additionally, individuals that score 2 or greater are considered at a greater risk of distress contributing to a personal or professional consequence. The greater the score the greater the risk of poor well-being.26,27
The ProQOL tool consists of 30 questions that are answered on five-point Likert scales. These questions are grouped into 3 subscales: compassion satisfaction (a = .90), burnout (a = .80), and secondary traumatic stress (a = .84). 28 Compassion satisfaction is the pleasure a person gets from being able to do their work well and helping others. Burnout is a person’s level of hopelessness, unhappiness, being overwhelmed and bogged down and difficulties dealing with work. Secondary traumatic stress is an element of compassion fatigue characterized by being preoccupied with thoughts of people one has helped and caregivers report of feeling trapped on edge, overwhelmed and infected by other’s trauma. 25 For each category, a score of 22 or less is considered low, between 23 and 41 is considered moderate, 42 or more is considered a high level well-being on the ProQOL tool. 25 Psychometric validation deeming the ProQOL tool a valid and reliable tool to test compassion satisfaction, compassion fatigue and burnout has been shown by multiple studies.29,30
Procedure
For this pilot observational study, we described rates of professional quality of life, well-being, and turnover intent of hospice IDT members at 2 points in time; at baseline and 3 months later. Participants were recruited from an IDT undergoing a quality improvement program, Aliviado Dementia Care-Hospice Edition, in the complexities of providing dementia care in the hospice setting. 31 Methodology from this study are reported in greater detail elsewhere. 31 Participants were invited to complete the survey after completion of the dementia care training of the Aliviado program. All data was collected between March and September 2019.
Demographics, ProQOL, well-being and turnover intentions were collected. After 3 months, a follow up survey was collected. The response rate was 100% (N = 25) at baseline and was 70% (N = 17) at the 3-month follow-up. Descriptive and frequency analyses were run to assess the demographic information of the IDT members. Percent change was calculated to compare the baseline differences of the IDT members’ WBI and ProQOL tool scores by disciplines, if they have dependents, and by response to follow up to further assess the sample’s characteristics. T-tests were run for normally distributed data, which included all the ProQOL tool scores subgroups and WBI scores by discipline and response to follow up to assess significance of differences at baseline. Wilcoxon signed-rank test was run to assess significance for WBI baseline scores by dependents since this subgroup was not normally distributed. Paired sample t-tests and percent change were calculated using participants that responded to quantify the differences and significance of the IDT members’ WBI and ProQOL tool scores at baseline and at the 3-month follow-up period with participants that responded at both baseline and follow up. RStudio 1.1.456 statistical software was used for analysis. A p-value of 0.05 or lower is seen as statistically significant.
Results
Participants eagerly welcomed consideration of their well-being. All (n = 25) participants invited completed the first survey and 68% (n = 17) completed the follow up survey. No participants reported any distress or other challenges in completing the survey.
The IDT members were on average 51.7 (SD = 10.6) years old and mostly female (80.0%). A racially/ethnically diverse sample (48% non-white participant base) was enrolled. Full demographics are displayed in Table 1.
Demographic and Work Characteristics of the IDT Sample.
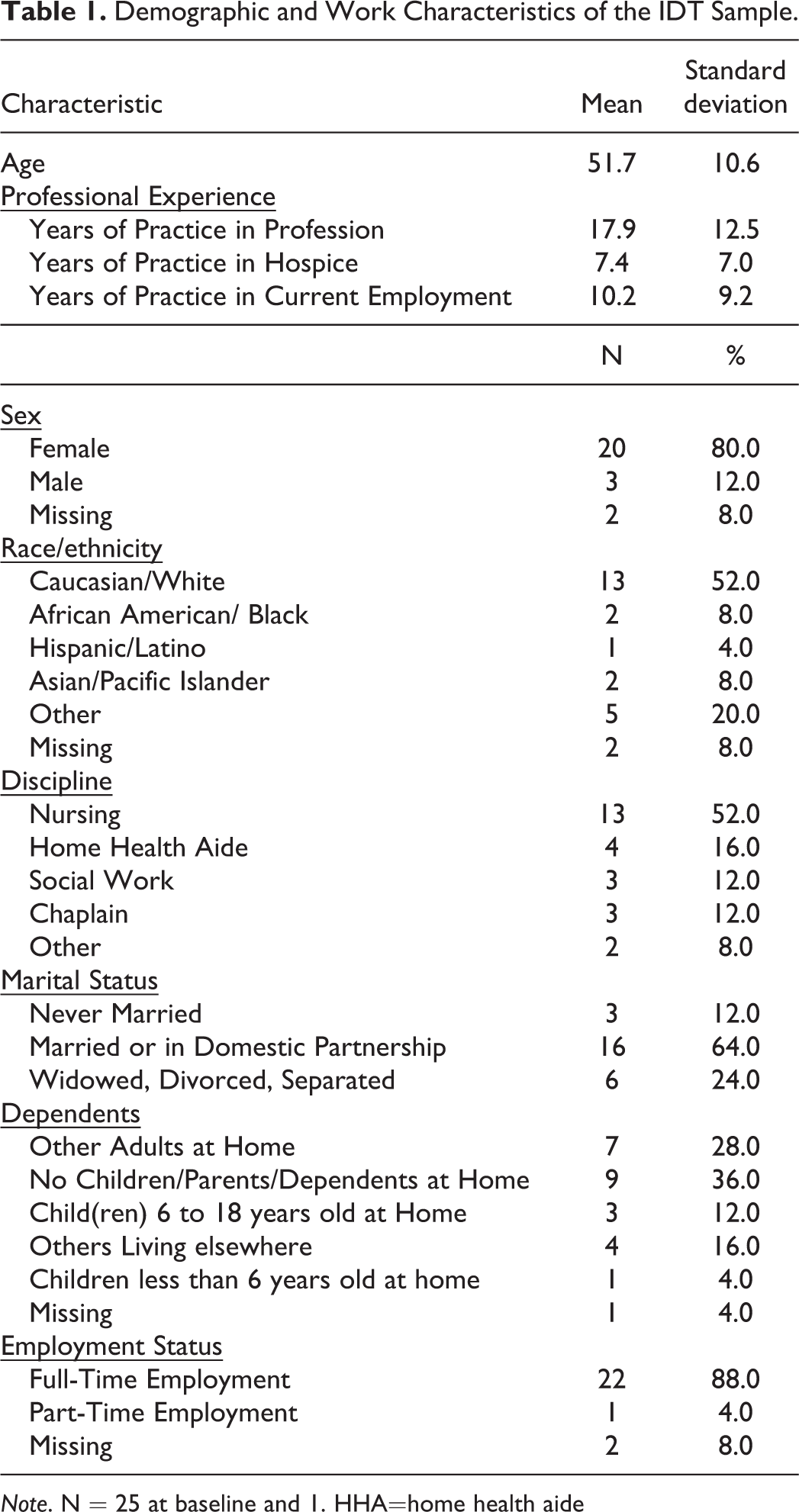
Note. N = 25 at baseline and 1. HHA=home health aide
At baseline, there were no significant differences in WBI and ProQOL scores across disciplines and between IDT members that had dependents versus members that did not. Status of participant’s dependents was examined due to the extension of caregiving burden/strain to the home setting for individuals who already occupy jobs that are intensive caregiving. There were also no significant differences between IDT members that followed-up after 3 months and members that did not (not shown).
When assessing the differences from baseline to follow-up of the overall sample, there was no significant increase in the WBI score of the IDT members from their baseline score. The ProQOL scores reflected low burnout and secondary traumatic stress and high compassion satisfaction levels at baseline. At follow-up, there was a significant, though modest, reduction in compassion satisfaction (-3.5%, p = 0.05) and a significant decrease in secondary trauma stress (-31.7%, p = <0.001) (Table 2). At baseline, no individuals intended to leave their current employer in 1 year, and at follow-up 1 (5.9%) individual expressed intent to leave and 1 individual had actually left the organization (not shown).
Paired Sample T-test of Baseline and 3 Months Follow Up Well-being Index and PROQOL-5 Scores.
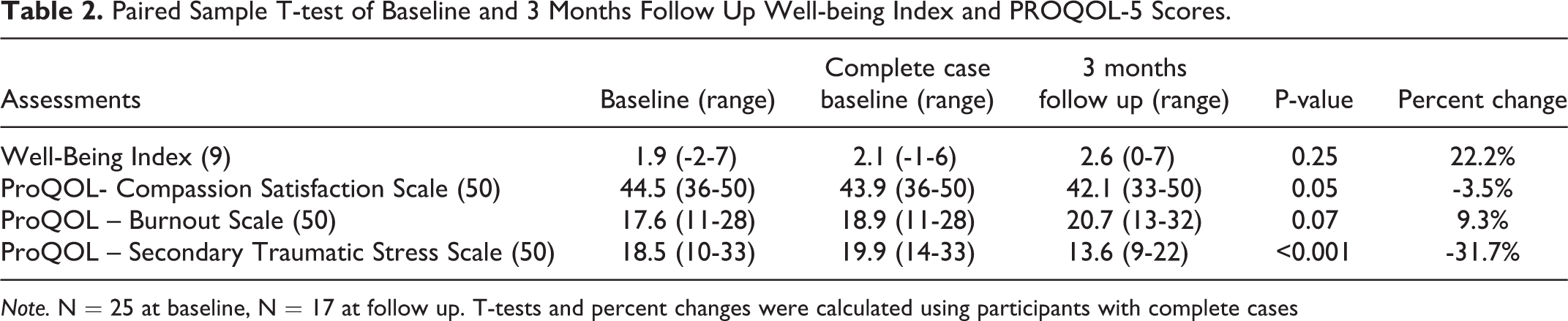
Note. N = 25 at baseline, N = 17 at follow up. T-tests and percent changes were calculated using participants with complete cases
Discussion
The results of this study demonstrate hospice team members’ interest and engagement with evaluation of professional work and well-being, and feasibility of collection. For this pilot study, the high level of participant engagement supports further exploration of the concept of well-being in future work. Moreover, the results provide a preliminary understanding of well-being, and turnover intentions in hospice IDT members at a single site. This is the first study to examine well-being and turnover in hospice IDT members, which demonstrated low baseline scores in WBI and high potential for future burnout and decreased compassion satisfaction. Participants in this study demonstrated significant decreases in compassion satisfaction. On the other hand, secondary traumatic stress levels decreased from baseline to 3-month follow up. IDT members demonstrated low baseline WBI scores, with the majority representing being at-risk of distress at baseline. However, low levels of intended turnover were found. Instead, a high percentage of IDT participants identified intentions to stay at their current place of employment. Thus, it is unclear if there is high variability from time to time in the instrument measures due to the nature of hospice practice, or if intention to stay at current place of employment is due to their dedication to the specialized care they provide regardless of the distress and burnout it causes.
Hospice staffing is already challenging in many cases due to a variety of labor market and professional issues, and nationally in the United States, hospice nursing staff turnover at an annual rate is 19%.8,32 These staffing issues present a substantial service delivery threat to hospice agencies, as well as substantial costs for recruiting, hiring, and training replacements. 33 Thus, further work is needed on determining factors affecting burnout and turnover specific to this setting as well as targeted interventions to address the factors found. Existing studies do not examine the linkage between burnout and turnover and do not look at professional quality of life. Moreover, they are modestly conflicting, likely because of sample concerns or focusing on only a single discipline. For example, one multi-site study of 181 hospice nurses found low levels of burnout, 34 measured by the ProQOL. In another study of mostly palliative care physicians in academic medicine or hybrid practice (73.6%), not hospice practice, 18.2% of respondents met the criteria for burnout and 16.6% presenting with high emotional exhaustion. However, a low response rate of 15% must be considered when interpreting these findings. 35 Neither study linked burnout with turnover. Moreover, differences in how workers in traditional hospice care programs perform their work versus those in more varied other forms of palliative care (e.g. inpatient, outpatient, home-based, telephonic) may support understanding of the differences reported in levels of burnout between these delivery models.
Furthermore, workload represents a key influence on the level of an individual’s stress, which may then subsequently impact reported well-being. 34 For example, IDT members may be responsible for a high number of cases. Additionally, IDT members may be required to provide care to individuals in various stages of the end-of-life trajectory, increasing the difficulty of providing appropriate care. 34 Changing patient loads and greater variation in the types of patients seen may contribute to increased workload perceptions and burnout. 36 Additionally, a lack of interaction among colleagues and increased work requirements during weekends have demonstrated increased rates of burnout. 35 While not measured in this study understanding the influence of workload on burnout and well-being represents a key future consideration in continuing to explore the concept of well-being in hospice and palliative care.
While half of the well-being measures worsened (burnout and well-being), including compassion satisfaction, secondary trauma improved over the 3-month follow-up. This improvement may of occurred and been influenced by the number of dependents a participant had and hours they cared for them. This could be a determent of this finding because caregiver responsibilities do not end for those with dependents when they return home after work, therefore respite and reprieve of stress caused by job demands is never accomplished. Although if number of dependent went down or if status of having a dependent in general (i.e. older parent) was removed secondary trauma scores could have improved. This specific finding needs to be investigated in future studies.
Finally, as noted in a recent National Academies of Science, Engineering and Medicine report, the healthcare worker workforce is aging, raising significant concerns for the ability to staff hospices 37 effectively within the next 5-15 years. Although this study was conducted preceding the COVID-19 pandemic the concern is exacerbated by the pandemic, where a scoping review has already found 37 studies indicating increasing stress, anxiety and depressive symptoms amongst healthcare workers, 38 and anecdotally reported by hospice executives of substantial staffing challenges. 38
Limitations
This research was a pilot study in a medium sized hospice serving urban and suburban patients, and thus provides preliminary consideration of well-being in hospice IDTs. Further research is needed to explore well-being across different hospices with greater variation over longer periods of time so that we can explore relationships between well-being, turnover intent, and turnover. The majority of respondents were nurses, limiting understanding of the broader IDT experience in hospice; however, nurses are the largest group of hospice providers. Proportionally, it is expected that there would be a greater number of nurses than other IDT members. Finally, we only examined the outcome at baseline and 3 months, and further work is needed in a longitudinal pattern to understand the effects over time.
Conclusion and Future Directions
Understanding well-being in hospice IDT members represents a key concern for the promotion of high-quality care for seriously ill individuals receiving hospice. Recognition of the factors, such as burnout and turnover, relating to care in hospice settings may support the development of interventions specific to the setting to ensure IDT member wellness. Further research is needed to continue to understand well-being in larger sample sizes as well as over a longer time frame, which is currently being conducted as part of the National Institutes of Health/National Institute on Aging funded 25-site Hospice Advanced Dementia and Symptom Management Quality of Life stepped wedge trial (NCT04175977).
Footnotes
Authors’ Note
This clinical trial is registered at NCT03681119.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by National Institutes of Health/National Institute on Aging grant R33AG061904.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.