
Abstract
Purpose:
When patients with advanced cancer have minor children (age < 18), their health-related quality of life is closely linked to their concerns about the impact of progressive illness and death on their children. The Parenting Concerns Questionnaire (PCQ), a validated measure for parents with cancer, does not capture the full range of concerns in advanced cancer. The aim of this was study was to adapt and establish psychometrics for the PCQ for advanced disease (PCQ-AD).
Methods:
After generating an initial item-bank, we conducted concept elicitation interviews with clinicians (n = 8) and cognitive interviews with patients (n = 23) for face validity. New items addressed concerns about impact of parental death, making every moment count, communication, and financial impact of cancer on children. We administered 21 candidate items to 151 parents with advanced cancer. We conducted confirmatory factor analysis (CFA), calculated internal consistency, and assessed convergent and known-groups validity.
Results:
We removed 8 redundant items due to residual covariation between items. CFA of the 13-item PCQ-AD demonstrated satisfactory fit (CFI = 0.971, TLI = 0.966, RMSEA = 0.081) and high internal consistency (Cronbach’s alpha = 0.94, composite reliability = 0.95). The PCQ-AD demonstrated convergent validity and known-groups validity; patients with poor functional status reported higher scores than patients with better functional status (Cohen’s d = 0.56, p = 0.002).
Conclusion:
Adaptation of the PCQ yielded the addition of constructs important in advanced cancer. The PCQ-AD appears to be a reliable and valid measure of parenting concerns in advanced cancer, but future studies are needed to examine measure performance in diverse populations and responsiveness of the PCQ-AD to interventions.
Introduction
Adults with advanced (incurable or life-limiting) cancer who are parents of minor children report high levels of depression and anxiety and poor health-related quality of life (HRQOL).1,2 Research has shown that their psychological symptoms and HRQOL are closely linked to their concerns about the impact of their illness on their children and parenting abilities.1,3-7 Attention to their parental role is an important aspect of high quality clinical care for these individuals.
To mitigate parents’ distress and concerns in advanced cancer, it must first be measured reliably and accurately. Developed in 2012 by Muriel et al, the Parenting Concerns Questionnaire (PCQ) assesses parenting concerns in patients with any stage or type of cancer. 8 It has been validated in patients with mixed stage cancers as well as cancer survivors.8,9 The 15-item PCQ consists of 3 subscales that assesses parents’ concerns about the practical impact of their illness on children, concerns about the emotional impact of their illness on children, and concerns about their co-parent. The number of items in the co-parent subscale depend on the presence or absence of a partner and another living parent. The PCQ’s total and subscale scores represent an average of completed items rated on a 5-point scale (1 = no concerns to 5 = extremely concerned).
Although the PCQ demonstrated adequate internal consistency reliability (α = 0.86) in a study of 211 parents with advanced cancer, its original 3-factor structure was not supported. 10 In this study, parents’ concerns about the physical impact of illness and emotional impact of illness subscales were represented as a single factor. Both subscales were highly correlated with patients’ performance status (their ability to perform certain activities of daily living), suggesting that concerns about the physical and emotional impact of illness may be more challenging to differentiate in the context of advanced cancer. 10 Several studies of parents with advanced cancer also suggest that parents’ concerns about discussing end of life with children and the progressive loss of parental roles and responsibilities are important stressors for parents with advanced cancer.3-5 Typically, these domains are less pertinent for patients with early-stage cancers and therefore not addressed in-depth in the PCQ measure. Therefore, the purpose of this study was to adapt the PCQ for use in patients with advanced cancer (Parenting Concerns Questionnaire—Advanced Disease, PCQ-AD) and to evaluate the psychometric properties of the PCQ-AD, including convergent and known-groups validity.
Methods
Initial Item Generation and Refinement
We developed the PCQ-AD item bank from a comprehensive literature review, concept elicitation interviews, 11 and the full item bank developed by Muriel et al when first testing the PCQ (Anna Muriel, M.D., email communication, July 30, 2012). The purpose of the literature review was to identify parenting concerns that were not reflected in the original measure. The concept elicitation interviews consisted of audiotaped semi-structured interviews with 8 cancer care clinicians in mental health, oncology, nursing, social work, or palliative care. Interview questions addressed the representativeness of the initial item bank and significance of each item to the underlying construct of parenting concerns in advanced cancer. We used these interviews to confirm face validity of original item bank (n = 98, 90 were newly developed or reworded items) and to select candidate items (n = 59) for further testing.12,13
We used semi-structured interviews with 25 parents with advanced cancer to further refine the measure. These interviews included both concept elicitation (parenting concerns) and cognitive interview (evaluation of item importance, relevance, redundancy, acceptability, and comprehension) portions. 14 Mean interview length was 59 minutes (range, 25-123 minutes). Eligible parents were English-speaking adults who had a stage IV solid tumor with distant metastases and a minor child (age < 18 years) who lived in the home. 12 In these interviews, parents were first asked to describe their parenting concerns. They subsequently read and rephrased question items and talked through how they chose their item responses. 15 All parents were recruited from a large, public academic comprehensive cancer center. Purposive sampling (parent gender, age of children, single parent status, education level) was used to ensure a diversity of participant perspectives. We conducted 7 rounds of interviews (in groups of 3 to 5), iteratively refining the candidate items in response to feedback. We used Tourangeau’s model to analyze cognitive interviews. 14 Both the interviews and coding were conducted by 2 researchers experienced in semi-structured interviewing and qualitative analysis. 16
We selected 21 candidate items for psychometric testing. Candidate items reflected those from the original measure (n = 6) as well as newly developed questions. New items addressed communication with children, legacy-making, ability to parent, children’s coping, and financial impact. Questions related to partner support or co-parents were modified to allow for responses from all participants, regardless of marital or relationship status. All items included minor changes to the original PCQ’s question stem and formatting and were scored using a four-category Likert-type scale (1 = Not at all; 2 = Somewhat; 3 = Moderately; 4 = Very). It took less than 5 minutes to complete.
Psychometric Evaluation
From April 2018 to March 2020, we conducted a psychometric evaluation of the 21 candidate items. Eligible patients were parents or custodial guardians of a minor child and had a diagnosis of advanced cancer, defined as any of the following: stage IV solid tumor with distant metastases, stage III solid tumor with poor prognosis (e.g., unresectable stage III solid tumor), stage IV head and neck tumor, Grade III or Grade IV brain tumor, or relapsed and refractory hematological malignancy. We identified participants through review of ambulatory oncology clinic schedules of a large, public academic comprehensive cancer center or 1 of 6 community oncology practices. Participants’ disease status was confirmed with their oncology team prior to recruitment. We sequentially approached all eligible patients in person or by telephone. Of 179 eligible patients, 168 (94%) agreed to participate; of those, 151 completed all study measures and were included in the final analysis. The most common reasons for nonparticipation were loss to follow-up (n = 7) and participant death (n = 6). Two participants withdrew due to emotional concerns about the questions. All participants provided written, verbal, or electronic informed consent for each phase of the study which was approved by the University of North Carolina—Chapel Hill Institutional Review Board (No. 17-1820 and No. 18-2413).
Factor Analysis and Internal Consistency Reliability
We conducted a confirmatory factor analysis (CFA). Based on our prior studies using the PCQ and our adaptation to the co-parent subscale items, we conceptualized parenting concerns in advanced cancer as a unidimensional construct. While individual concerns vary between parents, these concerns are typically overlapping and highly interdependent. The latent factor was standardized (mean = 0, Standard Deviation, SD, = 1) to set the metric. The overall model-data fit was evaluated by testing the exact fit between the observed and model-predicted correlation matrices as well as comparing CFI, TLI, and RMSEA against the widely-accepted criteria (CFI/TLI > 0.95 and RMSEA < 0.06 combined indicates a good relative fit).17,18 All factor analysis models were estimated using a robust diagonally weighted least square estimator that is appropriate for analyzing ordered categorical data. 19 We also computed Cronbach’s alpha, item-rest correlations, and composite reliability statistics (based on standardized factor loadings).20,21
Convergent and Known-Groups Validity
Participants completed a sociodemographic and medical history form and the following validated measures:
Functional Assessment of Chronic Illness Therapy—Palliative Care (FACIT-Pal)
The FACIT-Pal assesses HRQOL in individuals with advanced cancer). 22 It has 46 items, each rated on a 5-point scale, and 5 subscales addressing Physical Well-Being, Social/Family Well-Being, Emotional Well-Being, Functional Well-Being, and palliative care. The total FACIT-Pal score ranges from 0 (low) to 184 (high).
Hospital Anxiety and Depression Scale (HADS)
The HADS is a common measure of depression and anxiety symptom severity in the medically ill. 23 The 14-item HADS has two 7-item subscales, each rated separately on a 4-point scale. Total scores for each subscale range from 0 to 21, with higher scores representing greater degrees of mood symptoms.
Peace, Equanimity, and Acceptance in the Cancer Experience (PEACE)
The PEACE questionnaire measures peaceful acceptance and struggle with illness among patients with advanced cancer and other serious medical illnesses. 24 The PEACE questionnaire has 12 items, each rated on a 4-point scale. The peaceful acceptance subscale ranges from 5 to 20, with higher scores indicating more peacefulness. The struggle with illness subscale ranges from 7 to 28, with higher scores indicating more struggle.
Parental Stress Scale (PSS)
The PSS is a general measure of the strains and rewards of the parental role irrespective of other life stress. 25 The PSS contains 18 items, each rated on a 5-point scale (1 = strongly disagree to 5 = strongly agree). All items are summed to derive a single parental stress score, ranging from 18 (low stress) to 90 (high stress).
Eastern Cooperative Oncology Group Performance Status Scale (ECOG)
The ECOG evaluates the severity of symptoms and amount of assistance an individual with cancer requires to complete “normal activities.” 26 This single item measure is graded on a 5-point scale ranging from 0 (no assistance) to 5 (death). We used a modified version of the ECOG for self-report.
Validity Analyses
We tested 2 hypotheses: (1) the PCQ-AD would demonstrate high convergence (r > 0.6) with other measures of psychosocial distress (depression and anxiety symptoms, parental stress) and divergence with measures of peaceful acceptance and HRQOL, and (2) PCQ-AD scores would significantly differ by patients’ functional status.
We conducted descriptive statistics for sociodemographic characteristics and structured measures. To ensure validity and generalizability of the results, missing data were also examined and treated using appropriate procedures. We quantified PCQ-AD correlations with PEACE, HADS, FACIT-PAL, and PSS scores for convergent validity. We assessed known-groups validity by comparing PCQ-AD scores between individuals with better (0 to 1) versus worse (2 to 4) ECOG scores.
Data preprocessing, descriptive statistics, missing data analysis, categorical CFA were conducted in R version 3.5. 27
Results
Participant Characteristics
The participants had a mean age of 43.7 years (SD = 7.6). More than 90% (n = 138) were currently receiving antineoplastic therapy. Table 1 summarizes participants’ sociodemographic characteristics; Table 2 summarizes their illness characteristics.
Participant Demographic Characteristics (N = 151).
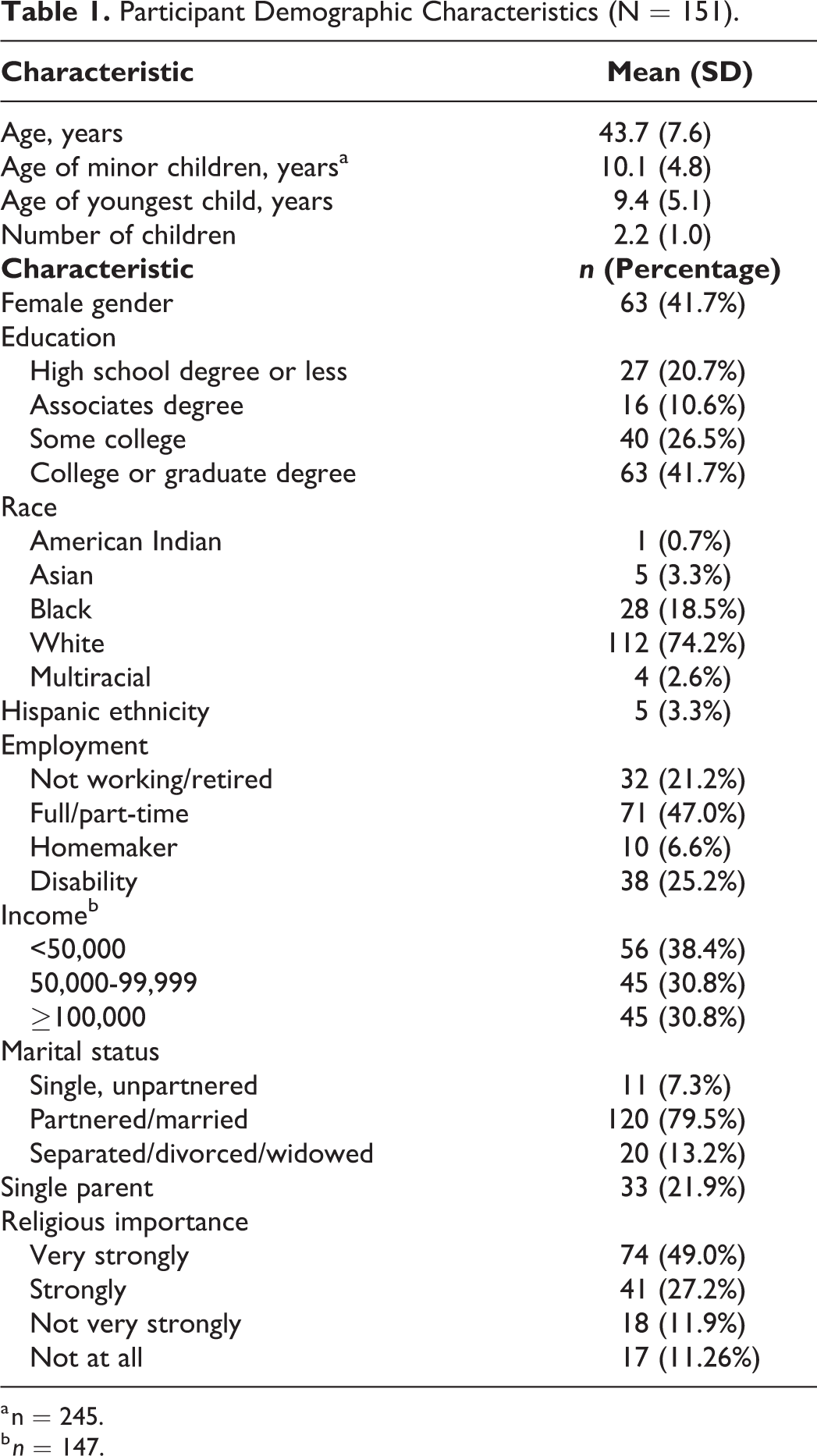
a n = 245.
b n = 147.
Participant Illness Characteristics (N = 151).
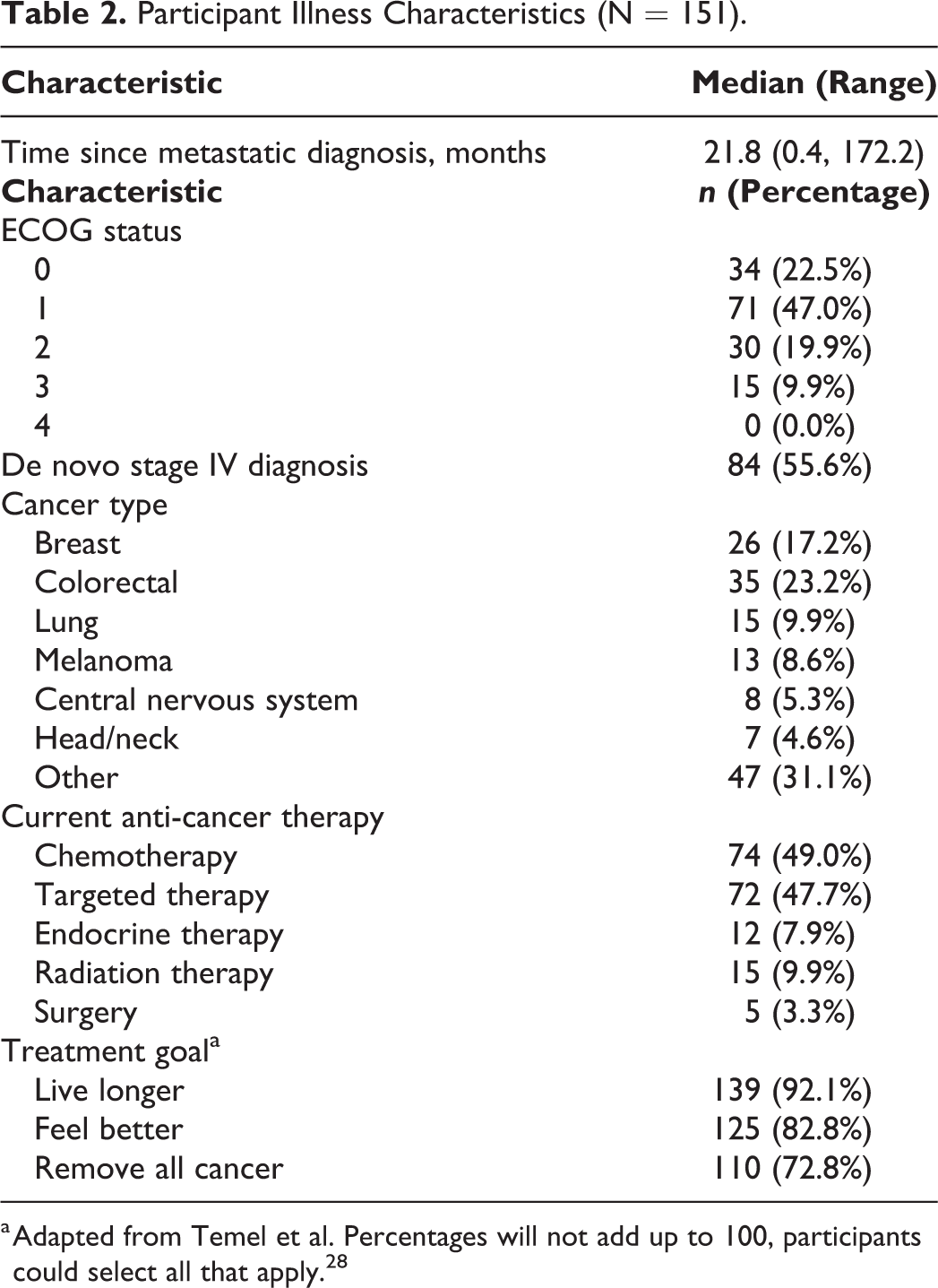
a Adapted from Temel et al. Percentages will not add up to 100, participants could select all that apply. 28
Factor Analysis and Internal Consistency Reliability
Table 3 lists the labels, stems, mean, range, and sources for retained items. Prior to CFA, we calculated the polychoric correlation matrix (see Supplemental Appendix) and found that some items had very high correlations (>0.8) which suggested overlapping or redundant item content. We then used item response theory model (similar to a categorical CFA model) to diagnose residual correlations. 29 The LD-X 2 indices revealed substantial residual covariation existed between items. We therefore removed 8 redundant items to obtain a well-fitting model. The revised 13-item model was then refit to the data, and the fit was satisfactory (CFI = 0.971, TLI = 0.966, RMSEA = 0.081). Among the 13 items, PCQAD_18 () and PCQAD_21 () had the weakest loadings relative to others (>0.7). In addition, no problematic residual covariation was found under this new model. Figure 1 presents a path diagram of the final model.
Reliability and Fit Statistics for the PCQ-AD (N = 151).
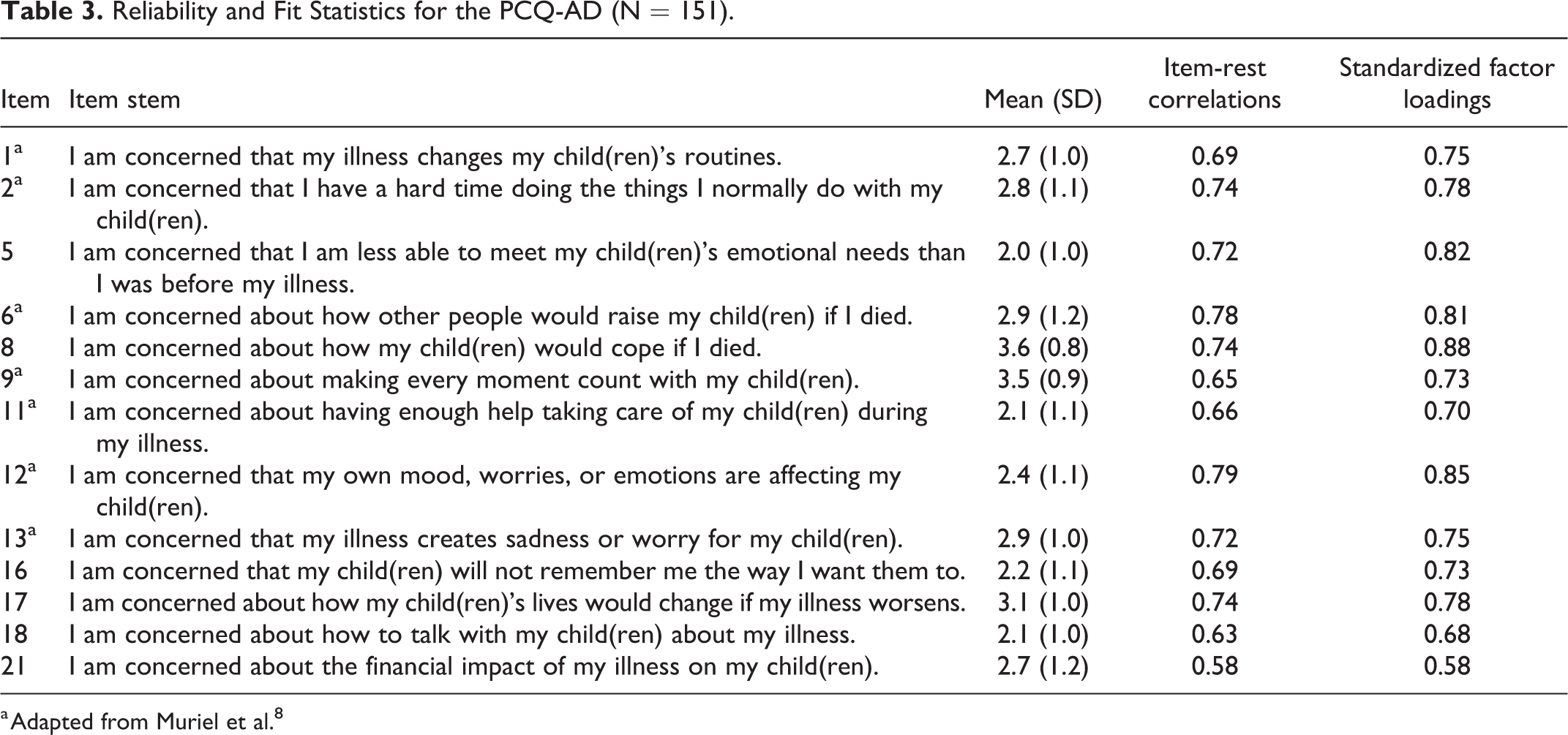
a Adapted from Muriel et al. 8
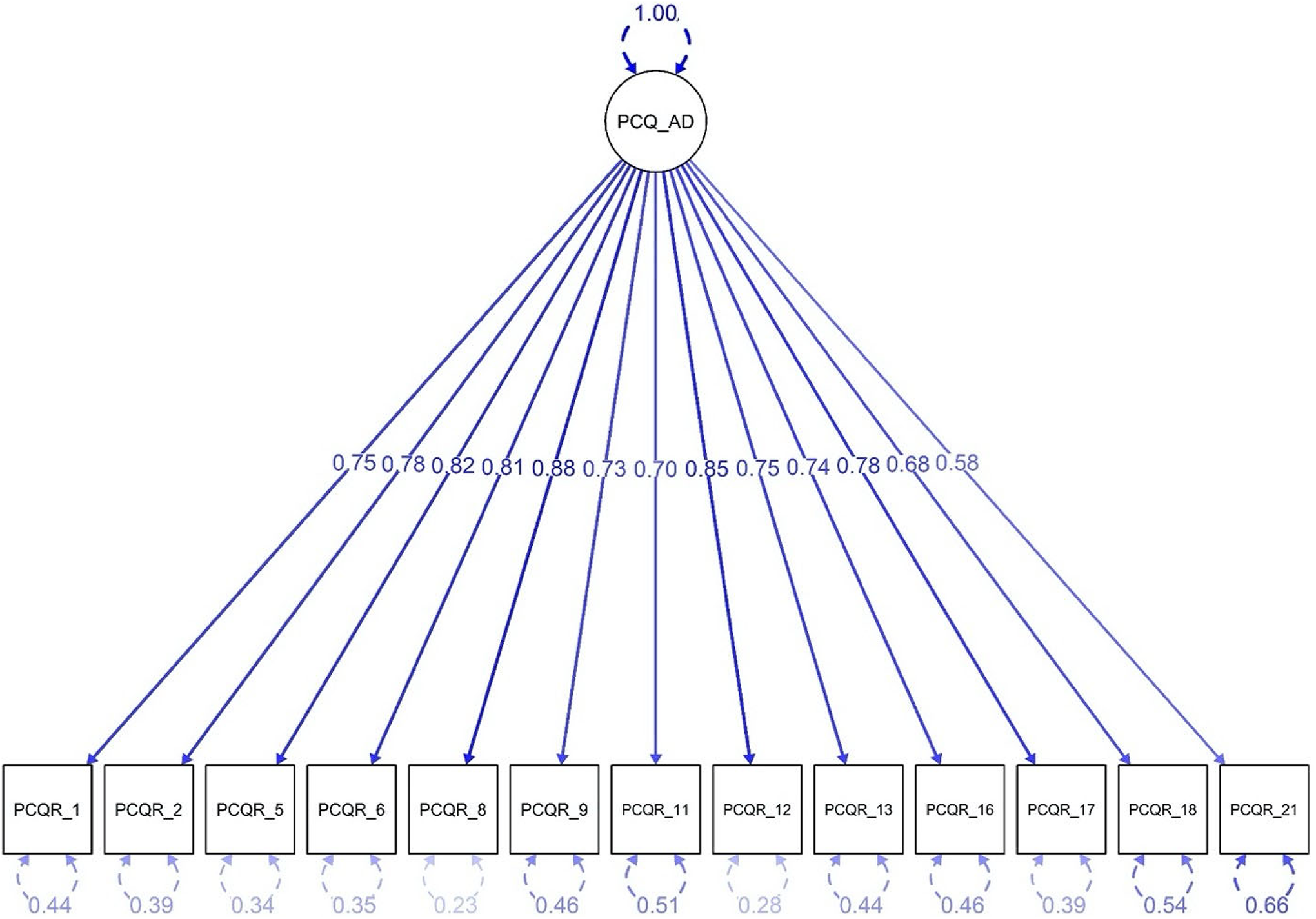
Path diagram for the 13-item single-factor structure.
The initial 21-item PCQ-AD measure and the shortened 13-item version were both found to be highly internally consistent. Item-rest correlations (Table 4) ranged between 0.60 and 0.79 (21 items) and between 0.58 and 0.79 (13 items). Cronbach’s alphas were 0.96 (full) and 0.94 (shortened); composite reliabilities were 0.97 (full) and 0.95 (shortened).
Validation Measures Summary Statistics and Pearson Correlations With the PCQ-AD.
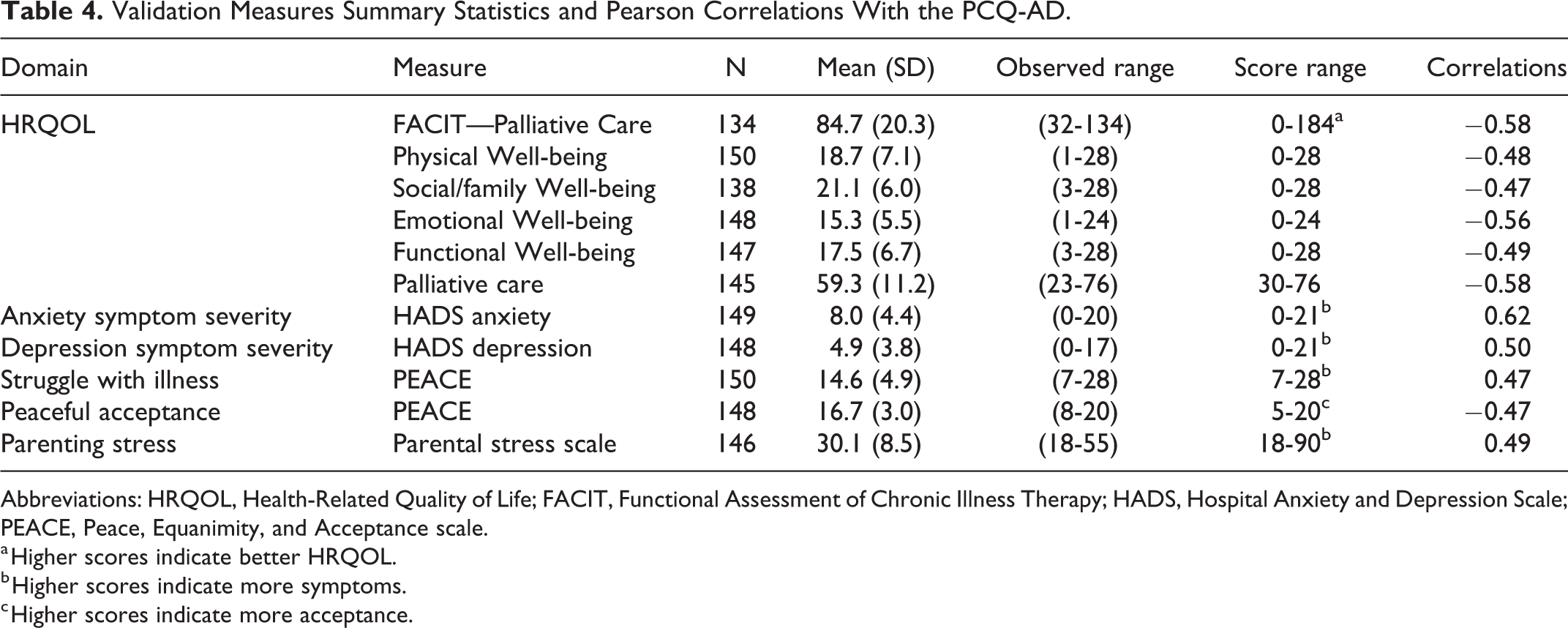
Abbreviations: HRQOL, Health-Related Quality of Life; FACIT, Functional Assessment of Chronic Illness Therapy; HADS, Hospital Anxiety and Depression Scale; PEACE, Peace, Equanimity, and Acceptance scale.
a Higher scores indicate better HRQOL.
b Higher scores indicate more symptoms.
c Higher scores indicate more acceptance.
Convergent and Known-Groups Validity
Table 4 shows the descriptive statistics for the FACIT-Pal, HADS, PEACE, and PSS as well as their correlations with the 13-item PCQ-AD. Mean FACIT-Pal Physical, Social/Family, and Functional Well-Being subscale scores were overall consistent with reference values for patients with metastatic cancer. In contrast, Emotional Well-Being scores were considerably lower. 30 Mean HADS Anxiety scores were 8.0, which equals the screening threshold for clinically significant anxiety symptoms. The PCQ-AD demonstrated convergent validity in expected directions with other measures of psychosocial distress (HADS Anxiety, PSS, PEACE Struggle with Illness, p < 0.001) or well-being (FACIT-Pal, PEACE Acceptance of Illness, p < 0.001). As hypothesized, there were significant differences between individuals with better (ECOG score 0 to 1) and worse (ECOG scores 2 to 4) functional status (Cohen’s d = 0.56, t = 3.22, p = 0.002). Additionally, of the demographic and illness characteristics, we found only gender difference; women reported significantly lower concerns than men (Cohen’s d = −0.388, t = −2.37, p = 0.019).
Discussion
We found that the PCQ-AD was a valid and reliable scale to measure parenting concerns in our sample with advanced cancer. New items address concerns about how children would cope with parental death, making moments count, communication, and financial impact of illness on children. Despite the emotional intensity of some of the PCQ-AD’s questions, participants did not demonstrate elevated distress as compared to other studies with this population.1,31 Nevertheless, parents’ assessments of their psychosocial functioning revealed clinically significant anxiety symptoms and poor HRQOL. These results highlight the need for measures that can more precisely evaluate the sources of their psychological distress.
The parenting concerns of patients with advanced cancer are closely linked to their worries about premature death. In this study, 3 quarters of the sample reported they were “very” concerned about how their children would cope if they died. Consistent with existing literature, parents’ concern increased as their functional abilities declined. 1 Qualitative studies provide compelling evidence that parents experience extraordinary psychological suffering related to the potential impact of their death on their children.3,5,32 Participants also reported high levels of concern about “making every moment count” with their children. Across cultures and countries, parents value preparing their children for life as adults and transmitting their cultural values. 33 This process of sharing values, traditions, and beliefs typically occurs over the course of several decades. 34 When serious illness disrupts this timeline, parents can feel an urgency to “create memories,” distill life lessons, and “cram a lifetime’s worth of parenting into a few short years.”3,32 Children similarly describe the pressure of spending compressed time together.35-37
Parents with cancer must decide whether, when, what and how to share information about their illness with their children. These discussions can become particularly challenging when cure is unlikely.38,39 Recognizing the contribution of communication concerns to parental distress, the creators of the PCQ included several items addressing communication in the initial item bank. Surprisingly, these items did not meet the factor loading threshold for inclusion in the original measure. This may reflect the broader range of disease severity in the original sample. 8 Both the adult and pediatric literature suggest that parents’ awareness of disease incurability greatly contributes to their fear of upsetting their children and the associated difficulties of having developmentally-appropriate conversations with them.5,40,41 Thus, including communication concerns are important to measuring the parenting experience of individuals with advanced cancer. More importantly, these concerns may be clinically actionable. 42
The inclusion of concerns about financial impact on children reflects the patient-centered focus of this measure. Both fathers and mothers consider financial support a key parenting responsibility and many parents identify being a financial provider as their most important parental role. 43 Modern US cancer care threatens this role in multiple ways. Adults experience lost wages and reduced ability to work due to cancer or its treatment. Out-of-pocket expenses directly and indirectly related to treatment lead to changes in household spending as well as substantial psychological distress and reduced HRQOL. 44 These cancer-related financial changes are particularly burdensome for younger adults as well as individuals with advanced disease, who can typically expect long-term, high intensity treatment and monitoring. 44 Assessing parents’ concerns about the financial impact of their disease on their children may therefore reveal an important and previously unmeasured contributor to their parental distress.
Limitations and Strengths
This study has limitations. The sample size did not allow for both exploratory factor analysis and CFA. Furthermore, the concurrent and predictive validity of the PCQ-AD, as well as its test-retest reliability, were not evaluated. Future studies incorporating criterion variables, repeated assessments, and larger samples will allow for a more comprehensive evaluation. Future studies can further evaluate the factor structure of the PCQ-AD and test its measurement invariance across demographic, sociocultural, and illness subgroups. Participants in this study were predominantly White and highly valued their religious faith, and these characteristics may not reflect the broader demographics of parents with cancer. Results may differ in more geographically or ethnically diverse groups. Addressing these limitations in future studies is essential.
This study also has notable strengths. The sample included a balance of mothers and fathers and patients from both academic and community oncology treatment settings. These attributes increase our confidence regarding the measure’s applicability to the broader population of parents with advanced cancer. Since all eligible participants were serially approached about the study, patients with a variety of tumor types were well-represented. In addition, we employed a rigorous process when generating candidate items prior to psychometric analysis. Collaboration with the PCQ’s original authors further allowed us to expand their prior work to a specific patient population with particularly high psychosocial needs and poor HRQOL.
Conclusions
In clinical settings, assessment of parenting concerns among patients with advanced cancer can be a challenging topic to broach, even for experienced clinicians.45,46 Having a brief and patient-centered measure that can accurately measure their concerns can facilitate delivery of targeted psychosocial care for these individuals. The PCQ-AD may be a useful clinical tool to aid the psychosocial evaluation of these individuals and we recommend further testing and evaluation of this measure.
Supplemental Material
Supplemental Material, sj-eps-1-ajh-10.1177_10499091211049801 - Adaptation and Psychometric Evaluation of the Parenting Concerns Questionnaire—Advanced Disease
Supplemental Material, sj-eps-1-ajh-10.1177_10499091211049801 for Adaptation and Psychometric Evaluation of the Parenting Concerns Questionnaire—Advanced Disease by Eliza M. Park, Mian Wang, Savannah M. Bowers, Anna C. Muriel, Paula K. Rauch, Teresa Edwards, Samantha M. Yi, Brittany Daniel, Laura C. Hanson and Mi-Kyung Song in American Journal of Hospice and Palliative Medicine®
Footnotes
Authors’ Note
The data that support the findings of this study are available from the corresponding author, EMP, upon reasonable request.
Acknowledgments
The authors gratefully acknowledge the individuals who participated in this study and who gave their time to share their experiences. Aspects of this study were presented at the Academy of Consultation-Liaison Psychiatry Annual Meeting on November 12-13, 2020 (held virtually).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (NIH) [grant number 5K07CA218167]; the Foundation of Hope; and the National Center for Advancing Translational Sciences, NIH [grant number 2KR891706]. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.