
Abstract
Background:
A critical aspect of pediatric palliative care consultations is the assessment and documentation of patient and family needs. While these assessments usually include a focus on physical pain, there is less standardization of assessments of other physical symptoms and psychosocial, emotional, or spiritual needs.
Aims:
To improve the breadth of assessment of psychosocial and emotional needs, screen for symptoms other than pain among pediatric patients utilizing palliative care services, and to increase documentation of assessment data from 30%-40% to 80% through practice changes implemented in 2 Plan-Do-Study-Act (PDSA) cycles.
Methods:
This quality improvement project involved implementing provider education and adapting the palliative care consultation template in the electronic health record to improve breadth and consistency of assessment and documentation during consultations by the interdisciplinary pediatric palliative care team. Two PDSA cycles were performed. Chi squared tests and statistical control charts were used for data analysis.
Results:
There was statistically significant improvement in the inclusion of documentation of a pediatric palliative care social work note from baseline (32%) to Cycle 2 (57%). Physical symptom screening declined slightly, but not significantly (p = .32) and socio-emotional discussions also declined but not significantly (p = .05).
Conclusions:
Screening for physical symptoms and discussions with patients and families about psychosocial/emotional needs during the initial palliative care consultations are extremely important in providing effective, holistic, patient-centered care. There is a need for development of pediatric-centric guidelines and quality measures to evaluate pediatric palliative care programs; further research is indicated to determine methods for evaluating compliance with these guidelines.
Keywords
Introduction
Problem Description
It is widely accepted that pediatric palliative care improves outcomes for patients and families,1-3 and has been declared by the World Health Organization (WHO) to be a moral duty of hospital systems. 3 However, integration of these services into the fast-paced environment of acute care continues to be met with both system and process barriers,4,5 and can be described as inconsistent and often incomplete. 1 One area of pediatric palliative care integration that is feasible for intervention is consistent assessment and documentation of patient and family palliative care needs by the palliative care specialists. There are known gaps in specific domains of palliative care services, such as assessing emotional and social needs, and managing pain and other physical symptoms. 6 During palliative care consultations, the presence of physical pain is often well assessed, yet many other physical, emotional, psychological, spiritual, and social dimensions associated with pain and suffering that make up the concept of “total pain” 7 are overlooked or poorly assessed.6,8 This could be due to many factors including the amount of time allotted for the interview, the clinical condition of the patient, and consistency in assessment and documentation of needs. To relieve suffering, the goal of palliative care, it is essential to assess both pain and other aspects of physical and psychosocial distress beginning with the initial consultation. Gaps in thorough assessment and the documentation of findings must be identified and targeted for improvement to enhance quality of care for pediatric patients and their families.
Rationale
In 2000, the American Academy of Pediatrics (AAP) released a statement saying, “Excellence in pediatric palliative care is essential for hospitals and other facilities caring for children.” 9 Early implementation of palliative care services leads to improvement in patient quality of life, mood, symptom management, outcomes of end-of-life care, and access to resources, in addition to decreasing the psychological burden on caregivers. 10 Parents report that involvement of a palliative care team in their child’s care improves the quality of life of both child and parent, 11 and health care professionals also report improved cooperation, communication, and family support when palliative care services are implemented. 1 Additional evidence suggests involvement of a pediatric palliative care program decreases hospital admissions and length of stay during admissions for children with potentially life-limiting illnesses. 12 Furthermore, the Institute of Medicine (IOM) has discussed at length the importance of attending to the emotional and spiritual concerns of children and families while also controlling physical symptoms and easing suffering. 13
The World Health Organization recommends initiation of palliative care services at the time of diagnosis for all patients with serious life-limiting illnesses. 14 These services can and should be implemented to decrease suffering and improve well-being for patients with life-limiting illnesses despite the status of the patient’s disease.9,15 Unlike many medical interventions and services, palliative care not only targets the patient but also provides care and resources for clinicians, family members, and other individuals and groups who play a formative role in the patient’s life. 15 This is particularly true for pediatric patients who often have parents and siblings uniquely affected by their illness, 16 and typically have a larger group of caregivers and family members directly affected by their situation compared to adult patients. 17
Implementing palliative care services early in the disease trajectory as a standard of care provides many opportunities to improve quality of life and symptom management for children and their families.15,18 While utilization of pediatric palliative care services has increased and continues to become more consistent in clinical practice over recent decades, many aspects of palliative care such as psychosocial and religious/spiritual implications of life-limiting illnesses are poorly addressed in medical and nursing education leaving novice healthcare providers with limited knowledge and experience to provide comprehensive and effective care for children with painful, chronic or life-threatening illnesses. 19 Studies show that healthcare providers frequently assess for and document symptoms such as physical pain and pain management, but spiritual and emotional symptoms and other psychosocial concerns are missed during comprehensive assessments or undocumented. 20
Current measures used to assess quality of palliative care services in pediatric acute care largely focus on end-of-life care rather than addressing palliative care from diagnosis through natural death, 21 and data on the effectiveness of these quality indicators are limited. 22 Through the Measuring What Matters (MWM) project, the American Academy of Hospice and Palliative Medicine (AAHPM) and the Hospice and Palliative Nurses Association (HPNA) cultivated a list of 10 valid, clinically relevant quality indicators useful for internal review of adult palliative care programs that could be used to create national standards for benchmarking these programs across the United States. 6 These quality indicators are particularly helpful for assessing the components of a palliative care patient encounter in the clinical environment 23 ; however, pediatric palliative care programs differ from adult programs in fundamental ways, 16 so these indicators must be adapted in order to assess and improve the quality of care quality in a pediatric setting. 24 A crucial initial step toward improving the quality of a palliative care service program is to discover where deficits exist compared to existing quality standards to determine targets for improvement. 6
Specific Aims
This quality improvement project was designed to assess effectiveness of an established pediatric palliative care consultation process. We used 2 Plan-Do-Study-Act (PDSA) cycles and evaluated the results to assess for areas of improvement and implement changes to enhance processes and patient outcomes. The Plan-Do-Study-Act Model is used by the Institute of Healthcare Improvement to assess changes in the healthcare setting by creating a plan to test the changes made (Plan), completing the test (Do), evaluating the results (Study), and making the decision to adapt or abort the change pending these results (Act). 25 The primary aim was to improve the breadth of assessment and documentation of psychosocial and emotional needs, and expand screening for symptoms other than pain among patients and families in a pediatric palliative care service. Our aim included increasing the documentation of findings from 30-40% to 80% through practice changes implemented in each PDSA cycle.
The first practice change included standardized in-person education for providers conducting palliative care consultations and implementing an email reminder system to emphasize the importance of screening for the selected indicators; the second practice change focused on improving the electronic medical record (EMR) template for the consultation note to increase consistency in documentation. The aim of this data analysis was to determine if the quality improvement practice changes, performed after 2 PDSA cycles, resulted in improvement in documentation of psychosocial and emotional needs and physical symptoms other than pain.
Methods
Context
The setting for this QI project was the pediatric units in a private academic medical center in the southeastern United States. The interdisciplinary pediatric palliative care team typically includes 3 medical doctors (MD) who alternate coverage of the pediatric palliative care service, as well as 1 pediatric nurse practitioner (PNP) and 1 clinical social worker (CSW) who are both dedicated to the pediatric palliative care service. The pediatric palliative care team has been functioning in this institution for 10 years and typically performs over 200 consultations annually. This QI was exempt from Institutional Review Board approval. Based on the evaluation of 3 months of baseline data from initial pediatric palliative care consultation notes completed by providers on the pediatric palliative care team, 2 MWM Quality Indicators were chosen as a focus for improvement: Screening for Physical Symptoms and Discussion of Emotional or Psychological Needs. These quality indicators were chosen as, according to the preliminary review, screening for physical symptoms other than pain only occurred 30-40% of the time during initial consultations, and discussion of emotional and social needs with patients over 2 years old only occurred 40% of the time.
Intervention
Baseline data were collected from 3 months of retrospective chart reviews. Two PDSA cycles were conducted. In the first cycle, the pediatric palliative care team reviewed baseline data from 3 months of retrospective chart reviews, received education regarding the importance of assessing and documenting these palliative care need indicators (physical symptoms other than pain, and a discussion of psychosocial/emotional needs), and were provided monthly reminders to conduct high quality consultations. Additionally, a system was put into place to standardize the process of communicating incomplete assessments within the pediatric palliative care team to improve follow up evaluations. In cycle 2, the template for the pediatric palliative care consultation in the EMR was adjusted to make documentation of the assessment of social and emotional distress and symptoms other than pain more straightforward. The updated template encouraged comprehensive symptom screening by creating shortcuts for automatic phrases to ease provider documentation. Data was collected after each cycle via retrospective chart reviews.
Baseline Assessment
Initially, data were collected to evaluate documentation in pediatric palliative care initial consultations. Charts were reviewed from 43 hospital admissions with 40 unique patients (consultations taking place between 2/08/2019 and 5/29/2019). The data included the assessment of pain and other physical symptoms (nausea/vomiting, dyspnea/shortness of breath, constipation, diarrhea, and agitation/fussiness), and documentation of a discussion held regarding psychological and emotional needs, with whom it was discussed (patient, family/caregiver, or both), and whether or not there was a progress note documented by the pediatric palliative care social worker. Data on patient characteristics were also collected (patient age, gender, ethnicity, technology dependence, and length of stay). Figure 1 outlines the timeline of the project.
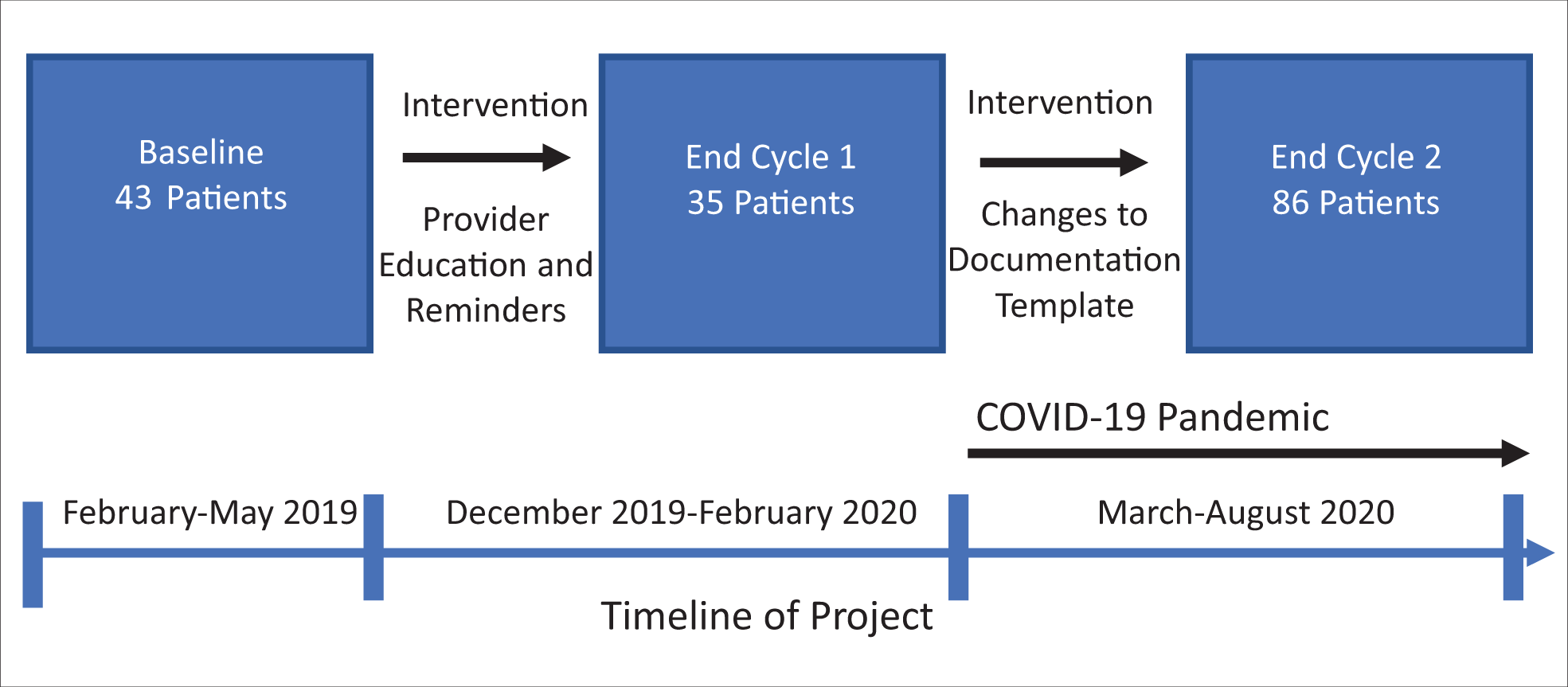
Timeline of project.
Post-Intervention Assessment
Similar data were collected after each PDSA cycle. After the first cycle, lasting 3 months, 35 charts were eligible for review. Cycle 2 data collection was extended to 6 months due to changes in the composition of the pediatric palliative care team, availability of team members in the hospital to conduct consultations, and other changes in hospital policies and procedures related to the novel coronavirus pandemic. After the second cycle, 86 charts were reviewed. Patient characteristics were also recorded for each patient in these cycles. Documentation on individual physical symptoms, inclusion of a pediatric palliative care social work note, and discussions of psychosocial and emotional needs was evaluated across all 14 months (3 months of baseline data, 3 months of Cycle 1 data, and 6 months of Cycle 2 data) and are displayed in Figures 2–11.
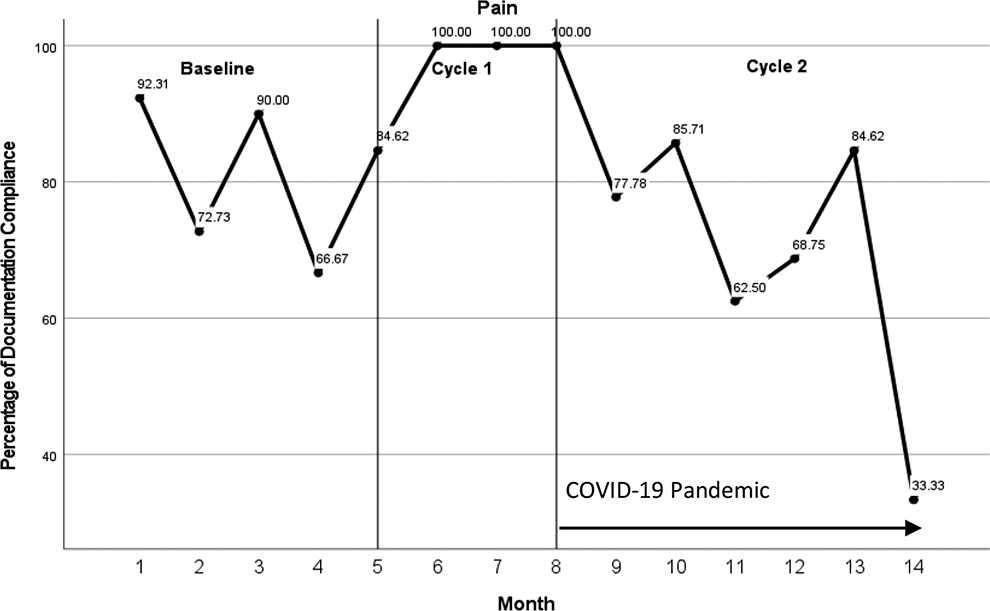
Pain consult documentation.
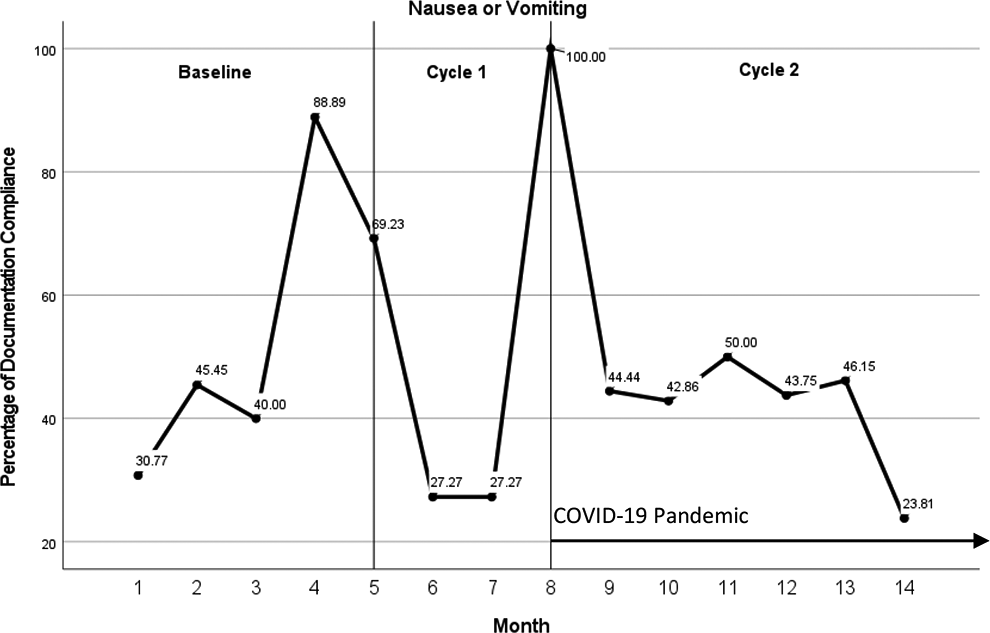
Nausea/vomiting consult documentation.
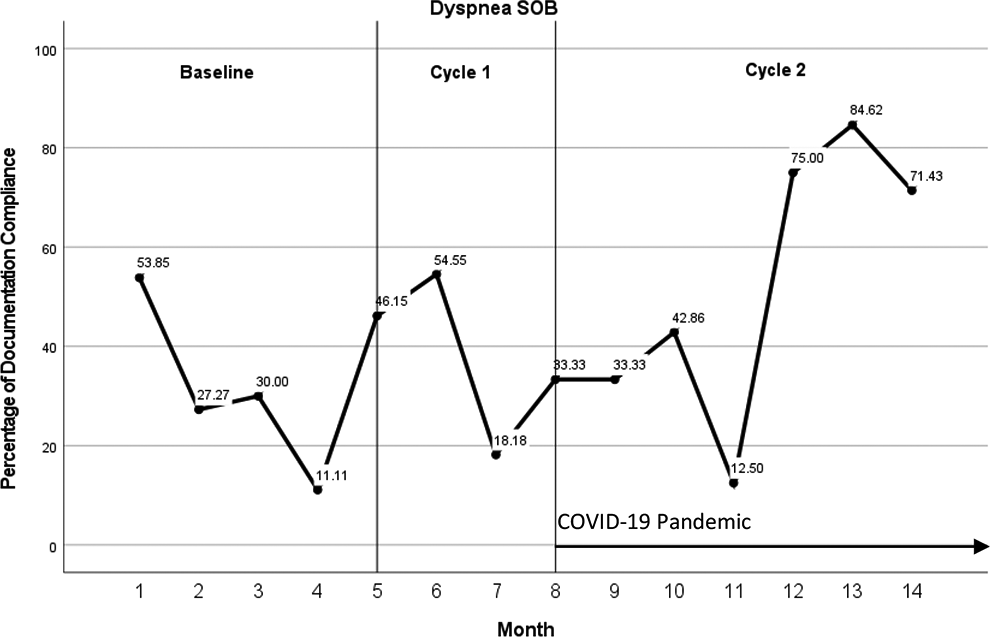
Dyspnea/shortness of breath consult documentation.
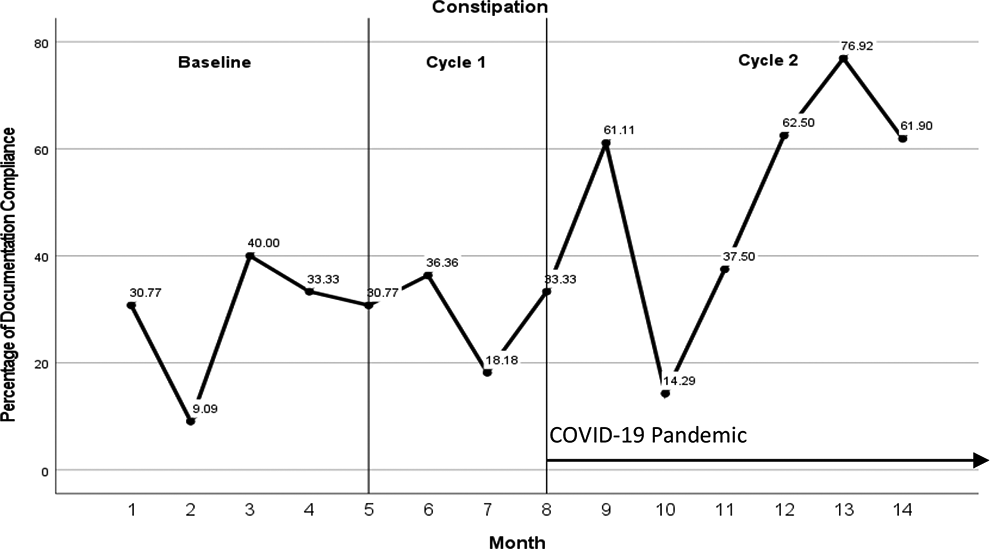
Constipation/shortness of breath consult documenation.
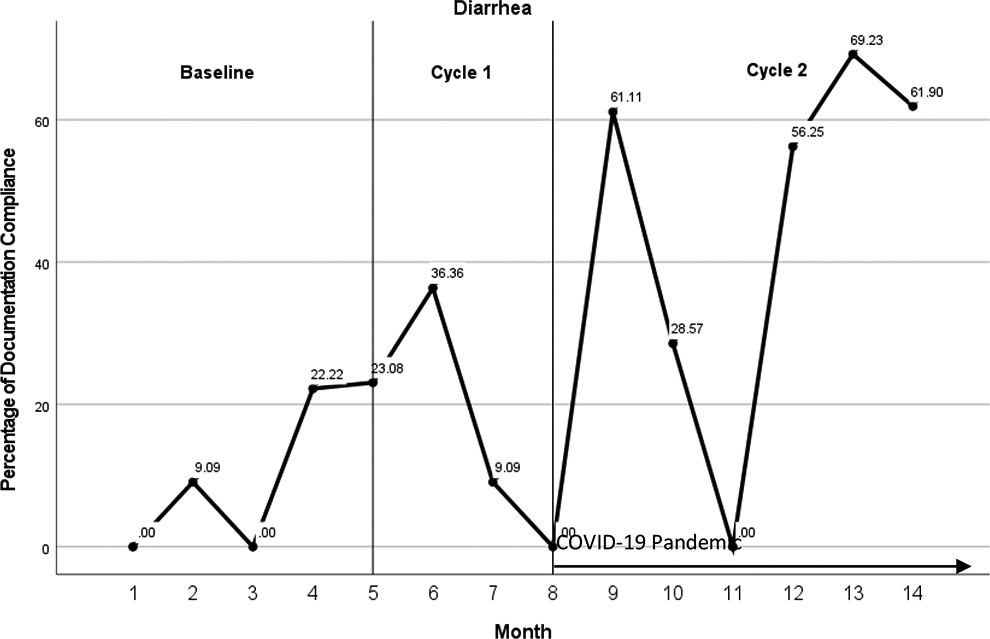
Diarrhea consult documentation.
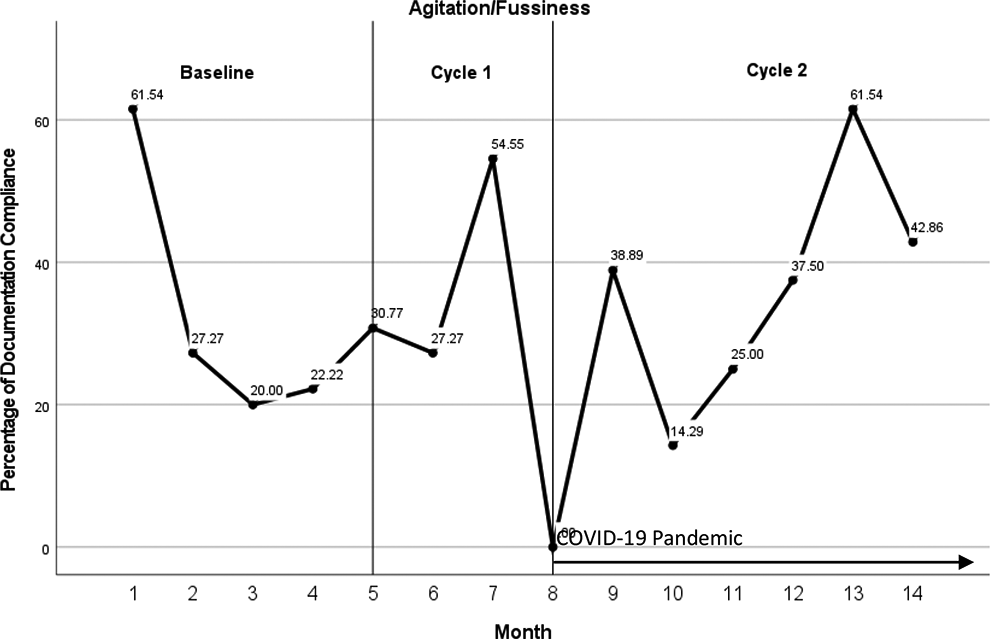
Agitation/fussiness consult documentation.
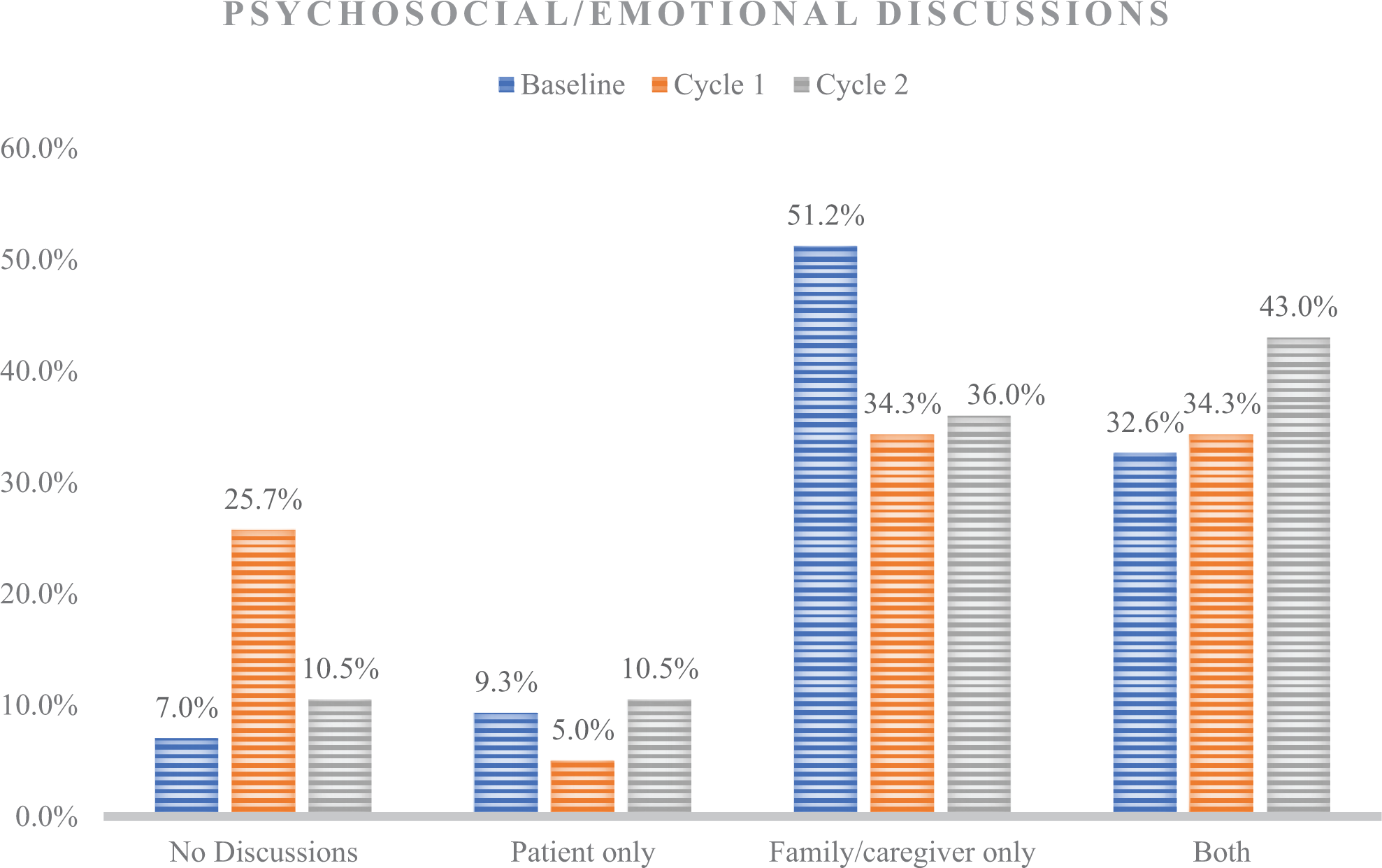
Psychosocial/emotional discussions at Baseline, Cycle 1, and Cycle 2.
Patient psychosocial/emotional distress consult documentation.
Caregiver/family psychosocial/emotional distress consult documentation.
Patient and caregiver/family psychosocial/emotional distress consult documentation.
Evaluation Plan
Descriptive statistics (Mean, SD or n, %) were computed for demographic variables including patient age, sex, race, ethnicity, technology use, and length of hospital stay. Documentation of screening for physical symptoms including pain, nausea/vomiting, dyspnea/shortness of breath (SOB), constipation, diarrhea, and agitation/fussiness and discussion of psychological or emotional symptoms were assessed through retrospective chart analyses and coded as a binary outcome (Yes/No). A series of Chi square tests were performed to compare the proportion of documentation between baseline, Cycle 1 and Cycle 2. Statistical control charts (p-charts), which are graphs designed to show how processes change over time, were displayed across all 3 cycles for each binary documentation outcome to look for patterns in the way each assessment was documented throughout the project. Data were aggregated and analyzed using IBM SPSS version 26.
Results
Patient Demographic and Clinical Characteristics
A total of 164 patients were included in this quality improvement project. Demographic and clinical characteristics are displayed in Table 1 computed using descriptive statistics. Most patients were female in the baseline and cycle 1 assessments, but not cycle 2 (44%). Race was reported to be Caucasian/White for over 50% of the patients in all 3 PDSA cycles and ethnicity was Not Hispanic/Latino for over 70% of the patients in all 3 PDSA cycles. Inpatient length of stay (LOS) was highest for baseline (average of 37 days) and lowest for Cycle 1 (average of 26 days). Evaluation of technology use by patients showed that feeding tubes were the most common type of technology in use by patients, with 33% at baseline, 43% at cycle 1, and 45% at cycle 2. Extracorporeal membrane oxygenation (ECMO) was the least common technology in use, with 5% of patients on ECMO at baseline, 0% at cycle 1, and 1% at cycle 2.
Patient Demographics and Clinical Characteristics.
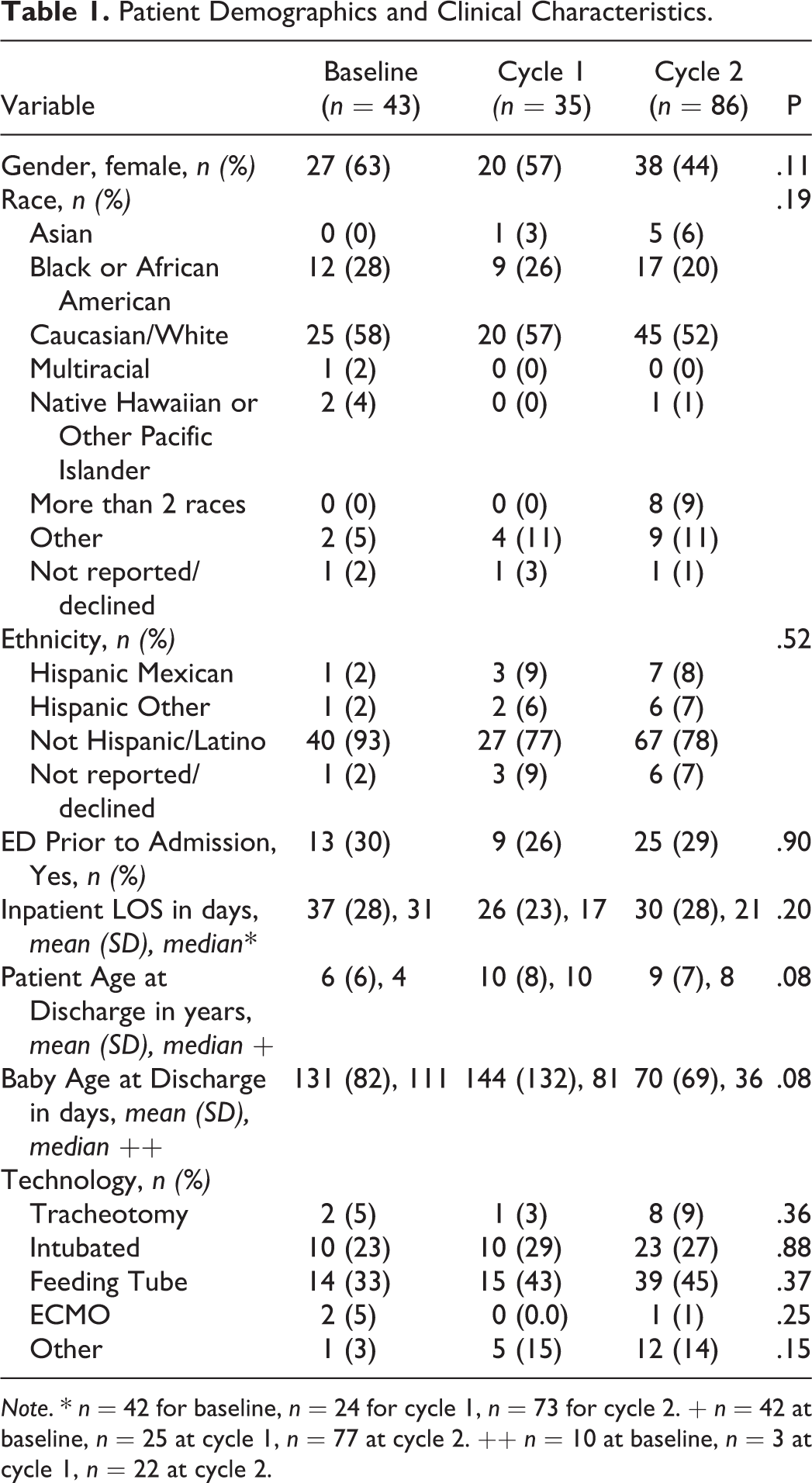
Note. * n = 42 for baseline, n = 24 for cycle 1, n = 73 for cycle 2. + n = 42 at baseline, n = 25 at cycle 1, n = 77 at cycle 2. ++ n = 10 at baseline, n = 3 at cycle 1, n = 22 at cycle 2.
To examine improved consistency in documentation, 2 types of analyses were conducted. First, run charts were plotted monthly and for each PDSA cycle to display the percentage of records with documentation on specific physical, and emotional/psychosocial elements. Second, Chi square tests were conducted to compare the percentage of compliance across each PDSA cycle.
Physical symptoms
Figure 2 displays results for assessment and documentation of pain. As shown, compliance with pain peaked during Cycle 1 with rates above 80% for Months 5-8. During Cycle 2, the compliance decreased to levels similar to baseline.
Figure 3 displays results for assessment and documentation of nausea/vomiting. The peak rate occurred during the first month of Cycle 2 (Month 8) at 100%. Only one other time period (Baseline, Month 4) exceeded 80%.
Figure 4 displays results for assessment and documentation of dyspnea (shortness of breath). As shown, Cycle 2 yielded the highest consult documentation rates with a peak at Month 13 (84%).
Assessment and documentation regarding constipation improved over time as shown in Figure 5. The 4 highest documentation rates occurred during Cycle 2, with a peak during Month 13 (76%).
Figure 6 shows the results for assessment and documentation of diarrhea. Cycle 2 yielded the highest rates of consult documentation, with the peak rate occurring during Month 13 at 69%. There were 3 months in Cycle 2 that showed consult documentation exceeded 60%.
Figure 7 shows the results for assessment and documentation of agitation/fussiness. The first measurement month (Month 1, baseline) was a peak rate 61% which also occurred during Cycle 2, Month 13.
Psychosocial/emotional discussions
For psychosocial/emotional discussions the project assessed whether the discussion was held with the patient, caregiver/family, or both. The percentage of records with patient only, caregiver/family only, and both were calculated for each cycle and compared using a chi square test. There were no statistically significant differences between cycles on documentation of discussions, X2 (6, N = 164) = 9.67, p = .139. There was improvement for discussions with the patient only from baseline (4, 9%) to Cycle 2 (n = 9, 11%). Discussions with both patients and family/caregivers also improved from baseline (n = 14, 33%) to Cycle 2 (n = 37, 43%). Discussions with caregiver/family only decreased from baseline (n = 22, 51%) to Cycle 2 (n = 31, 36%). Figure 8 displays the psychosocial/emotional discussion results for each cycle.
Another exploratory analysis was conducted to examine patients that are younger than 2 years old compared to those that are 2 years of age and older. There were 62 patients younger than 2 years of age and 102 patients who were 2 years of age or older. Table 2 below shows the percentage of psychosocial/emotional discussions with patients <2 years old compared to patients that were ≥2 years old across the 3 cycles. There was a significant increase from Cycle 1 (55%) to Cycle 2 (89%) in discussions for children less than 2 years old, although those were less than the baseline percentage of discussion of 93 (p = .014). For those less than 2 years old, the discussions with patients and both patients/family did not have significant differences. For discussions with caregiver/family, they declined from baseline (93%) to Cycle 1 (55%), which was not significant. They improved from Cycle 1 to Cycle 2 (87%), which was statistically significant (p = .03).
Psychosocial/Emotional Discussions According to Age Group.
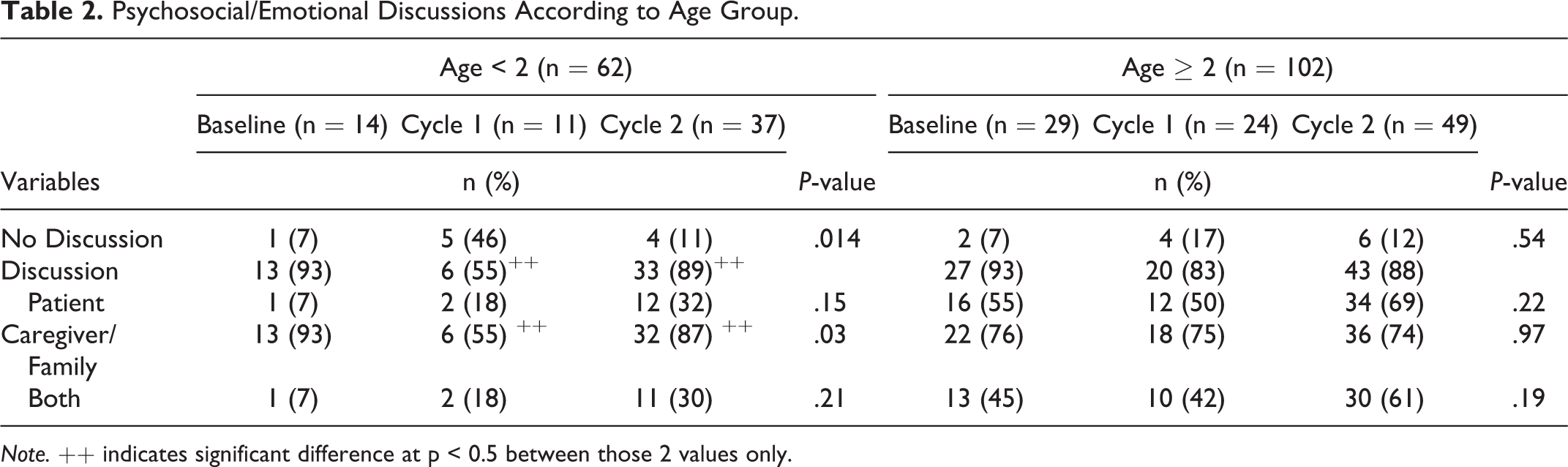
Note. ++ indicates significant difference at p < 0.5 between those 2 values only.
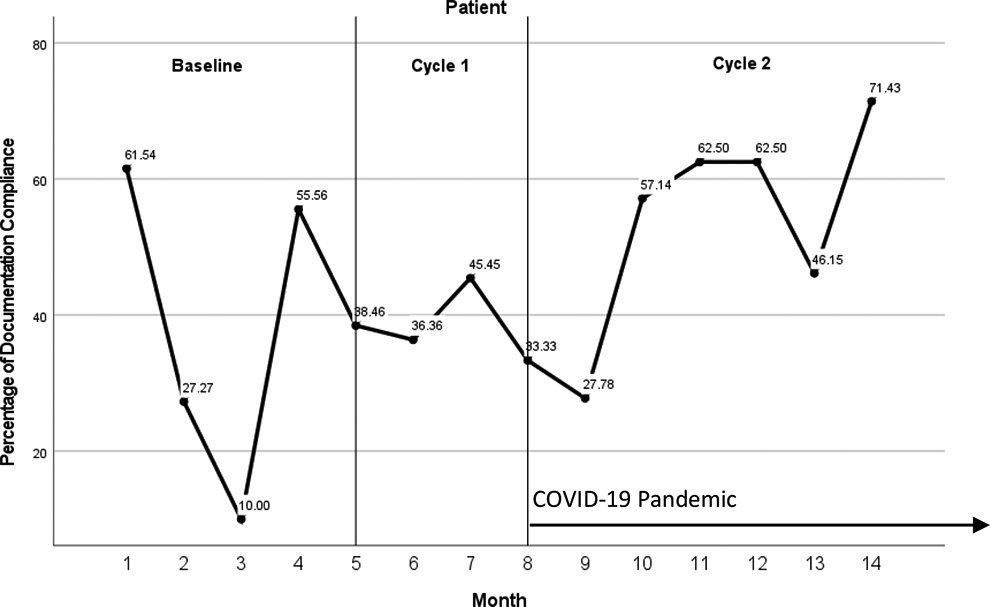
Figure 9 displays the results for assessment and documentation of a discussion with the patient of psychosocial/emotional distress. The peak rate occurred during the final month of data collection, Cycle 2, Month 14 with a 71% documentation compliance rate.
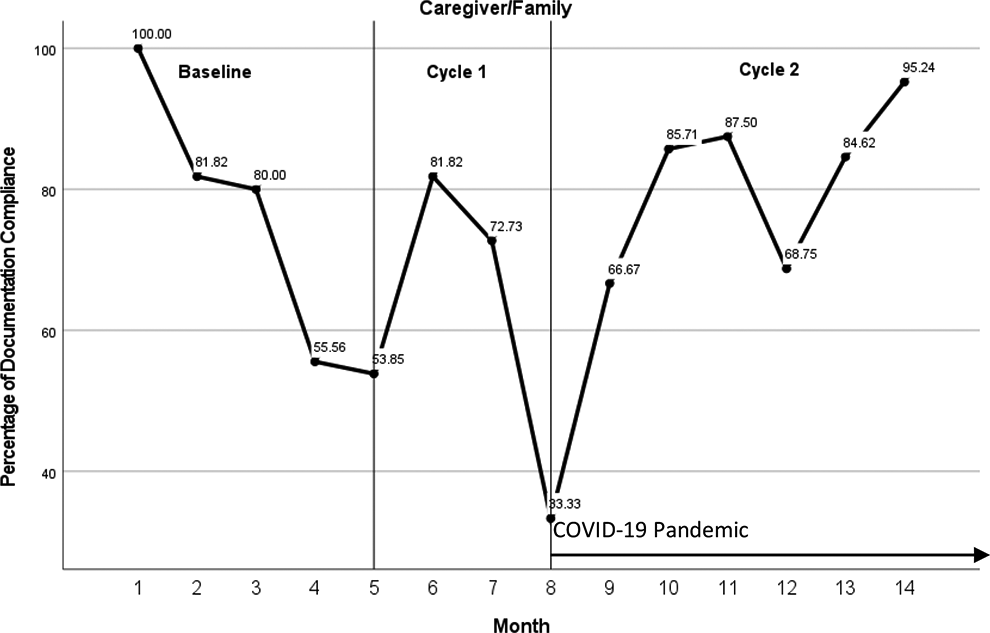
Figure 10 shows the results for assessment and documentation of a discussion with the caregiver/family regarding psychosocial/emotional distress. The peak rate occurred during Baseline, Month 1 with a documentation rate of 100%. There was only 1 month during all 3 PDSA cycles that showed less than 50%, Month 8, Cycle 2, just as the COVID-19 pandemic began.
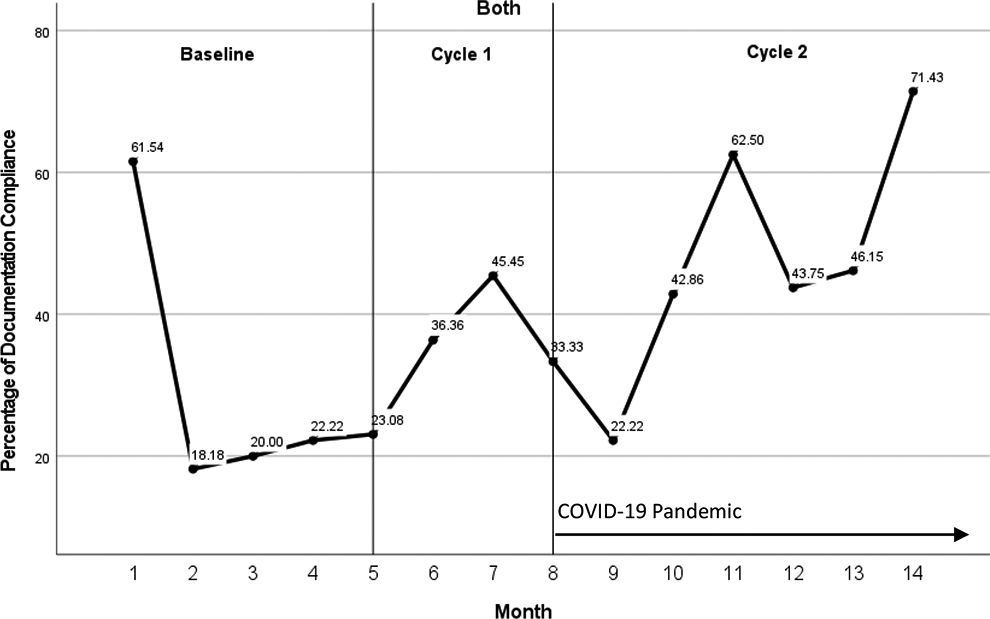
Figure 11 displays results for assessment and documentation of a discussion with both the patient and caregiver/family regarding psychosocial/emotional distress. The peak rate occurred during cycle 2, Month 14 at 71.43%.
PDSA cycle comparison
To evaluate the documentation compliance and impact of the PDSA cycle using statistical testing, chi square tests comparing the overall consult documentation for each PDSA cycle were conducted on 3 outcomes: Physical Symptom Screening, and Psychosocial/Emotional Discussion with the inclusion of a pediatric palliative care Social Work Note during admission. For this broader evaluation, if any element of physical symptom screening and discussion of psychosocial/emotional needs were addressed during the consult and documented, the record was coded as compliant. Results are shown in Table 3. There was statistically significant improvement in the inclusion of a pediatric palliative care social work note during admission from baseline (33%) to Cycle 2 (57%). Physical symptom screening declined slightly, but not significantly (p = .32) and psychosocial/emotional discussions also declined but not significantly (p = .03).
Consult Documentation According to PDSA Cycle.
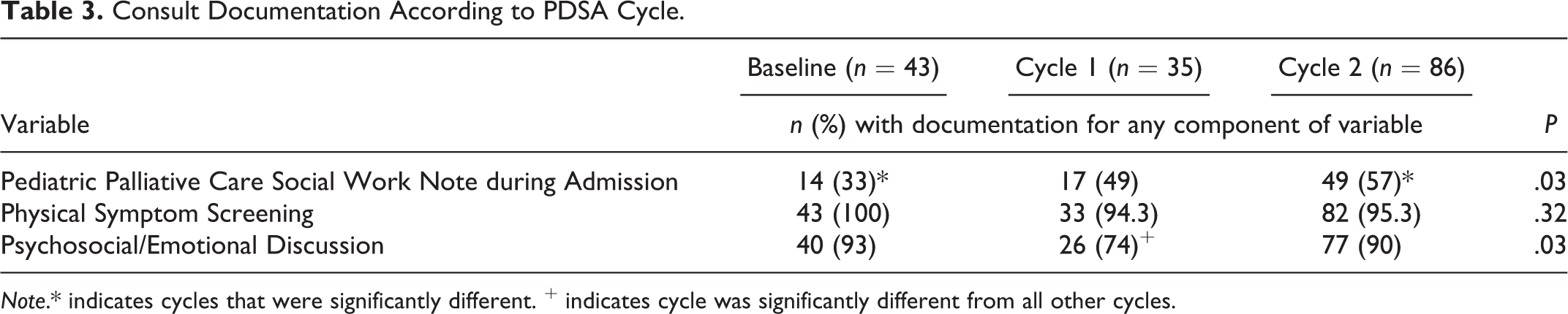
Note.* indicates cycles that were significantly different. + indicates cycle was significantly different from all other cycles.
There was non-significant improvement for conversations with the patient only from baseline (9%) to Cycle 2 (11%). Conversations with patients and family/caregivers also improved from baseline (33%) to Cycle 2 (43%), but not significantly. While the documentation of psychosocial/emotional discussions for patients <2 years old declined slightly from baseline (93%), there was significant improvement of documentation from Cycle 1 (55%) to Cycle 2 (90%). This documentation about psychosocial emotional discussions held with family/caregivers of children <2 years old also significantly improved from Cycle 1 (55%) to Cycle 2 (87%), although was still slightly lower than baseline (93%).
There was also statistically significant improvement in the inclusion of a pediatric palliative care Social Work note in the chart from baseline (33%) to Cycle 2 (57%).
Discussion
Interpretation
Evaluating programs to assess for quality using established indicators is necessary to improve palliative care services. The MWM indicators developed to benchmark palliative care programs are an important step toward improving quality of these programs nationwide. The results of this quality improvement project demonstrate the importance of assessment and documentation of physical symptoms other than pain, and having discussions around psychosocial and emotional needs with patients and their families/caregivers beginning with the initial palliative care consultation with an interdisciplinary pediatric palliative care team. These results also emphasize the difficulty in applying indicators designed to evaluate adult programs to those serving pediatric populations.
There are many important differences between the delivery of palliative care services for adult populations versus pediatric populations. 17 Indicators designed to evaluate programs geared toward adults may not directly translate to evaluate pediatric programs and need to be adapted. Children and their families who are facing potentially life-limiting illnesses have multifaceted and distinctive experiences that are not the same as adult. 16 The patient population at any given time plays a significant role in the ability to accurately assess these factors—for example, infants and young children or children who are intubated are often unable to communicate about physical or psychosocial/emotional symptoms or needs, so family members or caregivers are called upon as surrogates to report these needs to the healthcare team; while there are dedicated tools to assess symptoms in adult populations, unique assessment tools must be used at different stages of development to evaluate symptoms in pediatrics. 16 If parents or caregivers are not available to report, this further decreases the likelihood of accurate assessment and documentation of symptoms.
Additionally, it is clear that changes and reductions in on-site staffing due to a global health crisis during the project also impacted the consultations performed. In early 2020, in the middle of this quality improvement project (the beginning of PDSA Cycle 2, starting with month 8 of data collection), the novel coronavirus (COVID-19) arrived in the United States and was declared a global pandemic by the WHO in March of 2020. 26 During a pandemic, providing palliative care services remains critical, but can be challenging due to infection control mechanisms, limited resources, and other often unforeseen environmental pressures. 27 COVID-19 has had a dramatic impact on every aspect of healthcare, including the pediatric palliative care team involved in this project. Due to COVID-19 restrictions in the hospital, in April and May only the attending physician was present in the hospital to do face-to-face consultations with patients and families, and the PNP and CSW were working from home via telephone. The pediatric palliative care PNP returned to the hospital in May and the CSW returned in June. From June through August the pediatric palliative care team was also decreased to only 2 MDs. Conducting these initial palliative care consultations is time-consuming, which can prove even more difficult during a time when resources are stretched thin. Due to these changes in the composition and in-hospital presence of the pediatric palliative care team, fewer providers were available on a consistent basis to conduct initial consultations. Additionally, due to COVID-19 restrictions, morning rounds were held virtually instead of face-to-face, and fewer families were present in the hospital, especially at the beginning of the pandemic when visitor restrictions were enacted and only 1 parent was permitted at each pediatric patient’s bedside. Many parents faced additional challenges requiring them to care for siblings at home limiting their availability at the patient’s bedside.
Despite providing provider education and a reminder system about the importance of screening for the selected quality indicators for the first PDSA Cycle, then adjusting the provider template to improve ease of assessment and documentation for Cycle 2, there was a non-statistically significant decrease in overall physical symptom screening and discussions of psychosocial/emotional issues from Baseline to Cycle 2. There was, however, an increase in assessment and documentation of constipation and diarrhea in Cycle 2; this can likely be attributed to the inclusion of a question regarding the patient’s last bowel movement in the adjusted documentation template. Due to restrictions related to COVID-19, during Cycle 2 the pediatric palliative care social worker coordinated services and consulted with families by telephone. While typically many discussions involved in this type of coordination would have occurred face-to-face, working remotely necessitated consistent coordination and documentation via progress notes, which likely accounts for this improvement.
Limitations
Limitations for this study exist. Throughout the project consultations were being performed by multiple different providers, allowing for variability in the way each initial consult was conducted and documented, including the ways in which symptoms were addressed and discussions were held with each patient and family. Some patients may simply be too young to understand or express their needs, in which case the assessment may need to be performed by speaking with the patients’ parent or guardian. In other cases, the condition of the patient and family may prevent providers from performing a complete assessment during the consultation. If family members or caregivers are not present at the patient’s bedside during the consultation, it may also be difficult to obtain a full assessment during the initial consultation. Additionally, the data assess documentation of the screening only and do not reflect the degree to which discussions took place; documentation is a surrogate for adequate discussion, which may have been further impacted by decreased staffing, time-limitations, and other restrictions related to COVID-19. Most importantly, as pediatric quality measures do not exist, the MWM indicators chosen for this project are designed to assess adult programs, which in many ways are fundamentally different from pediatric programs and cannot be perfectly applied to evaluate pediatric palliative care programs effectively.
Conclusions
Screening for physical symptoms other than pain and having discussions with patients and their families around psychosocial and emotional needs during the initial palliative care consult are extremely important in gaining an accurate picture of the patient and family in order to provide effective, holistic, patient-centered care and to address “total pain.” When consults are conducted by a variety of providers, consistency during conversation and in documentation is key in assuring each patient receives high quality care. Good communication between patients, families, and providers is critical; when staffing is reduced, performing the necessary screenings becomes more difficult.
There must also be further research to determine methods for assessing compliance to palliative care guidelines.23,28 While the Measures that Matter clinical indicators used to assess palliative care programs for quality are valuable, they are geared toward an adult population. Pediatric populations present unique challenges in assessing symptoms of all types, and the needs of parents and families, which often differ from those in adult populations, must also be taken into consideration. Guidelines designed to evaluate adult programs cannot perfectly be applied to pediatric programs; pediatric-specific guidelines and quality measures must be developed to ensure standards are met consistently and programs operate effectively in delivering quality patient care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.