
Abstract
Keywords
Contributions of the Paper Statements
1. The findings could be used as a reference to design grief coping measures, guide grief-counselling processes for palliative care personnel, and develop localized teaching materials for life-and-death education so that patients and their families may receive more suitable end-of-life care and corresponding services.
2. Eastern and Western cultures have different attitudes toward death and grief. The coping methods adopted by individuals in Eastern cultures when facing death were summarized accordingly. These findings could serve as a reference to understand the coping mechanisms of individuals from Eastern cultures when dealing with anticipatory grief.
Introduction
When survival is no longer possible, patients, family members, and home-based palliative caregivers are forced to face the inevitability of death. 1 A majority of patients prefer spending their last days at home, which often exerts considerable physical and mental stress on their primary caregivers. 2 Current palliative home care services relieve the suffering of patients and their families through the comprehensive assessment and treatment of physical, and psychosocial, with the main goal of relieving symptoms. Since professional training for nursing personnel and caregivers does not include an emphasis on emotional care, such as grief counselling and grief adaptation and coping techniques, nursing personnel and caregivers often lack confidence in their ability to handle a patient’s (and family members’) grief; thus, these professionals are reluctant to attend to such needs. 3 However, when a primary caregiver’s emotional reactions are not properly guided and supported, deep grief likely will result, which could thereby negatively affect caregivers’ daily lives and mental health.4,5 Therefore, palliative care is provided through the teamwork between patients, families, and professionals in order to clarify care goals and provide symptom management, as well as psychosocial and spiritual support. 1
Eastern and Western cultures have different attitudes toward death and grief.6,7 Thus, exploring how individuals from both cultures perceive death and experience grief is of great significance within current multi-cultural environments. For this reason, the present study explored anticipatory grief experiences among primary caregivers of patients in home-based palliative care in order to better understand typical grief reactions, as well as caregiver needs when faced with an impending loss. The present findings could be used as a reference for designing grief coping measures, guide grief-counselling processes for palliative care personnel, and develop localized teaching materials for life-and-death education so that patients and their families receive more suitable end-of-life care and corresponding services.
Background
Grief and Anticipatory Grief
The word “grief,” originated from the Latin word “gravare,” which means the burden of sorrow. It is an experience that all individuals share, particularly when losing persons and/or objects, where there is a deep emotional attachment.8-10 Scholars pointed out that individuals experiencing grief usually go through a number of stages, namely “accepting the reality of loss,” “processing the pain of grief,” “adjusting to a world without the deceased” and “finding an enduring connection with the deceased in the midst of embarking on a new life.” In addition, the experience of grief is manifested through feelings, physical sensations, cognitions, and behaviors. 4
When individuals suffer a loss, their emotions, thoughts, values, and regular life rhythm tend to be affected. They are likely to get separated from their original pace of life, and their roles are likely to be shifted. In addition, the ability and time needed to adapt to a new family structure, social structure, and role identity, as well as handling the impact of the loss, tend to differ with each individual.8-10 Thus, balancing the relationship between grief and loss helps individuals cope with their grief experience. Each individual has his/her own way of grieving, and subsequent recovery processes also differ. Since loss is inevitable, having substantial support from external sources/networks could help alleviate the grief process while coping with the loss.
Anticipatory grief refers to the experience of grief that occurs prior to an impending loss. This is considered a protective coping technique that could mitigate grief reactions caused by actual loss through anticipatory mourning.11,12 Rando proposed the concept of anticipatory mourning and suggested that it is a broader concept when compared to anticipatory grief. 13 According to Rando, prior to an impending loss, individuals likely undergo a series of emotional experiences, including grief and mourning. During these processes, individuals not only react and adapt to the expected loss but also all losses and deaths in the past, present, and future. Therefore, anticipatory mourning covers grief and coping, and understanding anticipatory mourning is conducive to providing well-managed end-of-life care to patients, as well as assistance to their families, in order to regain balance in life. 13
Several studies have attempted to uncover anticipatory grief trajectories. The pioneer of near-death studies, Elisabeth Kübler-Ross, proposed five stages of grief: denial, anger, bargaining, depression, and acceptance.14,15 Since discussing demise is certainly not a heartfelt or appealing theme, individuals by and large will more often than not disregard or try not to talk about it. One might say that there is a denial of death in social orders, where demise is considered taboo. 15 To date, no study has explicitly tested whether the normal course of adjustment to a natural death progresses through stages of disbelief, yearning, anger, depression, and acceptance. 16 To examine the relative magnitudes and patterns of change over time post loss of 5 grief indicators for consistency with the stage theory of grief and the results find about 5 grief indicators achieved their respective maximum values in the sequence (disbelief, yearning, anger, depression, and acceptance) predicted by the stage theory of grief. 16 The identification of the patterns of typical grief symptom trajectories is of clinical interest because it enhances the understanding of how individuals cognitively and emotionally process the death of someone close. Such knowledge aids in the determination of whether a specific pattern of bereavement adjustment is normal or not.
Freud proposed the concept of “work of mourning” in 1917. According to Freud, the function of mourning is grief resolution, which allows individuals to gradually let go of their attachment to the lost person/object.17,18 However, if an intense ambivalence occurs during this process, this could interrupt the detachment process. Although Freud pointed out that such mechanisms are primarily concerned with the etiology of depression,19,20 such ambivalence also could be the foundation for mourning. In addition, the inability to let go of an attachment to the deceased is regarded as pathological grief.20,21
The present study defined anticipatory grief as a series of grief reactions experienced by family members to the impending separation from the patient, as they realize that death is unavoidable. Such reactions cover the physical, mental, spiritual, and social experiences of loss over the course of the entire illness, as well as the impending death.
Bereavement
The death of a loved one is a universal part of human life, which is often a significant life stressor, with effects across emotional, physical, behavioral, cognitive, social, spiritual, and financial domains. Throughout the bereavement literature, there is recognition that every grief experience is unique. 22 Bereavement is associated with poor physical outcomes among older adults, including weight loss, decreased nutritional intake, immune system impairment, increased illness susceptibility, and mortality risk.23-25 A recent population-based survey found that about 7% of those who experience excess bereavement develop complicated grief. Thus, palliative care services may be best served by investing efforts toward assessing and supporting family caregivers during the pre-bereavement period while developing referral pathways for bereavement care. 26
Domestic and International Studies
This section reviews domestic and foreign studies on anticipatory grief. The majority of theories related to grief prior to, and following, the death of a loved one has been proposed by Western scholars. There is currently no theoretical grief framework specifically designed for Eastern cultures. Domestic studies on grief experiences and adaptation still adopt Western theories; only a limited number of scholars have incorporated characteristics of Eastern cultures into their research designs.27-29
Each individual grief process is unique, all cultures have created ways of adapting to death. For example, the traditions of Anatolia give importance to sharing and supporting the family of the deceased, which overlaps the literature of bereavement process psychology. In Anatolia, when people die, the first thing they are required to do is read Qur’an loudly, which comforts the person and diminishes the fear of death. The other most important requirements are that a dying person can utter Kelime-i Shahada, which can help them go to heaven eventually. 30
Cultural and religious practices applied while the individual is on his/her deathbed, during, and after his/her demise have a positive and soothing impact on the loved ones of the expired. Such practices as memorial service customs plan to add to the change, a transformation of the expired as well as those in grief. Beliefs, practices, funeral rites differ between cultures, social groups, gatherings, yet all are connected with feelings communicated and largely rely upon society and its cultural-religious traditions.15-17
The Western theories of grief are mainly constructed based on individualism and existentialism and focus on an individual’s grief responses.4,14,15,31 Few studies have considered the characteristics of social networks and perceived relationships between the living and nature in non-Western countries. However, in Eastern countries and regions, individual grief responses likely differ, particularly in regions such as Taiwan, where ancestor worship constitutes a significant portion of folk customs. Some Taiwanese scholars believe that culture might affect how individuals are attached to the deceased, which thereby influences grief responses. 32 Hence, Taiwanese researchers have proposed a grief recovery theory suitable for Eastern societies that is influenced by the rationalism of Confucianism and monotheism, which incorporates individual relationships with heavens, gods, ghosts, ancestors, and society.32,33 Coping involves funeral ceremonies in order to settle the deceased’s soul.32,33 Hsu, Yee, and Lee explored grief resolution in a Taiwanese sample and discovered a series of grief responses that focused on reconnection with the deceased, including maintaining the status quo, restoring images of the deceased within family affairs, and communicating with the dead. Religious practices, spiritual mediums, and ancestor worship were found to be common channels for such reconnection.34,35 Thus, individual anticipatory grief appears to be influenced by cultural differences. Furthermore, a “sense of loss” and “recovery from grief” tends to be a repeated occurrence during the coping and adaptation process.
Methods
In our research, we use phenomenological approaches and methods to gather answers.36,37 The present study adopted a qualitative exploratory research design and used open-ended in-depth interviews to explore anticipatory grief experiences among 16 primary caregivers of patients receiving palliative home care. Participants were providing primary care for family members with cancer. Posters and snowball sampling were used to individually recruit participants. The interview dates, times, and locations were chosen for convenience of the interviewees. All interviewees were able to communicate in either Mandarin Chinese or Taiwanese Hokkien. Each interview was divided into two to three sessions, and each session lasted 60-90 minutes. The interview records were then collected and compiled. The sampling and analysis processes were repeated until no new themes appeared, and theoretical saturation was achieved.
We transcribed them and sent the records back to the participants for an audit of exactness and culmination. Whenever they had shown that these records caught what they needed to say about the experience, We investigated them utilizing a hermeneutic phenomenological approach. We didn’t attempt to break down a few implied unique collaborations that participants referred to in their records to assess them. All things considered, our attention was on reports of their experience and how they deciphered these. This study was approved by the Institutional Review Board for Human Participants (IRB # 10404-007) at our host university; the process respected the corresponding requirements of research ethics.
The interviews were conducted in a quiet and undisturbed location, typically a participant’s living room. The interviews were audio-recorded, and consent from the interviewees was obtained prior to each interview. The collected data were then coded. Use semi-structured interviews to collect data and an open-ended questionnaire as the interview outline. The items were as follows: (1) How (have) you (been) doing recently? (2) Who provides you with support during this period? (Is there anyone that you can turn to or give you support when you are unhappy and feeling low?) (3) Can you describe the feelings you have been experiencing since the diagnosis of your parent/spouse/in-law (the patient for whom the interviewee was caring)? (4) Can you describe the relationship between you and your parent/spouse/in-law before his/her diagnosis? (What do you think of him/her? What kind of a person is he/she?) (5) How close are the two of you? (6) When did you start to realize that you might lose your parent/spouse/in-law? How did you feel at the time? (7) How did you feel when his/her condition worsened? (8) Have you thought about how you would handle his/her affairs? (What would take place if he/she passed away?) (9) Do you have any plans for the future (in case he/she passes away)? (10) Is there anything else you want to share?
All interviews were recorded truthfully and completely, and the data were compiled within 36 hours following each interview. A “thematic analysis method” approach, proposed by Alholjailan,38,39 was utilized to analyze the interviews. The researchers conducted the interviews, as well as verbatim transcription, compilation, and analysis of the data. First, we transcribed the audio recordings of all interviews and preliminarily organized the text transcripts. Then, we carefully read the text transcripts and extracted statements related to primary caregiving as minimal units of coding. The common code characteristics were then clustered, and similar categories were grouped into themes. We read the records more than once, expressed our general feelings about each record, recognized themes, assessed the relationship of explicit expressions to the different subjects, and analyzed the relationship of themes with one another. We searched for logical inconsistencies in the strings.
While reading all interview materials, the researchers maintained an objective attitude, let the concept (code) emerge from the data itself, and when the open coding produced several low-level concepts, “spindle coding” was used. A concept was gathered together and generated from the bottom up. In other words, when a lower level concept (code) was present, more details were gradually gathered to create a higher-level concept (code). Each text transcription was independently analyzed by two researchers, and a consensus discussion was conducted when there was disagreement.
Evaluation criteria proposed by Lincoln and Guba 40 were adopted to assess validity of our methods. Each interview recording was played at least three times to ensure accuracy of the verbatim transcription. Moreover, authenticity of the collected data was analyzed and assessed by peer experts. Three weeks after the main data analysis, we randomly selected paragraphs from text transcripts and conducted a second content analysis. This second categorization was compared with the original, revealing a consistency of 92%. Interrater reliability between the two researchers was 82%. All researchers received 92 hours of training related to palliative care along with other training on communication and consultation skills.
Results
Interviewee Demographics
Demographic Characteristics of the Interviewees (n = 16).
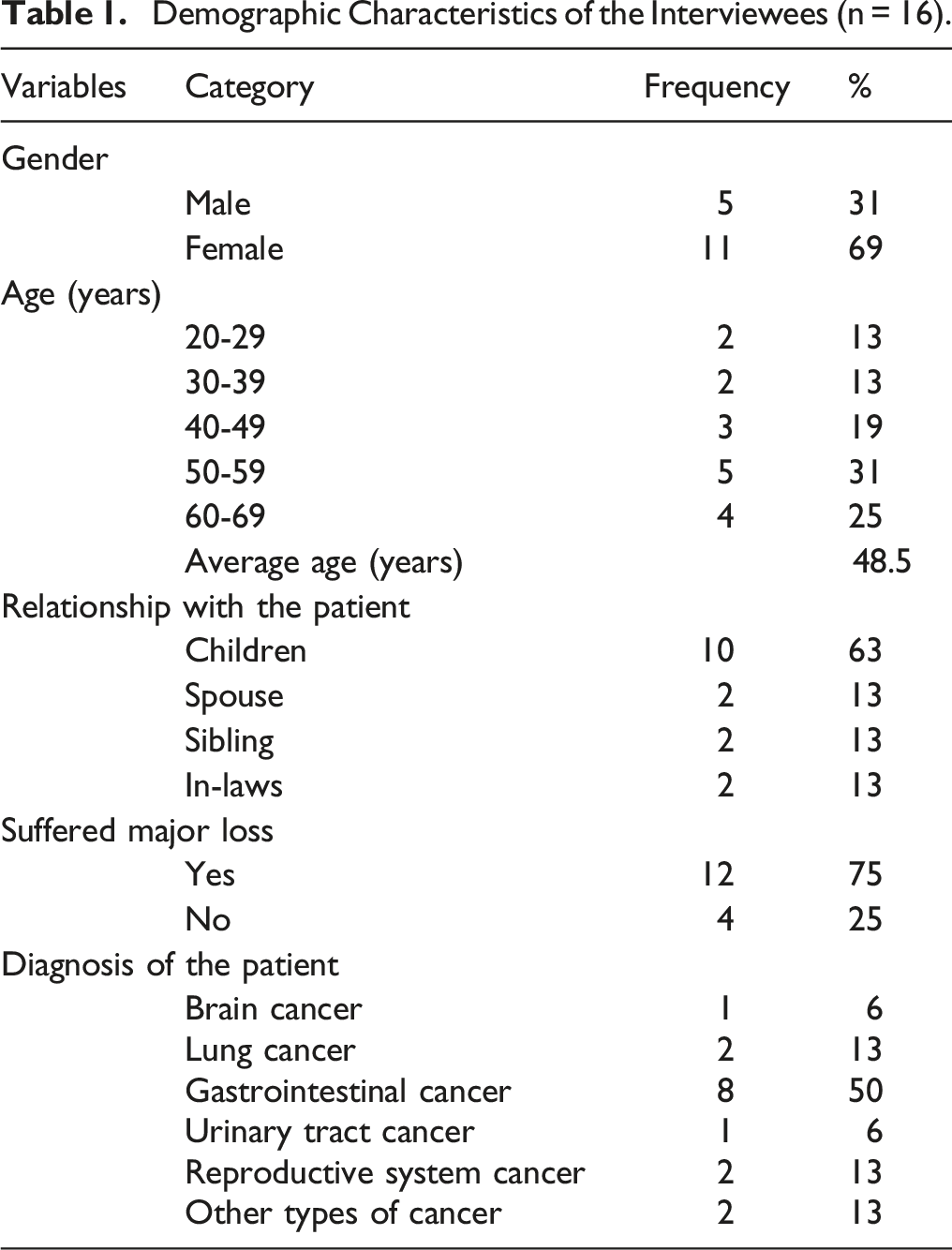
Results of Interview Records
In the study, we completed 102 decodings, re-selected similar concepts to reach the final 61 codes, and further summarized 14 categories according to the code content, after compilation and summarization, the interview data was categorized into four themes: the meaning and manifestation as to the essence of life, the art of coping with death, the realization and gift of death, and adapting, coping with, and controlling emotions. A detailed description of each theme is as follows:
Theme 1: The Meaning and Manifestation as to the Essence of Life
Life is the beginning of death, while death is the end of life. The experience and feelings that individuals undergo when placed between life and death have a significant impact on understanding the meaning and manifestation as to the essence of life. Including the main caregiver and the patient in the process of facing terminal illness and imminent death, because of the individual’s gender, age, and the difference in the patient’s life course, it reflects and responds, through the experience of life and psychology in the meaning of the essence of life. The sub-themes in the meaning and Manifestation of the Essence of Life include “Gender differences,” “Age differences,” and “Differences in life experiences.”
Gender Differences
The majority of the interviewed caregivers were women. Along with the influence of social roles defined by the society, many caregivers also unconsciously internalized the thoughts and beliefs associated with such roles. As a result, the belief that caregivers should be a “woman” was a common occurrence. Examples of relevant responses include:
“There are no other options, my mother relies on me, and I think that it’s better that I, the daughter, am the one who looks after her” (F03). “Taking care [of the sick members of the family] is a women’s responsibility after all (in Taiwanese Hokkien)” (F07).
“I am a man ... Oh! I’d be lying if I said I’m not sad! (Thinking) When the doctor first told me about her condition, I felt as if the sky was about to collapse. I didn’t cry ... When the pain is too great, you’re not able to cry! That’s me; I just don’t want to talk …” (M06).
Thus, the majority of our sample included women, who were willing to sacrifice their time temporarily and even alter their own career plans (hence, they usually were not the main income earner of the family).
Age Differences
The age of the caregivers and patient appeared to have a certain influence on the caregivers’ adaptation to grief. We classified differences in caregivers’ adaption to grief into two groups: differences due to patient age and differences due to caregiver age. Examples of relevant responses include:
“Since my mother divorced my father, I still like my mother. Although my father knew that my mother was sick, I came back to help. If my mother is gone, my father has my own family. I think I will be empty because I am with my mother. It’s the most talked about ... Is this home a home?!..” (F01).
“My brother is only 26 years old ... 26 ... 26 ... there are so many things he still hasn’t tried, are there? My mom studied palmistry. She said that the lifeline of my brother is fairly long, but ... there’s a fork (interruption, redirection, or life change); if he can’t survive this ... (sob) ... He’s just too young” (M09).
“He is 97 years old, and all my friends say that he has lived a well-lived life. But I would rather have him not suffer from any illness or pain ... He is my father; of course, I don’t want him to suffer” (F04).
Different age groups tend to be at different developmental stages of life; hence, their views on life are different. For F01, there were differences between losing a mother and losing a father, as the feeling of “home” is likely to change if a mother is no longer there. For M09, “the elder brother is like one’s father.” The emotional attachment between siblings is typically strong at this age. The thought of losing one’s brother generated strong feelings of loneliness.
Caregivers of those who are at much older ages tend to have more life experiences and diverse life events; as a result, they appear to be more capable of remaining strong while coping with the expected and unexpected loss of life.
“When I was younger, I was betrayed when acting as a guarantor, embezzled when participating in a loan club, and divorced from my husband. There’s very little in life that I haven’t experienced ... Yet I’ve lived through it all till now ... I have friends of the same age getting sick or (who have) died ... Death is inevitable ... the only difference is when it will come ... Am I right?” (F03).
Differences in Life-Experiences
Patients’ life experiences (whether smooth or eventful) appear to affect caregivers’ feelings regarding end-of-life stages. It is common for caregivers to feel angry when they feel life is unfair, when the patient’s life was considered eventful or unevenly anguished, or when the patient was forced to endure pain and suffering during the end-of-life stage.
“My parents got divorced when my mom was very young. She became ill right after the divorce... just a few years ago... And now, she’s lying there... (sigh)” (F08).
Similar feelings were also observed when the patients were known to sacrifice their happiness for others, were dying without having a chance to enjoy the happiness of life, or when exposed to suffering and pain:
“When my mom was young, she had to work with my dad at construction sites, living a thrifty life. Later on, she was tortured by illness. Now that we are [financially] capable of offering her [a better life]... she is sick and in pain...” (F08).
Theme 2: The Art of Coping With Death
People appear to have different techniques for coping with death. It is an art that individuals are obliged to learn in order to choose between courageously confronting death and moving forward or activating their “self-protection” mechanisms and retreating from reality. In the face of incurable diseases and the fact that a loved one is about to die, the primary caregiver’s response to internal self-pressure and external pressure, the turning point and expectation of the disease, and the time to facing cancer and death will all affect the primary caregiver’s feelings about death, facing the grief before death is like being in the realm of art, without personal experience and deep understanding, only after you accept this pain and the reality that you are about to lose, can you walk out of their shadows, and thus transcend, when You cried, and Finally, walked along with the monument in pain, only to find that the darkness gradually extended and disappeared, and the sun shone on your face across the black wall. We all hope that in the world of art, our close relatives have already escaped the shackles of the human world and flown to their own depiction of Heaven.
Changes in Medical Conditions and Hope for Survival
The speed of change in a patient’s condition appeared to influence caregivers’ mental and physical preparation for death. Rehearsing what needed to be done in the last days and beyond might also help caregivers cope with, and adapt to, these changes in order to relinquish their grief. Changes in a patient’s condition might also affect both the caregiver’s and patient’s daily routine. When the patient’s condition changes drastically, exploring methods to cope with the change appears to be beneficial for controlling perceived stress.
“My mother is in the late stage of breast cancer. The cancer then spread to the lungs, and later, she had an intracerebral haemorrhage. As a result, she was repeatedly hospitalized to both the intensive care unit and normal palliative care ward... After she was discharged from the hospital in March this year, she hasn’t been sent back ... Recovery...even the doctor said it was impossible...haha! (forced laughter)” (F01).
“The doctor told me that there were ways to extend his life, such as a combination of surgical treatment and radiotherapy. However, the chances of being cured were only 10%. He asked me to be mentally prepared for [the reality]... We listened to the doctor’s advice, went through the surgery, radiotherapy, and even treatment with Chinese traditional medicine, but the cancer spread to the brain. Later, we came to your hospital, as you provide target therapy. Now, although the application is approved... It’s of no use anymore” (F10).
Time Since Diagnosis and Awareness as to the Inevitability of Death
Time appeared to play a significant role in caregivers’ grief recovery. Caregivers’ grief seemingly reduced after a certain period of time compared to the moment that they were informed as to the patient’s diagnosis and unlikelihood of being cured.
“Since she was diagnosed 12 years ago... The cancer spread to her liver 9 years ago... For a moment, her condition stabilized; however, the situation didn’t last long. Her physical condition has been deteriorating ever since... Now, we are trying our best to cooperate [with the doctors and medical staff] and satisfy her end-of-life needs and make her last days relatively comfortable...” (M02).
The majority of caregivers wished that the patients could suffer less during the final days. Some hoped that the patients could be free from the pain of reincarnation, dismiss any confusion, and die peacefully.
“I prayed to my ancestors, asking them not to let my dad suffer too much in his last days. I also wished that the Bodhisattvas could come to take him so that he wouldn’t have to worry and be scared” (M12).
Theme 3: The Realization and Gift of Death
From the moment a patient was diagnosed with cancer and informed that a cure was not likely, the caregivers were by his/her side. The companionship of the main caregiver, depicting each other’s memories in the process, the accumulation of emotions in the movement of time, fluctuating due to the expression of mutual intimacy and emotion, affecting your and my emotional notes, reverberating In the journey of parting, through the power of social support and religion, strengthen the internal and external response, sublime the understanding and acquisition of spirituality in the suffering, and then complete and reinterpret and construct the meaning of life from it. In addition to stimulating caregivers’ reflection as to the meaning of life and death, this experience also allowed caregivers to embrace the positive side of human nature.
Social Support and the Power of Religion
Since caring for patients is often a task beyond the ability of a single person, effective support and assistance provided to caregivers appeared to be conducive to alleviating caregivers’ burden and stress.
“Now, I’ve dropped out of studies to look after my brother... Occasionally, when my parents are at home, they’d help me as well. However, [due to their health condition] moving around is not very convenient for them. Therefore, most of the time, I am the one by his side. Previously, when he was in the hospital, our maternal grandparents also came to help me” (M09).
“When my mother was first diagnosed with the illness, I had to frequently ask for leave. My colleagues were very understanding and took over my duty in turn. Since taking care of my mom [was not a temporary task], I applied for early retirement. My supervisors also offered to retain my position... Thinking of all the support they gave me really warms my heart...” (F14).
The power of religious belief was the most prominent when individuals had absolute faith in corresponding deities. Such belief often brought peace and appreciation for the assistance they received. However, when religious beliefs between the caregiver and patient were different, reaching a balance between the two beliefs appeared to be significant.
“I have been helping at the temple as a volunteer because I believe that the gods must be watching...Whatever we do, the gods are watching us. So don’t harm others... That way, things will unfold more smoothly...” (F03).
“The elder sister is a very devout Taoist. She believed that if the younger sister dies in July of the lunar calendar, she will go to hell... So she thought that it’s better that she makes it through July...” (F05).
Gain in Pain
When faced with a sense of loss generated by the fact that their family member’s illness was incurable, and that they may die in the near future, the majority of caregivers appeared to have no plan for a future life. Caregivers’ main focus was on daily patient care.
“Future...mine? I haven’t thought much about that. I have to wait and see [the patient’s health condition]” (M02).
It appeared that when caretaking tasks were shared among family members, the assistance helped primary caregivers release stress, as well as improve the quality of care provided. As a result, the family members were united under the same task and often became closer to one another.
“Other family members also take over some responsibilities. It may appear that I am the only one who has been busy all day long but, in fact, we all help and support each other. Both relatives from my parents’ side and those from my husband’s side help me during the process. It brings us closer...and helps us share the stress” (F11).
“In the past, I was not very social and am not good at communicating with others...and I didn’t know how to help others... But since my mother became ill...I should cherish this opportunity...be nice to the people around me and treat the events and things more seriously” (F08).
“When I was younger, I was with my mom during her last days and experienced the first funeral of my life... Now it’s my mother-in-law... It’s a different feeling though ...but I believe that having a beginning and an ending is something that one should experience in life! I’m perhaps still worried about having to suffer [when I become ill in the future], but compared to the people that haven’t had such an experience, at least I will be braver...and stronger!” (F07).
Theme 4: Adapting, Coping With, and Controlling Emotions
Caregivers’ adaptation and methods for coping with grief seemed to be affected by the progression of a patient’s illness and the proximity of the patient to death. Thus, it becomes a challenge to control and balance one’s emotions.
Loss-Oriented Coping
Some caregivers reacted either emotionally or evasively when informed of the fact that the patient was in the late stage of cancer. Caregivers’ responses toward this reality were generally negative, and their focus was on a sense of loss (loss-oriented coping).
“God is really cruel; he doesn’t give us any chance...such an unfortunate thing... (covers her face to cry). We are generous and kind-hearted people but look what we get in the end!” (F10).
“He used to be healthy and fit...then he had diarrhoea and it turned out to be cancer... Isn’t it weird? There’s no history of such illness in our family...he didn’t eat fried food, barbecue, or spicy food...maybe he was a bit overweight but...he just got cancer like that... (shaking his head)” (M09).
Restoration-Oriented Coping
Some caregivers applied a series of measures to adapt to, and cope with, the fact that the patient was very ill and nearing death (restoration-oriented coping). These caregivers often believed that death was part of a cycle of reincarnation: a causal circle between good and evil. Although the occurrence of the illness was not part of their life plan, caregivers often came to the conclusion that the sudden arrival of the disease was part of fate and that they should respect this arrangement. Such a coping mechanism appeared to be conducive to a smooth recovery from grief and sense of loss.
“Since the family believed in the Tiger God, we also burned incense and prayed to the Tiger God asking him not to make my mom suffer too much...not to make the last days too difficult and painful... What I can do as a son is to ask Tiger God to show the way, leading her to the reincarnation to a better life...” (M06).
These caregivers tried to change their attitude towards the last days of the patient’s impending death. The caregivers believed that it was better to accept the unfortunate event, make full use of the remaining days with the patient, and say goodbye. This mentality corresponded with the stages of anticipatory grief. By releasing sorrow and accepting the loss, the caregivers were able to approach the tragedy from a philosophical perspective and put more focus on a well-arranged departure and end-of-life stage for the patient.
“I just hope she doesn’t suffer too much...I signed a ‘Do Not Resuscitate’ order because I don’t want her to have to undergo chest compressions and electrical shocks on the way to the hospital...that would be a sad way to go...it will be best to just leave with no unsettled issues!” (F01).
“The bitter fruits that were planted in his past life, have been harvested, and the next stage will be Dharma joy... I read these in a book, and I found it encouraging...it helped me let go of the fear and sorrow of having to lose my husband...” (F10).
These aforementioned findings showed that when the caregivers realized that the patient’s death was not optional, caregivers tended to experience anticipatory grief. Furthermore, caregivers were also faced with many changes in their lives, as well as the emotional impact generated by the caregiving process. If such changes and impacts are not handled with proper coping strategies, the changes will likely increase feelings of grief. In many Eastern cultures, when death is expected for July of the lunar calendar, additional apprehension ensues. Furthermore, crying is often not permitted prior to the death of a family member, and even for several days following the death. Finally, gender differences are still apparent within the Taiwanese cultural context.
The present results also revealed that devout religious beliefs, acceptance of changes in a patient’s medical condition, receiving palliative home care, receiving social support, stress coping abilities, the ability to embrace change, and learning abilities had a positive impact on grief coping effectiveness. In addition, it was easier for caregivers to cope with grief when a patient did not suffer too much, when no regrets were espoused, and when the duration of the caregiving process was bearable. However, no conclusive results were observed in terms of the impact of the expected ness of death on caregivers' grief coping abilities.
Discussions
Major four themes emerged from the qualitative analysis (Figure 1). The present study revealed that primary caregivers' anticipatory grief experiences tended to continuously shift between four themes. However, it is not until the patient passes away that grief progresses into bereavement. This finding corresponds to the dual process model of grief proposed by Stroebe and Schut.
41
They suggested that during anticipatory grief, individuals tend to experience a dynamic process of oscillating between loss-oriented and restoration-oriented coping, as well as controlled and uncontrolled emotions, until mourners eventually regain their normal emotional status. In the present study, primary caregivers’ grief responses gradually decreased over time; however, when the patient’s illness became more serious, grief once again increased. In addition, grief responses appeared to differ based on the severity of a patient’s disease, as well as expectations regarding a prognosis. Such reactions are different from what is presumed by stage theorists, who argue that there is a linear grief process.14,15 According to the present results, the impact of a patient’s expected remaining days on a caregiver’s grief experiences was subject to various factors, including prior life experiences, culture, and traditions. In many Eastern cultures, if the death is expected to occur in July of the lunar calendar (a month that is considered bad luck for all important events), additional apprehension is experienced by both patients and caregivers. Major four themes emerged from the qualitative analysis.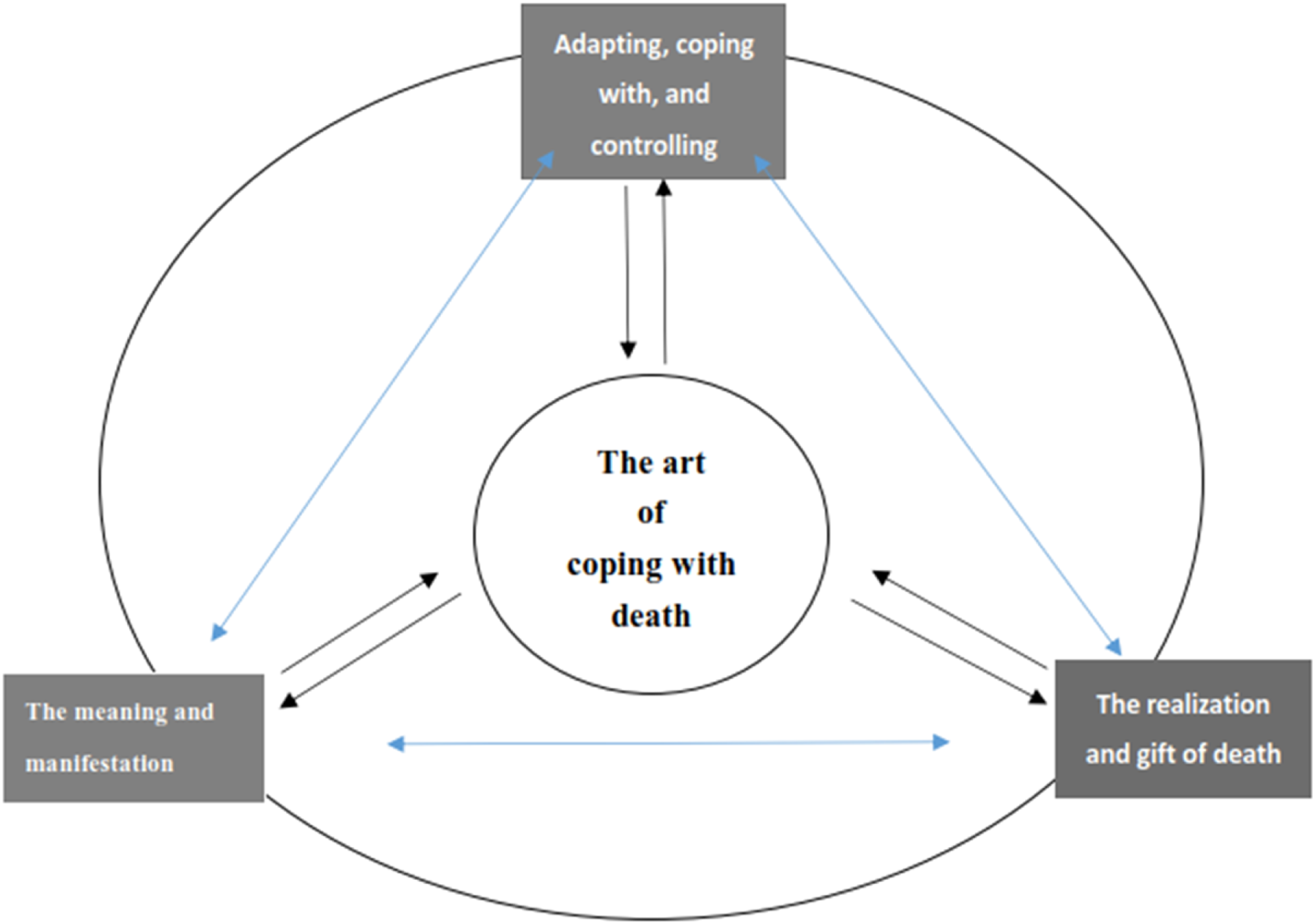
We also observed that gender differences emerged based on a Taiwanese cultural context. This differs from prior literature mentioning that gender does not influence expected grief.42,43 Furthermore, diversity among caregivers’ life experiences, rather than other demographic features (ie, age), appeared to influence anticipatory grief experiences. This is in keeping with prior work. 44
Previous studies have pointed out that primary caregivers tend to undergo tremendous stress and burden during the later stages of a patient’s disease. This is mainly caused by the several caregiving responsibilities present, as well as a caregiver’s family role.30,45-47 Given that primary caregivers, especially during end-of-life palliative care, have to deal with their caregiving workload while also managing the realization of an impending death, mental stress is greater than among primary caregivers of patients receiving active treatment. 1
The present study observed that anticipatory grief involves undergoing certain stages rather than remaining in a constant state of negative emotion. Moreover, some individuals tend to focus more on restoration and reconstruction rather than experiencing all emotional responses. This finding could be attributed to the Chinese mentality that “one should carefully attend to the funeral rites of parents and follow them when gone with due sacrifices.” 32 Furthermore, not all primary caregivers in the present study experienced pain and depression; some were able to develop a deeper understanding as to the meaning and values of life. Additionally, according to folk culture in Taiwan, crying is not permitted prior to the death of a family member, as well as for a certain number of days following the death, which counters other grief coping theories. 48 Thus, the relationship between Taiwan’s folk culture and individuals’ grief coping is worthy of further exploration.
Individuals’ complicated and unstable emotions, when faced with life and death, tend to affect their physical, mental, and spiritual peace while also impacting daily life functioning. Therefore, it is of great importance to understand caregivers’ needs at different stages of grief, recognize the cultural context, allow for three-dimensional connections between the caregiver and the deceased, help caregivers restore their normal life balance, regain self-recognition, and retain memories of the deceased in a non-distressed manner.24,49
Eastern and Western cultures have a different understanding of death. In many Eastern countries, the month of July of the lunar calendar is considered bad luck. 50 The majority of Taoism and Buddhism followers believe that individuals who die during July will not find inner peace. As a result, patients and families tend to apply unnecessary life-sustaining measures to postpone the date of death so as to ensure that it does not occur during July. However, such a practice contradicts the intent of “a good ending.”
Since many Eastern cultures tend to believe that the soul remains after death, people are more concerned about the whereabouts of the soul (eg, in either paradise or hell). Such concern and uncertainty usually increase fear and anxiety surrounding death. Therefore, it is worth exploring grief counseling measures within an Eastern context, wherein religion plays a significant role in society. However, corresponding knowledge and skills are not covered in today’s nursing education, which greatly hinders the effectiveness of anticipatory grief guidance.
Conclusions
The coping methods adopted by individuals in Eastern cultures when facing death were summarized accordingly. These findings could serve as a reference for understanding coping mechanisms from an Eastern context during anticipatory grief. It is expected that findings from the present will help scholars and practitioners obtain a better understanding regarding anticipatory grief experiences and the needs of primary caregivers. Thus, emotional support and psychological counseling can be developed accordingly; individuals with high levels of grief can be identified; effective support can be provided; and negative responses due to issues during grief adaptation and unnecessary medical expenses can be avoided.
Relevance to Clinical Practice
Potential relevance for the present findings include accepting Eastern cultural concepts of death, early intervention for hospice and palliative care to help with grief adaptation, case management and resource consolidation, and 24-hour telephone consultation services to reduce pressures on primary caregivers. Furthermore, professionals should regularly visit patients and caregivers, assess patients’ physical symptoms, and provide appropriate care guidance. Another important direction is to develop localized teaching materials for life-and-death education, implement tranquillity care in nursing education, cooperate with practical internships, improve end-of-life care skills, identify grief reactions and advocate for grief counseling, and help caregivers develop a new life and maintain a continuous connection with the deceased. Professionals can also assist with conducting case management and resource integration, understanding main caregivers’ care skills and abilities with responding to problems, assessing home care preparation before a patient returns home, help reduce a caregiver’s guilt, help caregivers accept “death as a natural process,” encourage caregivers to express their emotions (ie, grief mood swings are normal), build mutual trust, and provide an emotional support network at any time during the care process.
Footnotes
Acknowledgments
The authors would like to thank those who participated in the study, whose contributions have made this study possible.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.