
Abstract
Background:
Although religion and spirituality are important to adults with cancer and their family caregivers, few studies have tested spiritual care interventions in the outpatient setting.
Aim:
To determine the feasibility, acceptability, and preliminary effects of chaplain-delivered, semi-structured spiritual care to adult outpatients with advanced cancer and their caregivers.
Design:
In this pre/post pilot intervention study, board-certified chaplains utilized the Spiritual Care Assessment and Intervention (SCAI) framework during 4 individual sessions. Surveys at baseline and at 1, 6, and 12 weeks post-intervention assessed spiritual well-being, quality of life, depression, anxiety, and religious coping.
Setting/Participants:
We enrolled U.S. adult outpatients with or without an eligible family caregiver. Eligible patients were at least 18 years old and at least 2 weeks post-diagnosis of incurable and advanced-stage lung or gastrointestinal (GI) cancer.
Results:
Of 82 eligible patients, 24 enrolled (29.3%); of 22 eligible caregivers, 18 enrolled (81.8%). Four planned chaplain visits were completed by 87.5% of patients and 77.8% of caregivers. All enrolled participants completed baseline surveys, and more than 75% completed follow-up surveys at 2 of 3 time points. More than 80% of patients and caregivers reported they would recommend the sessions to a friend or family member. Patients’ spiritual well-being improved significantly at all timepoints compared to baseline: 1-week post (p < .006), 6-weeks post (p < .001), and 12-weeks post (p < .004).
Conclusions:
Spiritual care through SCAI is feasible, acceptable, and shows promise in improving spiritual well-being and other important outcomes in advanced-stage cancer patients and family caregivers. Further investigation is warranted.
Introduction
Religion and spirituality are central to many patients and caregivers.1-4 Among adults with cancer, religion and spirituality are an important resource for coping with illness.5-11 While prior descriptive studies have addressed the religious and spiritual needs of inpatients,12,13 interventions addressing religious and spiritual needs of outpatients remain an area of opportunity for further study.14-16 Specifically, religious and spiritual needs of adult outpatients with advanced cancer have received little attention.17-19 This lack of knowledge is an obstacle to delivering holistic, patient-centered palliative care that provides relief from the symptoms and stress of advanced cancer.
The chaplain-delivered, semi-structured Spiritual Care Assessment and Intervention (SCAI) framework is an evidence-based intervention previously shown to be feasible and acceptable with family surrogates for critically ill adults in the ICU. 20 The objective of this study was to test the SCAI framework in adults with advanced cancer and their caregivers in outpatient settings. We conducted a single-arm pilot study with a pretest/posttest design at a National Cancer Institute-designated comprehensive cancer center located in the midwestern United States. Our primary aim was to assess intervention feasibility and acceptability for patients and their family caregivers, if available. Our secondary aim was to determine preliminary effects regarding psychospiritual and quality of life outcomes. Feasibility benchmarks included enrollment rates and attendance rates for study visits; acceptability benchmarks included survey completion rates and mean satisfaction scores.
Materials and Methods
Enrollment of participants occurred between January 2019 and March 2019. The study was approved on December 21, 2018, by the Scientific Review Committee of the National Cancer Institute–designated Indiana University Simon Comprehensive Cancer Center (IUSCC-0665) and Indiana University Institutional Review Board (IRB #1809545753). The study is registered on ClinicalTrials.gov with identifier NCT03823313. All participants completed written informed consent prior to enrollment.
Setting and Participants
Eligible participants were recruited from a single university-affiliated cancer center. Eligible patients were at least 18 years old and at least 2 weeks post-diagnosis of an incurable and advanced stage IV lung or gastrointestinal (GI) cancer, had a reliable phone for study contact, had adequate English fluency for completion of data collection, and did not exhibit significant psychiatric or cognitive impairment. Patients were eligible to participate with or without a family caregiver. Eligible caregivers were family members or close friends identified by patients. Caregivers were eligible to participate if they were at least 18 years of age, had been invited by an eligible patient, had a reliable phone for study contact, had adequate English fluency for completion of data collection, and were able to begin the intervention within 6 weeks of enrollment.
Patients were identified through electronic medical record review in advance of a scheduled appointment at the oncology clinic. Using a brief screening, the patient’s oncologist was asked to judge if the patient had a prognosis of 1 year or less. If there was uncertainty, the physician was asked, “Would you be surprised if this person died within 12 months?” which has been validated in prior research as a proxy for prognosis. 21 Eligible patients and caregivers were approached for informed consent. Most patients were approached in clinic, and most caregivers were approached by phone.
Data Collection and Instruments
A trained research assistant conducted baseline assessments in person at the patient’s clinic appointment or by phone within 21 days of enrollment. The baseline assessment included social and demographic characteristics. Eligible caregivers were enrolled within 30 days of patient enrollment. Participants were invited to complete assessments at baseline (T0; week 0), at the end of the SCAI intervention (T1—1-2 weeks post-intervention), at 2 follow-up timepoints (T2—6-8 weeks post-intervention; T3—12-14 weeks post-intervention). Participants received a $25 gift card for each completed assessment.
Participant assessments included a combination of measures of religious involvement, spiritual well-being, quality of life, religious coping, depression, and anxiety from previously validated surveys. Religious involvement was characterized at baseline using the 5-item Duke University Religion Index (DUREL; Table 1). 22 This measure was not included in other timepoints because it is believed to be static. Measures of spiritual well-being, quality of life, religious coping, depression, and anxiety were assessed across all time points as change from baseline. Spiritual well-being was assessed using the 12-item Functional Assessment of Chronic Illness Therapy-Spiritual Well-being Scale (FACIT-Sp-12; Supplemental Table 1). 23 The FACIT-Sp for non-illness participants was used with caregivers. 23 Quality of life was assessed using the McGill Quality of Life-Revised (MQoL-R) for patients and the Caregiver Quality of Life Index-Cancer (CQOLC) for caregivers (Supplemental Table 1).24,25 Mental health symptoms for patients and caregivers, including anxiety and depression, were assessed using the Generalized Anxiety Disorder scale (GAD-7) and the Patient Health Questionnaire (PHQ-8) (Supplemental Table 2).26,27 Religious coping was assessed using the Brief RCOPE (Supplemental Table 3) for both populations. 28
Descriptive Characteristics of Participants, Including Patients and Family Caregivers.
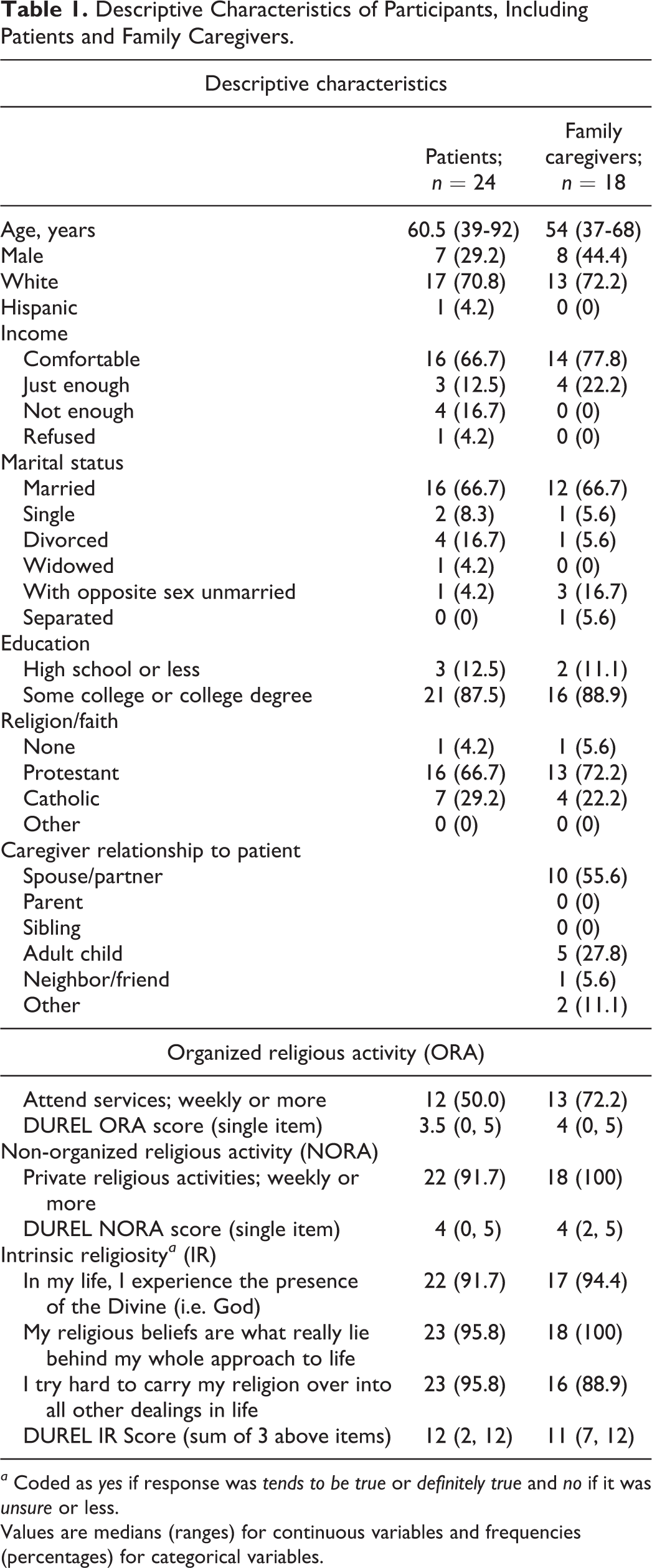
a Coded as yes if response was tends to be true or definitely true and no if it was unsure or less.
Values are medians (ranges) for continuous variables and frequencies (percentages) for categorical variables.
Interventions
Participation in the study included 4 chaplain visits with patients and caregivers intentionally assigned to different chaplains. The number of visits corresponded to the number of religious and spiritual dimensions addressed by the intervention framework—the SCAI—delivered by a chaplain who addressed an individual dimension at each visit. Visits were conducted in-person or by phone and were designed to last about 30 minutes. These sessions were scheduled in advance so as not to interfere with the patient’s clinical appointments.
SCAI is a semi-structured spiritual care assessment and intervention framework previously developed and tested with surrogates of intensive care unit (ICU) patients lacking decision-making capacity. 20 The SCAI framework includes proactive contact; a spiritual assessment addressing 4 dimensions of religious and spiritual experience; scripted questions designed to assess needs within each dimension; interventions tailored to the individual participant; and systematic documentation in the medical record. The 4 dimensions addressed by the framework are Meaning and Purpose, Relationships, Transcendence and Peace, and Self-Worth and Identity (Table 2). The intervention portion of the SCAI framework includes 26 interventions available to the chaplain. For example, the chaplain may acknowledge grief for a patient at the end of life or may offer to pray consistent with that patient’s tradition and informed by the SCAI spiritual assessment (Table 3). The chaplain determined the order to address each dimension based on assessment of each patient’s and caregiver’s needs. The semi-structured design of the framework allowed the chaplain the flexibility to devote time to the dimensions of greatest concern.
SCAI Cancer Use of Questions for Any Visit.a
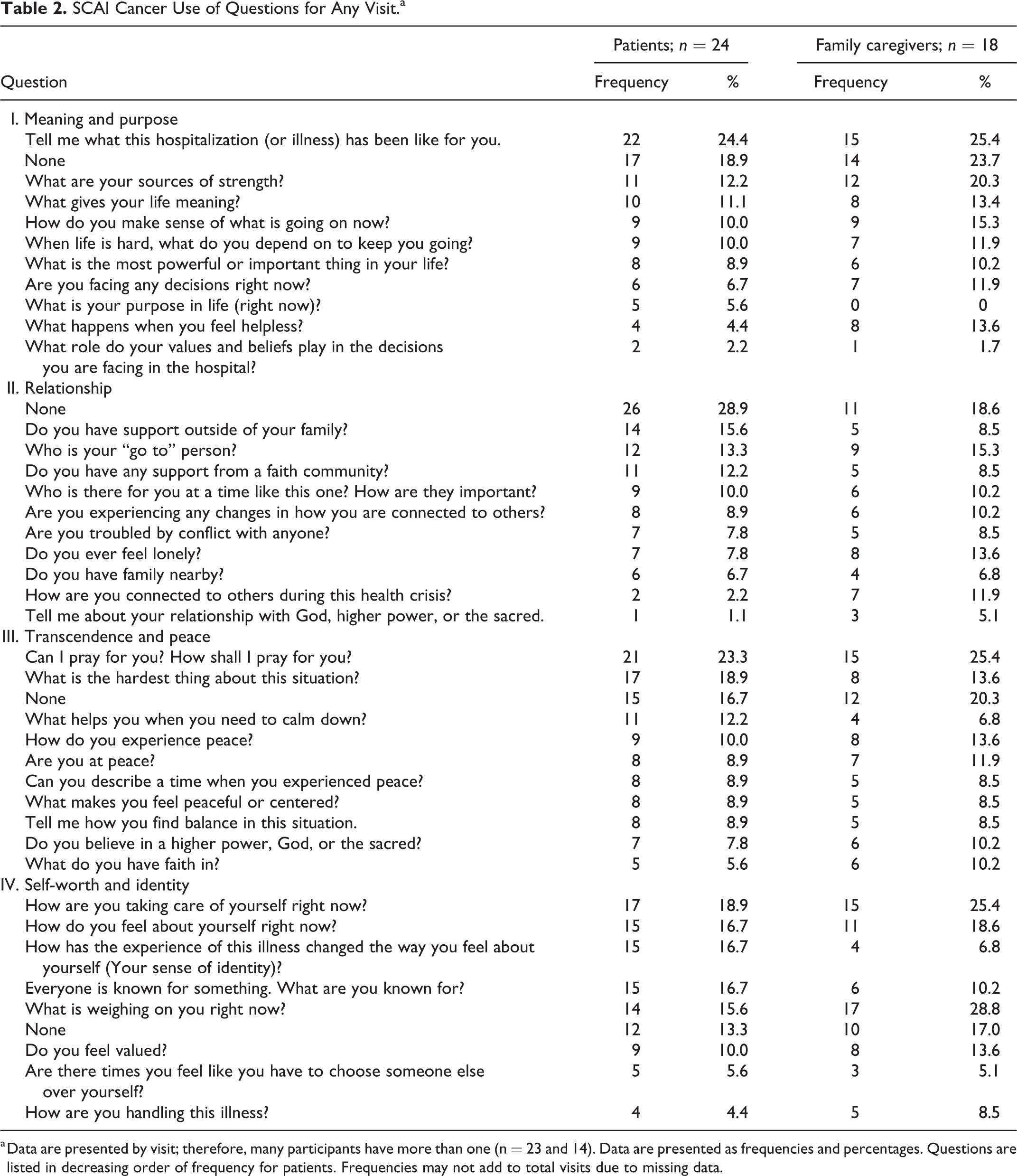
a Data are presented by visit; therefore, many participants have more than one (n = 23 and 14). Data are presented as frequencies and percentages. Questions are listed in decreasing order of frequency for patients. Frequencies may not add to total visits due to missing data.
SCAI Cancer Use of Interventions.a
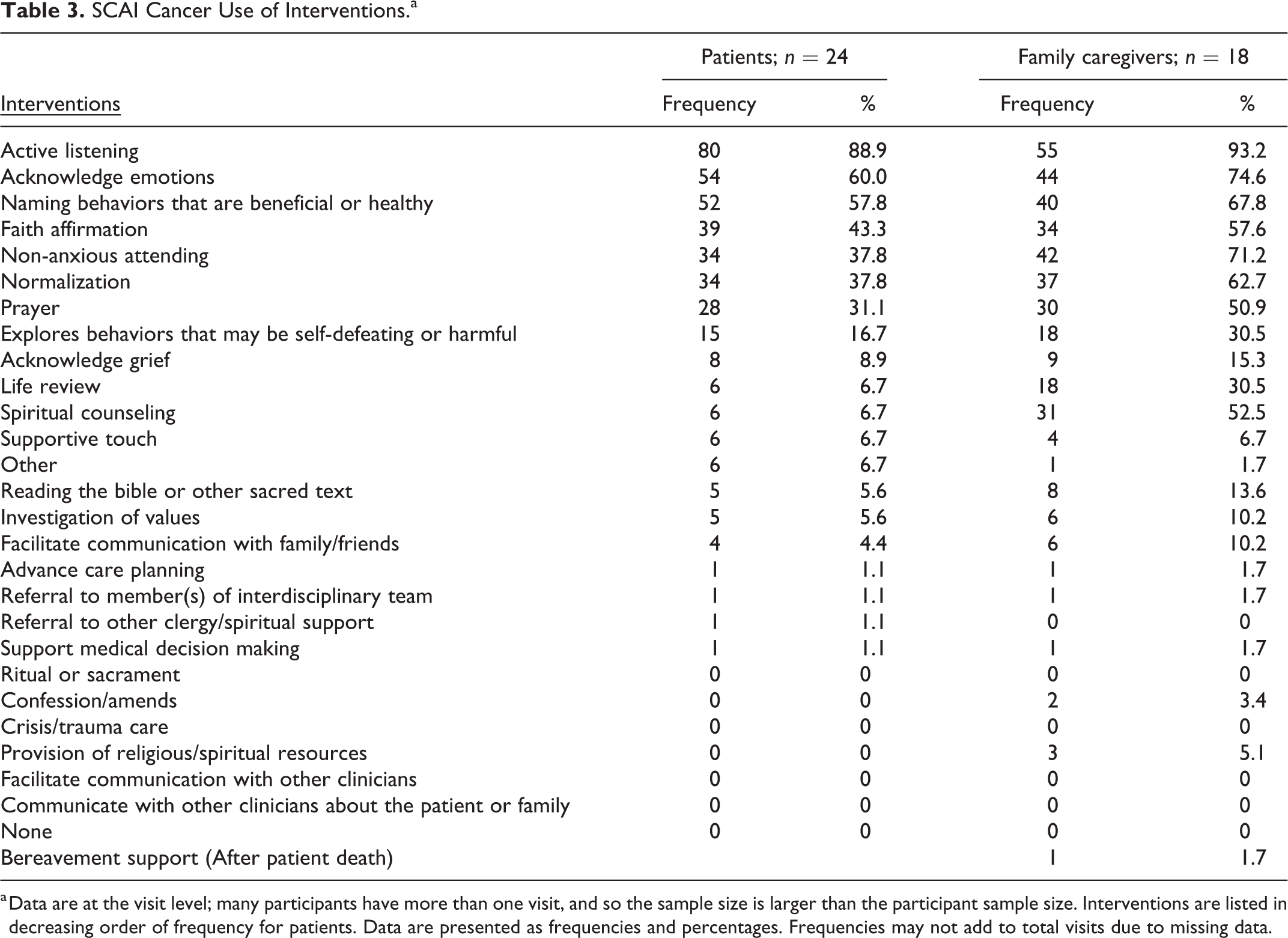
a Data are at the visit level; many participants have more than one visit, and so the sample size is larger than the participant sample size. Interventions are listed in decreasing order of frequency for patients. Data are presented as frequencies and percentages. Frequencies may not add to total visits due to missing data.
The SCAI framework was developed with chaplaincy input and rigorous review of current research on religion and spirituality, incorporating literature from international sources representing a variety of religious and cultural expressions. 20 The framework is intended to be delivered to participants by board certified chaplains. The 5 SCAI interventionists were graduate-level degree, nationally board-certified chaplains. In preparation for the study, chaplains participated in SCAI framework training by the study team, including a video training and discussion with investigators about the implementation of SCAI. Throughout the recruitment phase, chaplains met weekly to discuss and debrief their interventions. During this time, chaplains shared their experiences of implementing the framework and discussed challenges and benefits.
Qualitative Comments
Research staff utilized a standardized form to inquire about intervention satisfaction during phone interviews with participants at 12-weeks post-intervention. In addition to survey measures about outcomes of interest and quantitative satisfaction measures, research staff solicited qualitative comments from participants about what they liked most and least, things they learned, and anything they were doing differently post-intervention to cope. Responses were entered in Research Electronic Data Capture (REDCap). Comments were solicited to better understand nuances of the feasibility and acceptability with a new population (patients with advanced cancer) in a new setting (outpatient), as well as to tailor interventions for future studies. Two authors independently reviewed all participant comments and identified those that best illuminated aims of the study.
Data Analysis
Descriptive statistics for demographic and visit information were calculated for both patients and caregivers. Feasibility benchmarks included (1) enrollment rate greater than 40% of eligible patients and caregivers, and (2) attendance rate for study visits greater than 55%. Acceptability benchmarks included (1) baseline survey completion rate greater than 90%, (2) follow-up survey completion rate of greater than 75% and (3) mean satisfaction scores greater than or equal to 2.5 on a 1-4 scale. Preliminary hypothesis tests were performed to determine preliminary intervention efficacy for psychospiritual and quality of life outcomes. Analyses were performed to determine if responses changed significantly over time, from baseline to each of the 3 follow-up time points (1 week, 6 weeks, and 12 weeks post-intervention). Due to data skewness and non-linearity, non-parametric signed-rank tests were performed to determine if change over time was significantly different from zero (P < .05). All analytic assumptions were verified. Analyses were performed using SAS v9.4 (SAS Institute, Cary, NC). The data are housed at Indiana University in a Research Electronic Data Capture (REDCap) database. For inquiries about accessing a de-identified version of the database, contact the corresponding author.
Results
Patient and Caregiver Characteristics
Patients had a median age of 60.5 (range 39-92), and 25% were African American or Black; caregivers had a median age of 54 (range 37-68), and 27.8% were African American or Black (Table 1). Most participants were Protestant (patients 66.7%; caregivers 72.2%) or Catholic (patients 29.2%; caregivers 22.2%), with one participant in each group reporting no religious affiliation. We found that 50% of patients and 72.2% of caregivers reported attending religious services weekly or more; additionally, 95.8% of patients and 100% of caregivers strongly affirmed the item, “My religious beliefs are what really lie behind my whole approach to life” (DUREL; Table 1).
Feasibility
Over 11 weeks, 409 patients were screened for inclusion in the study and 82 were eligible (Figure 1). Of those eligible, 38 patients were approached and declined participation, with the most common reasons for refusal including “not interested,” “already has religious support,” or “doesn’t feel it would benefit me.” An additional 20 patients were approached and interested, but undecided. In total, 24 patients were enrolled (29.3%), and 18 identified eligible caregivers were enrolled. Most caregivers were spouses or partners (55.6%) with the next largest group being adult children (27.8%) (Table 1).
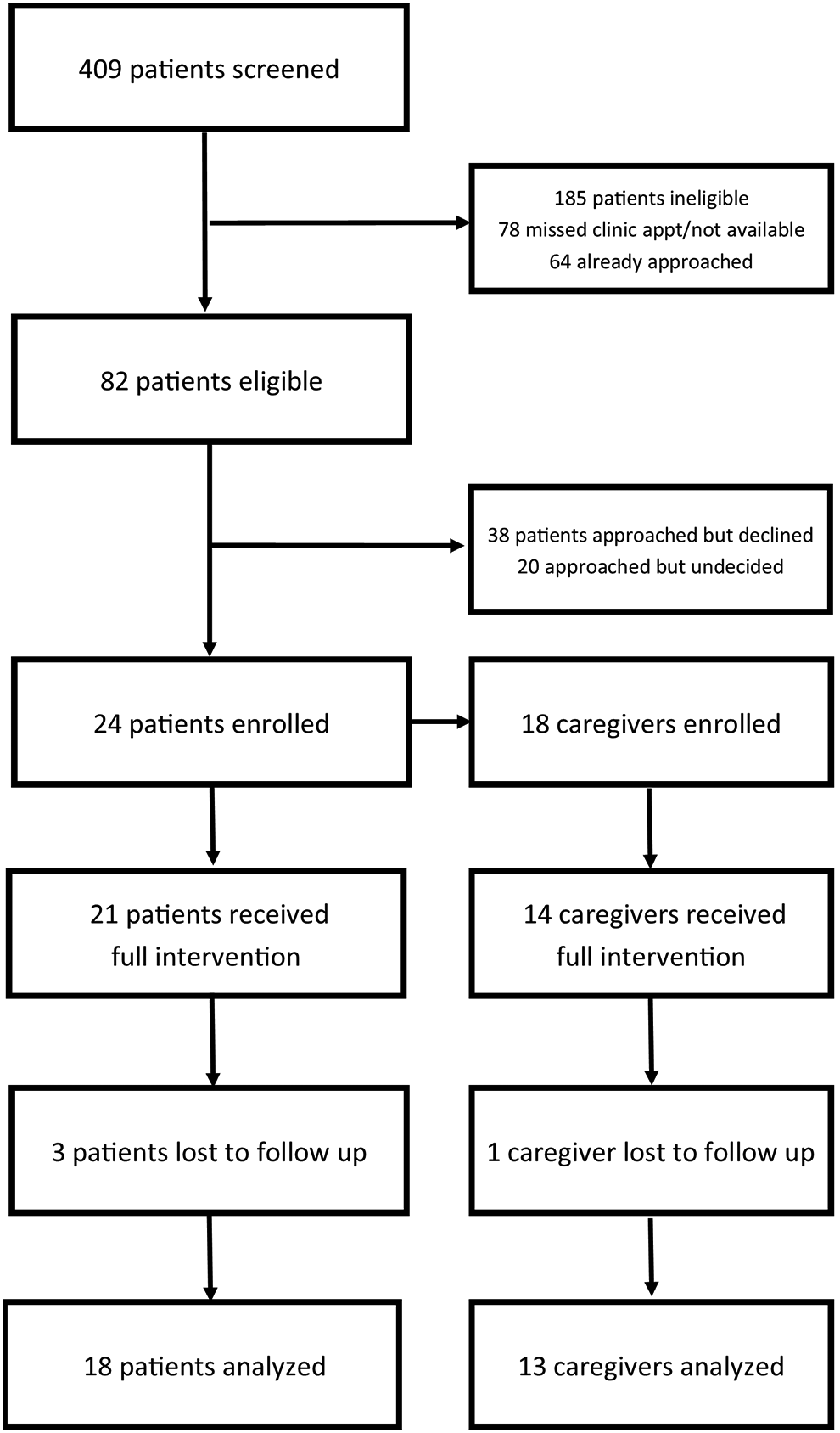
Study flow diagram.
All patients and a majority (16 of 18) of caregivers completed at least one spiritual care visit, and 21 of 24 patients and 14 of 18 caregivers completed all 4 planned visits (Table 4). Attendance rates for patients and caregivers were 87.5% and 83.3% respectively (Table 4). Visits occurred most frequently by phone (92.4% patients; 96.4% caregivers). Visits averaged 30.09 minutes for patients and 30.88 minutes for caregivers. Average visit duration remained relatively consistent across the 4 intervention visits (+/- 3 minutes). Of 26 possible interventions within the SCAI framework, 20 (76.9%) were used with patients, and 21 (80.8%) were used with caregivers (Table 3).
SCAI Cancer Chaplain Visits.a
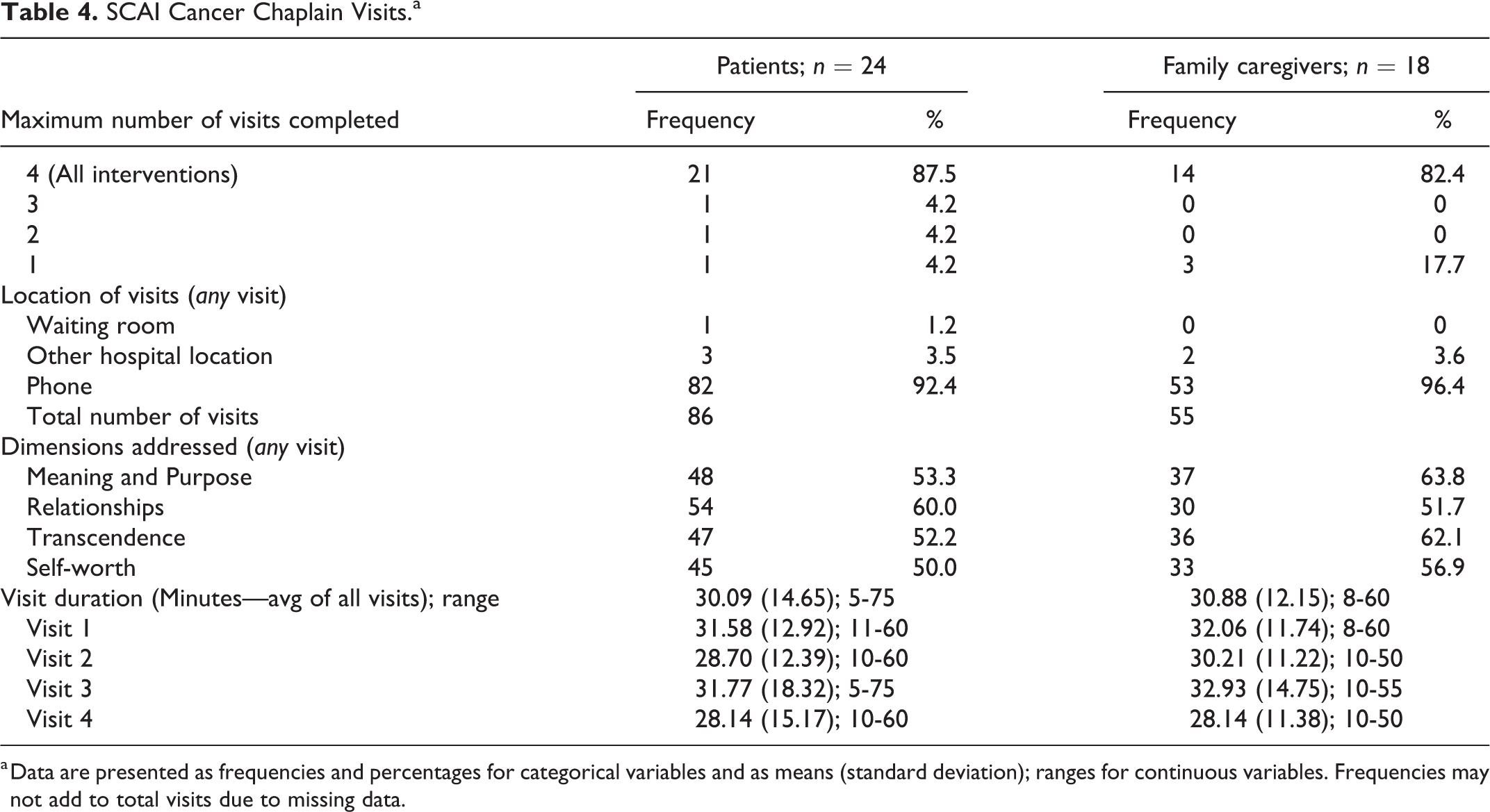
a Data are presented as frequencies and percentages for categorical variables and as means (standard deviation); ranges for continuous variables. Frequencies may not add to total visits due to missing data.
Acceptability
All enrolled participants completed baseline surveys (Supplemental Table 1). Follow-up survey completion rates were high overall with more than 75% of patients completing surveys at 2 of 3 time points (1-week 83.3%; 6-weeks 58.3%; 12-weeks 75%) and more than 75% of caregivers completing surveys at 2 of 3 time points (1-week 83.3%; 6-weeks 83.3%; 12-weeks 72.2%; Supplemental Table 1).
Patients and caregivers rated the project very highly; on a 1-4 scale, pro-rated mean satisfaction scores for patients and caregivers were 3.7. The pro-rated 4-point scale value was calculated by multiplying the current scores by 0.5714 (Tables 5 and 6). Approximately two-thirds of patients identified the sessions as moderately helpful or extremely helpful in “Learning how to live more positively through illness experiences,” “Improved experiences of peace as a result of receiving care from the chaplain,” and “Improved experiences of purpose as a result of receiving care from the chaplain” (Table 5). Of caregivers, approximately 80% reported the sessions were at least somewhat helpful in “Becoming more aware of coping with this illness,” and “Improved experiences of purpose as a result of receiving care from the chaplain” (Table 6).
SCAI Cancer Patient Satisfaction (frequency [%]).
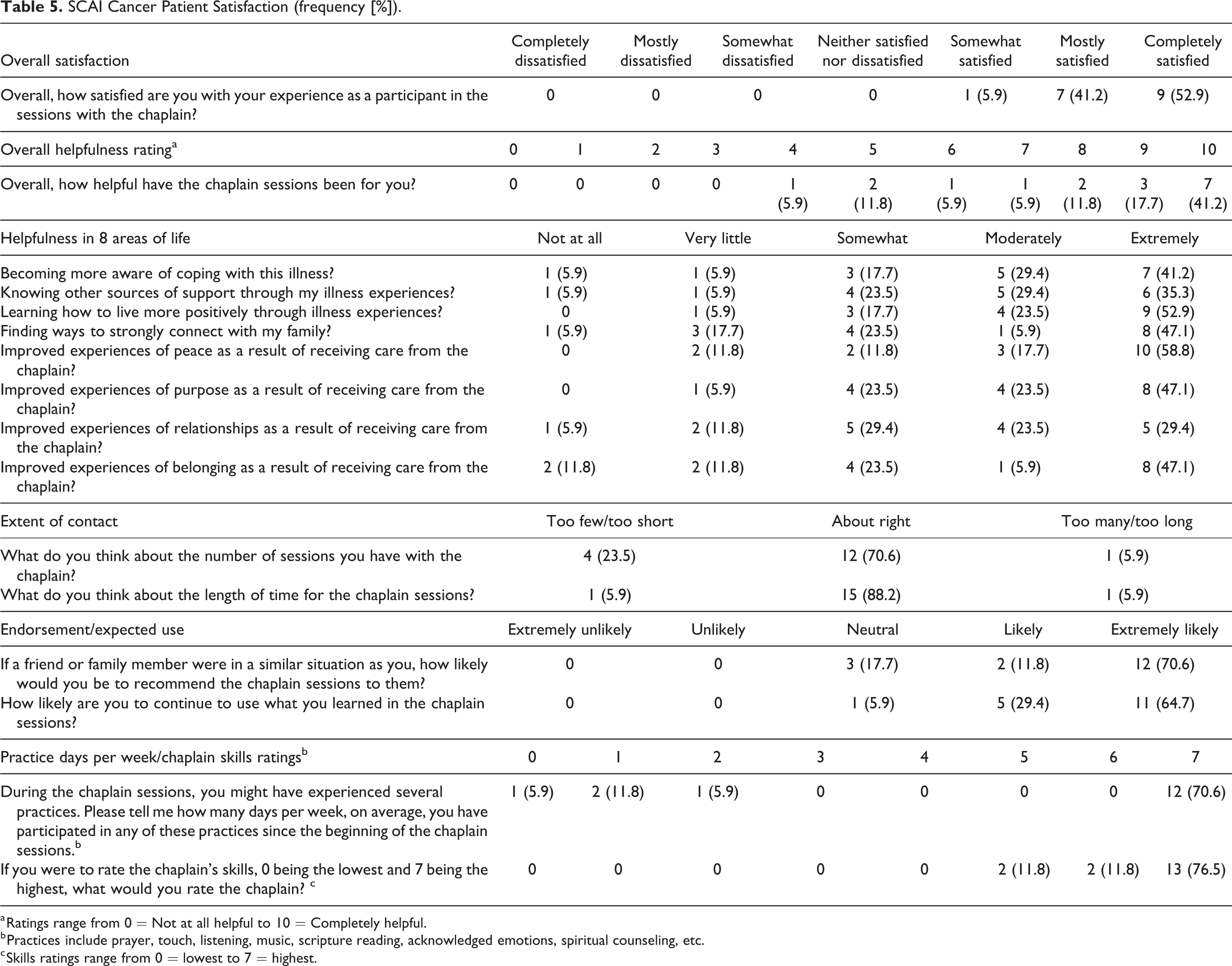
a Ratings range from 0 = Not at all helpful to 10 = Completely helpful.
b Practices include prayer, touch, listening, music, scripture reading, acknowledged emotions, spiritual counseling, etc.
c Skills ratings range from 0 = lowest to 7 = highest.
Data are presented as frequencies and percentages. Frequencies may not add to total visits due to missing data. Current overall satisfaction scores were pro-rated to a 4-point scale by multiplying current scores by 0.5714. The acceptability benchmark utilized a 4-point scale, whereas the current scale is 7-point, making a pro-rated calculation necessary for reporting benchmark and findings using the same scalar. The scalar was calculated by taking 4 (original scale) divided by 7 (current scale), arriving at 0.5714, which was then used to multiply the current scores to get the pro-rated mean value reported in the manuscript.
SCAI Cancer Family Caregiver Satisfaction (Frequency [%]).
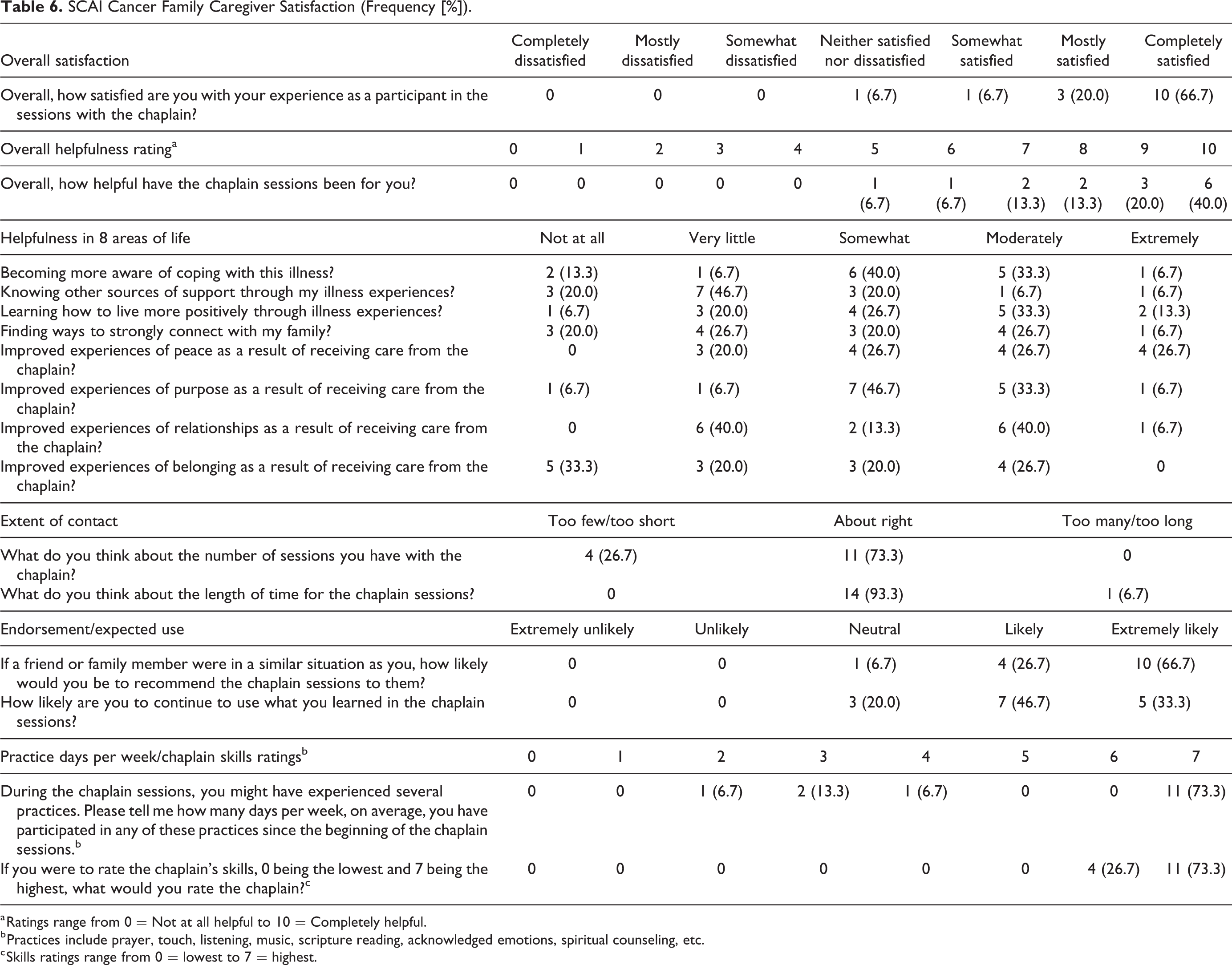
a Ratings range from 0 = Not at all helpful to 10 = Completely helpful.
b Practices include prayer, touch, listening, music, scripture reading, acknowledged emotions, spiritual counseling, etc.
c Skills ratings range from 0 = lowest to 7 = highest.
Data are presented as frequencies and percentages. Frequencies may not add to total visits due to missing data. Current overall satisfaction scores were pro-rated to a 4-point scale by multiplying current scores by 0.5714. The acceptability benchmark utilized a 4-point scale, whereas the current scale is 7-point, making a pro-rated calculation necessary for reporting benchmark and findings using the same scalar. The scalar was calculated by taking 4 (original scale) divided by 7 (current scale), arriving at 0.5714, which was then used to multiply the current scores to get the pro-rated mean value reported in the manuscript.
In review of qualitative comments, participants valued study interventions, such as acknowledging emotions, active listening, and specific rituals such as having the chaplain read a sacred text or pray with them. One such aspect was having a caring person to talk with and someone who listened to them. A patient stated, “…I usually try not to talk about my cancer because I don’t want to burden others or to be in the spotlight…it was really nice to talk to [the chaplain].” Another patient responded, “[the chaplain] made me feel comfortable sharing things I hadn’t talked about before…she’s a great listener, which was conducive to getting me to think more deeply about my illness.” Some people valued the more explicitly religious role of a chaplain such as providing prayer or Scripture reading: “…when [the chaplain] prayed for me, I felt like I mattered.” Comments from caregivers largely mirrored the comments from patients.
Patients and caregivers infrequently voiced preferences or concerns that varied from the designated structure of the intervention. Three such concerns were scheduling, desire for face-to-face interaction, and preference for additional time or sessions. One participant shared: “scheduling was sometimes hard.” Some participants acknowledged phone visits were more convenient than meeting in-person: “[it would have] been better to meet face to face, but I didn’t really want to go out in the cold weather…” Some participants wanted additional or longer sessions: “time went too fast, wanted more interaction,” and “I wish there had been more sessions.”
Preliminary Effects
Patients’ spiritual well-being demonstrated statistically significant improvement at all time points when compared to baseline: 1-week post-SCAI (P = .006); 6 weeks post-SCAI (P < .001); and 12-weeks post-SCAI (P = .004; Figure 2 and Supplemental Table 1). Patients’ and caregivers’ quality of life demonstrated statistically significant improvement at 2 time points when compared to baseline: patients at 1-week (P = .033) and 6 weeks (P = .011), and caregivers’ at 6 weeks (P = .034) and 12-weeks (P = .033). Other measures showed improvements at 1 time point, though not consistently (Figure 2; Supplemental Tables 2 and 3).
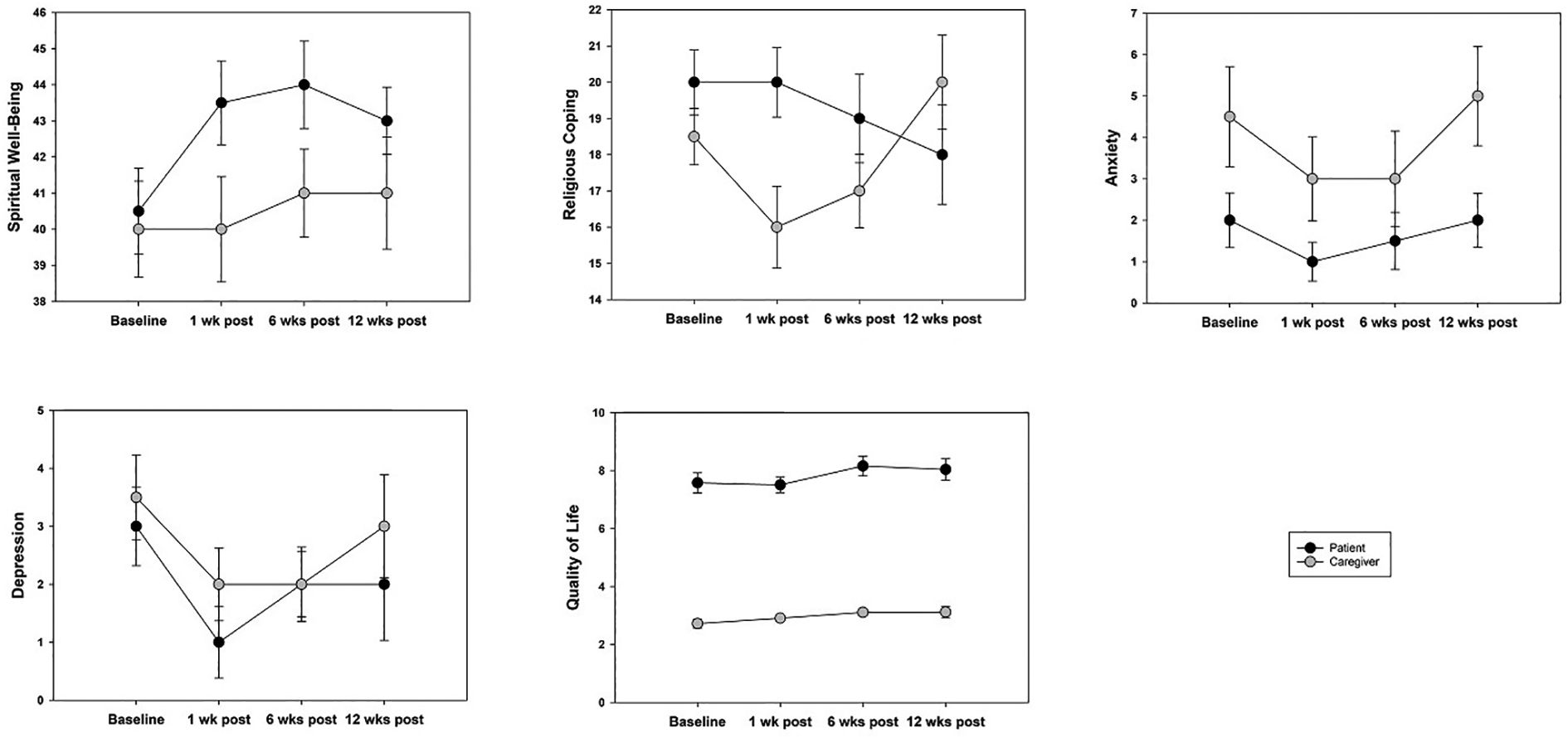
Changes in spiritual well-being, religious coping, anxiety, depression, and quality of life among patients and caregivers from baseline.
Discussion
Findings of this study of outpatient adults with advanced cancer support the feasibility and acceptability of utilizing the SCAI Framework with patients as well as preliminary evidence for use with caregivers. Whereas the previous study utilized the SCAI Framework with ICU surrogate decision-makers, this is the first study extending the SCAI Framework to patients. 20 Feasibility of completing outpatient study visits was high, with 21 of 24 (87.5%) patients completing all 4 study visits. For caregivers, this was slightly lower (82.4%). This far exceeds the hypothesized attendance rate of 55%. Though the study enrollment rate was lower than expected, enrollment was similar to prior studies. 29
Chaplains demonstrated sustained participant engagement across 4 sessions using the 4 dimensions in the SCAI Framework. All enrolled patients and caregivers completed the baseline survey with strong follow-up survey completion rates at most time points. Moreover, high patient satisfaction scores support the acceptability of the SCAI Framework, with 94.1% endorsing being mostly or completely satisfied with their overall experience with the study chaplain (Table 5). Significant changes in patients’ spiritual well-being, as well as significant changes in patients’ and caregivers’ quality of life demonstrate the impact of the framework with outpatient adults with advanced cancer (Supplemental Table 1). Small improvements also were seen in anxiety, depression, and religious coping at single time points (Supplemental Tables 2 and 3). These results suggest strong feasibility and acceptability with additional possibilities for improving enrollment in a larger study.
Importantly, most visits occurred by phone. This is in contrast to the delivery location of many spiritual care visits in the inpatient setting.30,31 However, spiritual care by phone is becoming increasingly acceptable in chaplaincy practice—especially given recent experiences with the COVID-19 pandemic.17,20,32,33 Spiritual care delivered by phone has notable benefits similar to virtual visits for clinical care: the care recipient is able to engage with a chaplain in a meaningful way without having to travel long distances, arrange childcare, or take extended time off from work, thus removing some barriers associated with healthcare access. Secondary benefits to tele-chaplaincy include the conservation of time and resources on the part of both participants and chaplains. These include clinical resources, particularly space, which tends to be at a premium in many ambulatory settings. A phone visit is unobtrusive to the workflow of the clinic. Another benefit of tele-chaplaincy is the recipient is in a familiar space and may feel more at ease sharing her or his concerns with the chaplain; this may be particularly meaningful for racially and ethnically diverse populations who may have negative past experiences in healthcare settings.
A limitation of this study is loss to follow up, which may have minimized detection of changes in outcomes over time. More robust data at multiple time points would provide additional information about the extent to which benefits of the chaplaincy intervention are enduring. A lower number of caregivers enrolled; this may be attributed to the requirement for a patient to enroll in order for a caregiver to be eligible to participate. Future studies could offer spiritual care to caregivers regardless of patient interest. Additionally, caregivers had lower distress scores at baseline on some measures, providing fewer opportunities for significant improvement in post-intervention scores (floor effect).
Participants were highly religious and primarily Christian. While representative of middle- and older-aged adults in the midwest, 34 generalizability to other U.S. regions with lower overall religiosity and greater religious diversity may be limited. Future studies should include different regions to capture greater variability in the degree of religiosity as well as recruit for a more religiously diverse sample.
A remarkable feature of this study is high retention of very ill advanced cancer patients over multiple visits. Participant comments suggested positive benefit from the intervention. Some participants stated they would have benefited from support earlier in their cancer diagnosis. Future studies could explore delivering SCAI earlier in the disease course.
Conclusion
Spiritual care through SCAI shows feasibility, high acceptability, and promise in improving spiritual well-being and other important outcomes in advanced-stage cancer patients as well as moderate success in supporting their caregivers. Given healthcare shifts from acute care to ambulatory care settings, spiritual care and chaplaincy have an opportunity to make a parallel shift to support patients and their caregivers in outpatient settings. Future work should test the efficacy of SCAI in a randomized controlled trial in comparison with standard care for outpatient adults with cancer diagnoses.
Supplemental Material
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211042860 - Spiritual Care Assessment and Intervention (SCAI) for Adult Outpatients With Advanced Cancer and Caregivers: A Pilot Trial to Assess Feasibility, Acceptability, and Preliminary Effects
Supplemental Material, sj-pdf-1-ajh-10.1177_10499091211042860 for Spiritual Care Assessment and Intervention (SCAI) for Adult Outpatients With Advanced Cancer and Caregivers: A Pilot Trial to Assess Feasibility, Acceptability, and Preliminary Effects by Shelley E. Varner Perez, Saneta Maiko, Emily S. Burke, James E. Slaven, Shelley A. Johns, Olivia J. Smith, Paul R. Helft, Kathryn Kozinski and Alexia M. Torke in American Journal of Hospice and Palliative Medicine®
Footnotes
Authors’ Note
All authors made substantial contributions to this manuscript and meet the definition of authorship.
Acknowledgments
We are grateful for the contributions of chaplains, physicians, nurses, medical assistants, and other staff who contributed to the successful completion of the study, especially Joy Bilger Goehring, MDiv, Nasser Hanna, MD, and Kelly A. L. Mathis, MDiv.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted with support from an internal grant from the Indiana University Health Values Fund, Indianapolis, Indiana; and Dr. Torke was supported by a Midcareer Investigator Award in Patient Oriented Research from the National Institute on Aging [K24 AG053794].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.