
Abstract
Extensive research has focused on understanding and managing symptoms, such as pain, fatigue, or distress, in patients with advanced cancer.1-3 Research shows that, supported by an interdisciplinary care team, caregivers are involved in actively monitoring symptoms for home hospice patients and often act as a primary decision-maker regarding a course of intervention and administering care.4,5 Patient symptoms can be dynamic, often intensifying as death approaches 6 and caregivers report having a high number of unmet needs and report feeling unprepared for their role. 7 Thus, the caregiving role is often associated with high levels of burden and psychological distress. 8 Further, many caregivers are older adults and have their own health issues and related symptom experiences, 9 which may be exacerbated by caregiving. 10 Though many studies capture caregiver psychological symptoms,11,12 such as anxiety, depression, or grief, fewer capture caregiver physical symptoms, such as sleep, fatigue, and pain.13-15
Capturing caregivers’ report of both the patient and their own symptom data could provide additional evidence for targeted interventions. Symptom data, especially when paired with decision-support tools, can help hospice nurse care managers direct interdisciplinary care needs.16,17 There is strong evidence patient and caregiver psychological and physical health is highly interdependent, such that patient health can impact caregiver health and vice versa.18,19 For example, hospice cancer patient fatigue has been shown to significantly impact caregiver depression. 20 Similarly, the presence of caregiver chronic conditions have been shown to impact advanced cancer patient well-being. 21 Few studies have assessed the relationship between caregivers’ report of the patient’s health and their own symptoms over time, and particularly at end of life.
The goal of this study was first to describe home caregivers’ report of hospice cancer patient and their own symptoms over the last 2 months of the patient’s life, and second, leverage repeated measures to explore the day-to-day associations between these reports over time. We hypothesize that caregiver report of their own and patient symptoms will be associated over time, particularly as death approaches. Ultimately, this information could be guidance on the complex interactions of patient and caregiver symptom burden and potential avenues to intervene.
Methods
Study Overview
Data were collected as part of a multi-site longitudinal, observational study of cancer home hospice patients and their informal family caregivers (kin or non-kin). Caregiver participants were identified through participating hospice agencies between 2017 and 2020. Consent was obtained from the caregiver and also from patients if they were physically and/or cognitively able. At the home visit, the caregivers completed a baseline survey and were asked to complete daily symptom ratings for the patient and themselves via Interactive Voice Response (IVR) telephone reporting system based on the [previous study blinded] list of patient symptoms. 22 This study was approved by the Blinded Institutional Review Board (IRB_blinded).
Participants
Home hospice patients were considered eligible for the study if they were 18 years or older with a primary diagnosis of cancer, had a prognosis of 1 week or more to live, and had an eligible caregiver. Caregivers who were 18 years or older and could speak and understand English were eligible. Detailed screening and recruitment processes are detailed elsewhere. 23 The current study focused on caregivers where the patient died in hospice and only on the reports made while the patient was still alive.
Measures
Patient demographic data were recorded from hospice records. Caregivers completed baseline sociodemographic questionnaires and were asked to make daily automated reports to provide the presence, severity and level of distress of symptoms for the patient and for themselves within the last 24 hours. If a symptom was present, they were asked to rate on a 1-10 scale: (1) perception of patient symptom severity for 8 symptoms including delirium, depressed mood, diarrhea or constipation, fatigue, nervousness/anxiety, pain, poor appetite, and trouble sleeping; (2) level of distress caregiver was experiencing for each of the 8 patient symptoms; and (3) caregiver ratings of their own symptoms and outlook, including anxiety, depression, fatigue, trouble sleeping, guilt, sense of peace, and their sense of positivity. Single-item symptom reports are considered valid and reliable 24 and were selected to reduce burden for caregivers and because of their clinical relevance. 22
Analysis
Descriptive Statistics
Demographic variables were summarized. Symptom severity on the 0-10 scale was categorized into none (0), mild (1-3), moderate (4-7), and severe (8-10) in alignment with previous research.16,25 Items rating peace and positivity were reverse scored to align with other ratings. Descriptive statistics of symptom severity ratings and prevalence were calculated.
Symptom Dimension Reduction
To determine how caregiver-reported outcomes could be combined into fewer meaningful domains, exploratory factor analysis (EFA) was conducted in MPlus with Varimax rotation. To allow potential for differences in factor structure as death approaches, we conducted separate EFAs for 60-41, 40-21, and 20-0 days before death. To allow for missing data, factor mean scores were computed by prorated mean of the outcomes in each factor with a requirement that ≥70% of questions be answered. The number of factors to be retained were based on scree plot and examination of eigenvalues. 26 Benchmarks for simple structure in the rotated loadings include loadings ≥.40 on any single factor and <.3 for dual loadings. Combining results from the three EFAs gave a rough guideline for dimension reduction. Separate Cronbach’s alpha was conducted on each of the identified factors with criteria of ≥.7 for acceptable, ≥.8 good, and ≥.9 excellent internal reliability. 27 Inter-factor correlations are also reported.
Modeling Caregiver Reports Over Time From Patient Death
To explore the sequential associations between outcomes over time and as death approaches, we conducted a series of mixed-effects analyses with random intercepts (random effects) about the overall population average coefficient (fixed effects). No imputation or aggregation was conducted. For each factor identified in the EFA, we constructed a lagged value (prior outcome) representing the mean for the factor at the previous call. Full models for each of the EFA factors incorporated the following potential predictors and interaction terms: (1) autoregressive-lagged (eg the degree to which last report of
Results
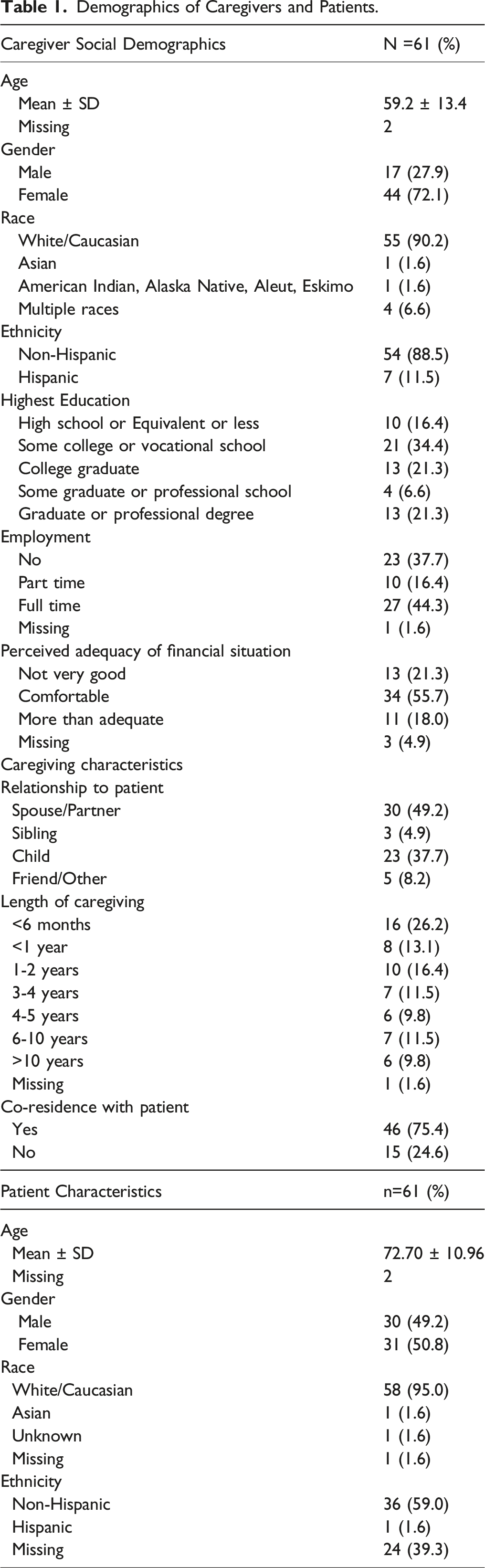
Demographics and Description of Symptom Report Reports
Demographics of Caregivers and Patients.
Symptom Prevalence
Prevalence and mean severity of symptoms at moderate or severe level.
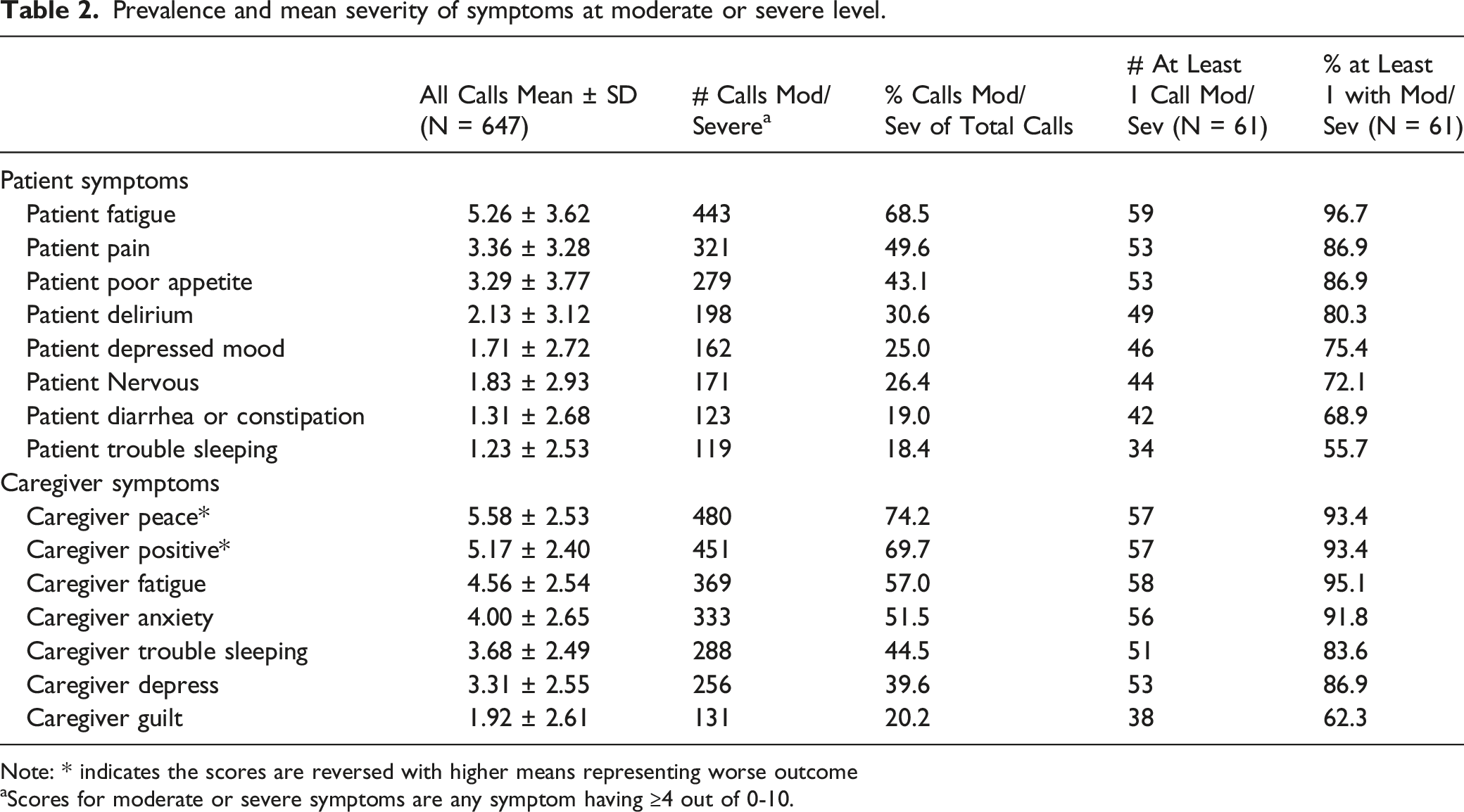
Note: * indicates the scores are reversed with higher means representing worse outcome
aScores for moderate or severe symptoms are any symptom having ≥4 out of 0-10.
Exploratory Factor Analysis of Caregiver Report of Patient and Their Own Symptoms
Exploratory Factor Analysis for symptom outcomes 60 days before patient’s death.
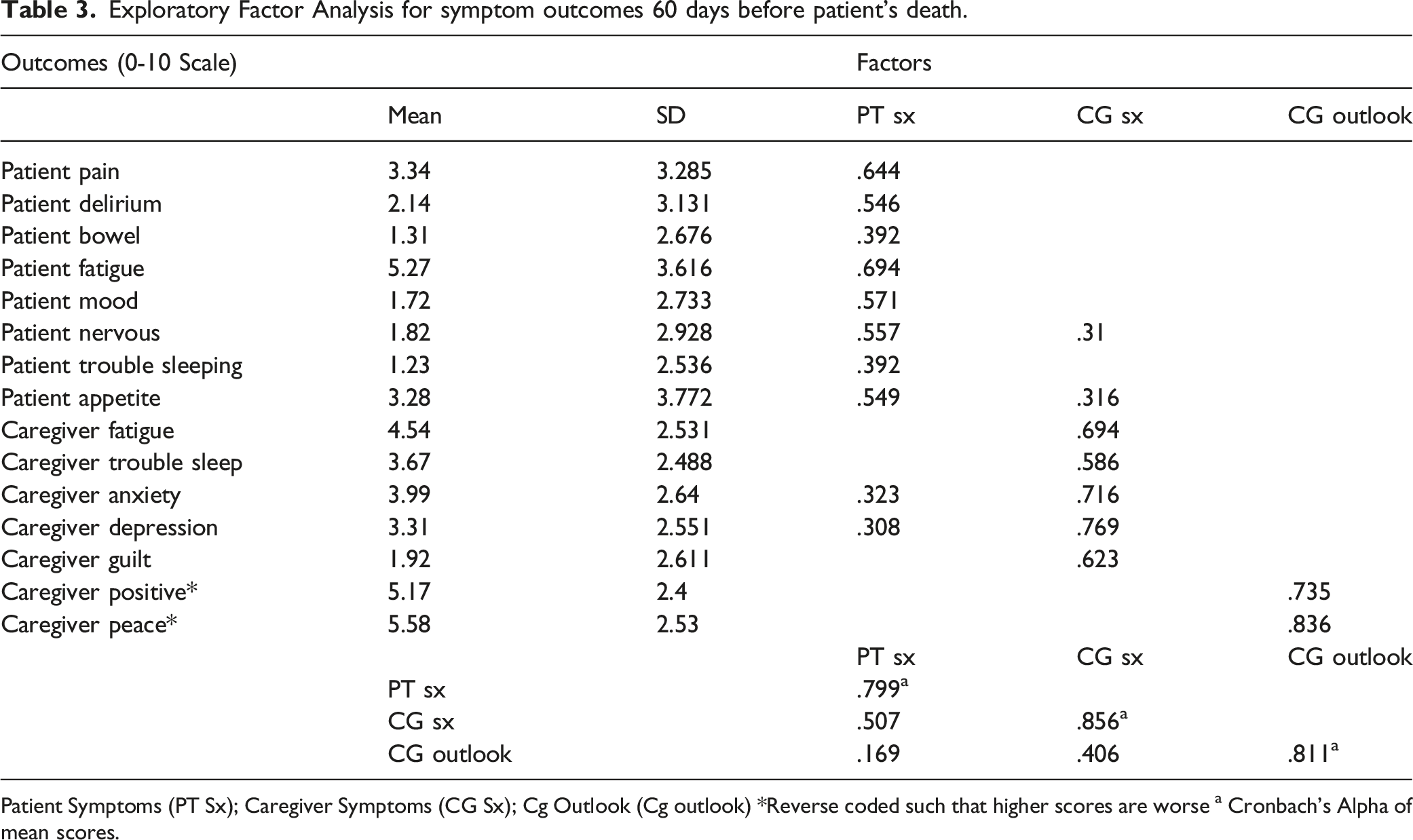
Patient Symptoms (PT Sx); Caregiver Symptoms (CG Sx); Cg Outlook (Cg outlook) *Reverse coded such that higher scores are worse a Cronbach’s Alpha of mean scores.
Sequential Relationships Among Caregiver Reports on Patient and Caregiver Symptoms
Sequential relationships of previous factors patient symptoms, caregiver symptoms, and caregiver outlook on current factors including the impact of associations as death approaches.
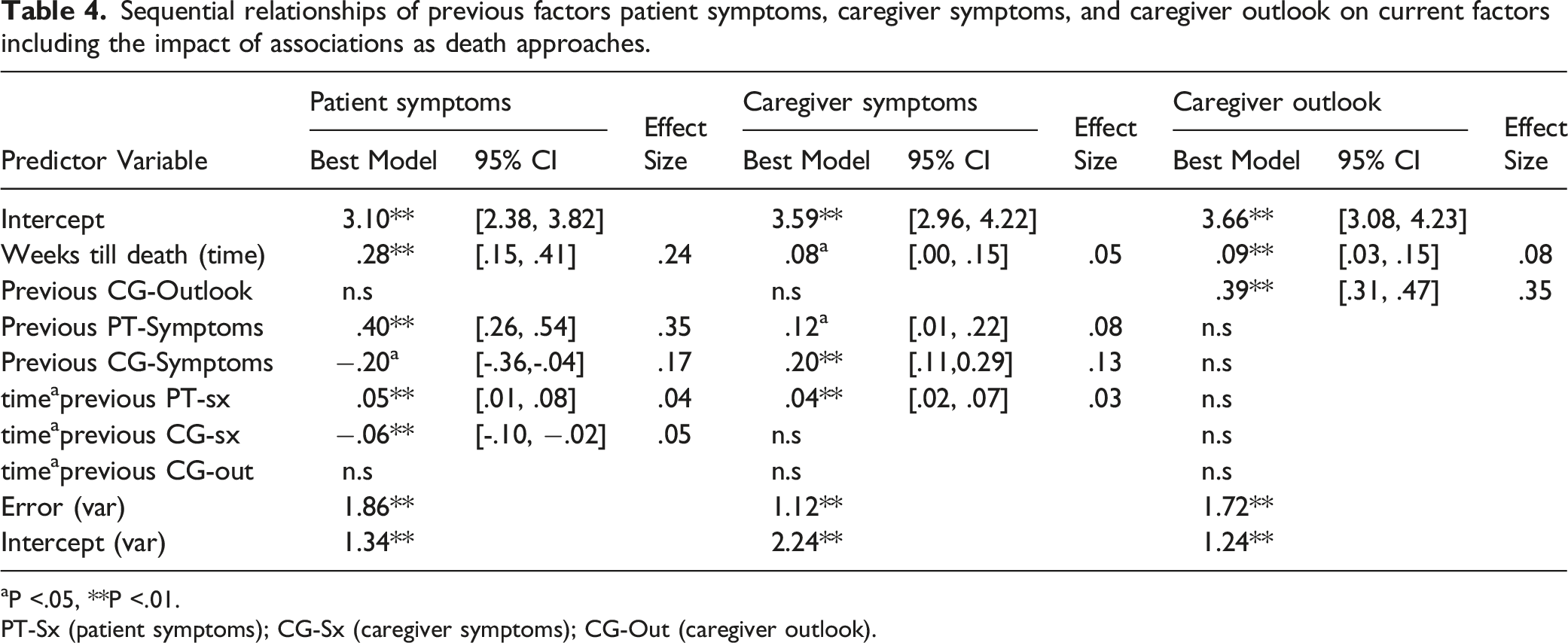
aP <.05, **P <.01.
PT-Sx (patient symptoms); CG-Sx (caregiver symptoms); CG-Out (caregiver outlook).
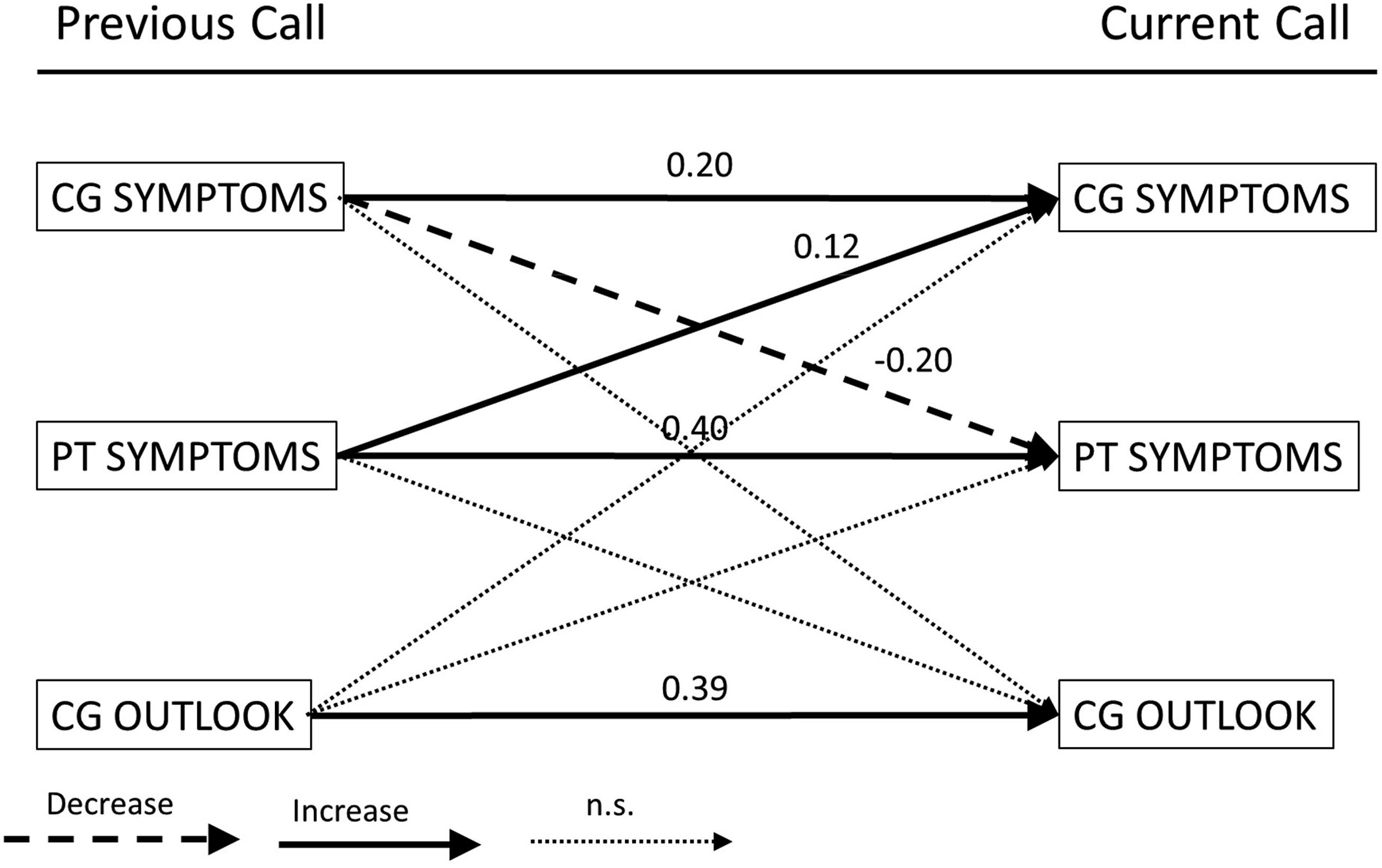
Lagged analysis results. Note: Each arrow defines the average fixed effect regression coefficient from the previous call outcome on current call outcome. Arrows from like outcomes are the autoregressive pathways (eg CP symptoms->CP symptoms) and those between different symptoms are the cross-lagged pathways (eg CP Symptoms ->Patient Symptoms). Because higher values represent worsening of the domain, significant positive coefficient is interpreted as previous call outcome leads to worsening or increase in current call outcome (solid arrows) while negative coefficients are interpreted as previous call outcome leading to improvement or decrease in current call outcome (long dashed arrows). Short dashed arrows represent non-significant (n.s.) associations. Cg: caregiver; pt: patient; n.s. = not significant.
As described above, models are composed of auto-regressive and cross-lagged predictors. There were significant autoregressive associations: previous caregiver symptoms positively predicted current caregiver symptoms (.2 95% confidence interval [.11, .29]), previous patient symptoms positively predicted current patient symptoms (.4 [.25, .54]), and caregiver outlook positively predicted current caregiver outlook (.39 [.31, .47]). For cross-lagged associations, caregiver symptoms and patient symptoms had significant cross-lagged associations, such that for patient symptoms, a one-unit change in previous caregiver symptoms results in a .20 decrease in patient mean current symptoms. For caregiver symptoms, a one-unit change in previous patient symptoms results in a .12 increase in caregiver mean current symptoms. There were no significant cross-lagged associations with caregiver outlook.
For all three outcomes, for each week approaching death there was significant worsening in severity with .28 increase for patient symptoms (P < .01), .08 increase for caregiver symptoms (P < .05), and .09 for caregiver outlook (P < .01). There were also significant interaction terms of the relevant past lagged predictors with death in weeks, such that (1) the magnitude of the impact of previous patient symptoms on current patient symptoms increased with proximity to week of death and (2) the impact of previous caregiver symptom on current patient symptom severity was stronger with proximity to death. For caregiver symptom severity, as patient symptom severity increased, there was a stronger negative impact on caregiver symptom severity as death approaches. There were no significant interaction effects for caregiver outlook (see Table 4).
Finally, there was significant variation for an individual’s overall symptom severity from the population average as reflected by the random intercept variance for all three outcomes. Variance for an individual’s predicted single factor score were also high for all three outcomes. These results suggest that there is unexplained between- and within-individual variance that is not accounted for in the current analysis.
Discussion
This study is one of the first to assess symptoms based on family caregiver report of both cancer home hospice patients and their own symptoms across time. In line with previous research primarily focused on cancer patient symptoms, 16 our study finds high proportion of reports of moderate-to-severe fatigue and pain, suggesting there is work to be done to improve symptom management at end of life in hospice. Although a limitation is that our patient symptom reports are made by caregivers, in hospice, daily patient care and hospice team response is often based on caregiver report. Even if caregivers are over-estimating patient symptoms, our findings suggest that this misperception still has important impacts on caregiver symptoms and outlook. Additionally, high levels of variability in all symptom reports exist both within and between individuals. While variability is expected due to the dynamic nature of hospice, systems are needed to help anticipate trends and alert hospice staff to address worsening symptoms. New technology can efficiently capture these changes and alert staff when visits should be intensified. 22
Few studies have specifically assessed daily reports of caregiver symptoms; our findings contribute to previous work noting hospice family caregiver physical and mental health are at risk.28,29 In addition to more physical symptoms, we also assess caregiver outlook variables of positivity and sense of peace. Growing research has identified positive aspects of caregiving, such as a sense of personal satisfaction, as protective for family caregivers. 30 Similarly, characteristics of spirituality, including peace, have been shown to be important aspect of caregiving and coping.8,31 The low levels of positive outlook in our study suggests there may be a need to better address these aspects in family caregivers. More research is needed to determine how caregiver outlook constructs such as peace and positivity interact with other more psychological and spiritual constructs, as well as the role they play in hospice caregiving.
A growing literature has demonstrated the relatedness of patient and caregiver outcomes.18,19 However, less work has assessed their interdependence over time. As symptoms can be dynamic, especially as death approaches, this is an important feature of the current study. As expected, the association between sequential ratings of patient symptoms strengthened approaching death. While the change over each report is small, it is statistically significant and because we asked for daily reports, this means that clinically-meaningful changes can develop over a relatively short amount of time. This finding reinforces the goal of addressing symptoms early--often it is more difficult to manage severe symptoms than minor symptoms—and provides additional evidence for the benefit of frequent symptom assessment.16,17
We also find the caregiver’s report of patient’s past symptoms is positively related to the caregiver’s own next symptoms, such that when the caregiver reports worse patient symptoms, the caregiver then reports worse symptoms themselves on their next rating. However, the caregiver’s past symptoms are negatively related to the patient’s next symptoms, such that when the caregiver reports worse symptoms for themselves, the caregiver actually reports better symptoms for the patient on the next rating. As death approached, these relationships between caregiver perceptions of the patient’s and their own symptoms strengthened, perhaps due to the increased need for care. One explanation for the somewhat counterintuitive negative relationship between caregiver symptoms and subsequent patient symptoms is that as caregivers work hard to improve patient symptoms, their perception of their own health and well-being suffers. Similarly, when caregivers believe patients’ symptoms are improving, this may produce complex emotions for caregivers; while glad for the improvement, some caregivers may view the improvement as a sign that the hard work of caregiving will be further extended. 32 Caregiving is often perceived as being a self-sacrificial act, 33 and evidence suggests caregivers are making this sacrifice without adequate resources and support.34,35 These exploratory and hypothesis-generating findings merit future studies. They also support continued research on promoting respite for caregivers and other psychosocial interventions.36,37
Limitations
This study is one of few to gather daily reports from caregivers of both patient and their own symptoms during home hospice care. Although patient reports can be difficult to obtain at end-of-life, there may be some bias in reporting based on caregiver perception. 38 More detailed standardized and validated questionnaires may also have captured greater precision in symptom reports. Our study also had missing data, and this may particularly impact our lagged analysis. Specifically, the sequential lagged analysis assesses the impact of the previous report on the current report which with missing data may not be based on reports on consecutive days. As such, our results likely underestimate the impact of perceived patient and caregiver symptom burden on current symptom reports. Furthermore, as this study was based on end of life and hospice care, there was heterogeneity in the timing of when participants joined the study prior to patient death. Thus, some caregivers had fewer opportunities to report on symptoms and consequently provided less information related to change in associations as the patient nears death. More complete datasets are needed to better understand the inter-relationships of caregiver reports of patient and caregiver symptoms. Further, additional symptoms not assessed in this study may have been important to patients and caregivers. A larger sample would also allow an examination of differences in symptom reporting by gender, race/ethnicity, and patient-caregiver relationship.
Conclusion
Symptom management continues to be an issue for cancer home hospice patients and their family caregivers. More policies, clinical services and interventions should be developed for family caregivers to better support their own health and protect their ability to care for the patient, particularly as they play a key role in hospice care.
Footnotes
Authors Contributions
Maija Reblin, Eli Iacob and Gary Donaldson conceptualized and designed the manuscript analysis. Lee Ellington was awarded funding to support the work. Maija Reblin and Eli Iacob wrote the first draft of the manuscript. Djin L. Tay, Megan C. Thomas Hebdon, Anna Beck, Kristin G. Cloyes and Lee Ellington contributed to later drafts. Eli Iacob, Hui Li and Gary Donaldson conducted analyses. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Nursing Research (Grant number R01 NR016249). Additional author time was supported by the National Institute of Nursing Research (T32 NR013456; MCTH) and the National Institute on Aging (K07 AG068185; LE).
Ethical Approval
This study was approved by the University of Utah Institutional Review Board (IRB_00033122). The authors certify that the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Data Availability
Data is available upon reasonable request from the corresponding author.