
Abstract
Background
Recruitment and attrition are inherently challenging issues in hospice research. We sought to describe strategies of recruitment, retention, and delivery of NOVELA (short for telenovela), an intervention for hospice family caregivers (HFCG).
Methods
Statistics were kept of every referral, consenting participant, visit session, and intervention activity. We used the Social Marketing Mix Framework to describe recruiting strategies employed and lessons learned.
Results
Two hospices in the U.S. Mid-Atlantic region referred 47 HFCG and N = 20 agreed to participate, out of which 50% (N = 10) completed all 4 sessions with an average of 2.8 sessions per person, each lasting an average duration of 13.5 minutes (range 8.0-25.7). The main reason for missing a session was a patient’s death (N = 8). Successful recruitment strategies employed in NOVELA included: (a) intensive start-up hospice engagement, (b) remote recruitment and delivery of NOVELA, and (c) scheduling flexibility to work around caregivers’ other demands.
Conclusion
The recruitment and intervention delivery had successes and challenges resulting in the identification of multiple opportunities to strengthen our strategy and inform future studies with HFCGs.
Keywords
Introduction
Research is important for improving knowledge, the quality of life for patients and their families, and the quality of care in the hospice setting. 1 However, research recruitment challenges in the hospice care setting are well documented. 1 Hospice care is a difficult and stressful time for patients and their family caregivers. Hospice enrollment is often late in the disease trajectory, within a few weeks of death, providing a short time frame to conduct research studies involving patients and caregivers. Family caregivers of patients receiving hospice care are often providing hands on care at home amidst of competing demands, making informed consent difficult in this population. In addition to patient/family-related factors, 1 particular obstacles in the hospice setting include lack of research infrastructure, few trained clinical researches, prioritization of clinical responsibilities, lack of protected research time and funding difficulties. 2 As a result, there are few adequately powered hospice clinical trials, especially, studies involving hospice family caregivers (HFCGs). 3
HFCGs, which include spouses, relatives or friends of a patient receiving hospice, are tasked with managing pain and other symptoms at home. For example, pain management is a demanding and multivariable task that involves managing medications and treatments, monitoring side effects, keeping track of pain severity, and communicating with the care team. 4 HFCGs encounter numerous challenges when caring for their loved one, which leads to low adherence to prescribed medications. 4 However, there is a lack of clear methods and recommendations on how to prepare HFCGs for managing patients’ pain and symptoms at home 4 thus, they request information and emotional support. 5
To address these unmet needs and built upon extensive preliminary work, 6 our project team, including hospice physicians, nurses, social workers and researchers, have produced a 4 chapter telenovela video series, To Care, which portrays the journey of one hospice family as they struggle with the decision to receive hospice care, manage pain, make healthcare decisions, and anticipate the dying process. Averaging 4:65 minutes, each episode addresses one of these challenges and was designed as part of the educational intervention, NOVELA (short for telenovela), to validate family experiences.
Is important that given the vulnerability of HFCGs, researchers must take care to place as little burden as possible on participants 1 while recruiting and delivering interventions in the hospice setting. The Social Marketing Mix (SMM) framework was proposed by White et al. 2 as a guide for researchers when planning and implementing recruitment strategies in palliative care. This framework consists of the 6 P’s: participants, product, price, place, promotion and partners. The recruitment strategies used in this study are compared with SMM principles to describe lessons learned. This study aims to address the following research question: How did the recruitment, retention, and delivery of the NOVELA intervention compared to Social Marketing Mix (SMM) framework?
Methods
Design
We conducted a pilot study to test an educational intervention for hospice caregivers, NOVELA, using a single-group pretest-posttest design. 7 Results of NOVELA intervention are published elsewhere. For the purpose of this study we tracked data related to recruitment, retention and intervention delivery and performed post-hoc comparison with SMM framework to describe lessons learned.
Participants
Study participants were HFCGs of patients who were receiving care from one of two hospice sites in the mid-Atlantic United States during November 2020 to June 2021. Inclusion criteria included: (1) HFCG older than 18 years, and (2) access to an internet device. Exclusion criteria included: (1) patients with a Palliative Performance Score of less than 20%, and (2) HFCGs unwilling to be recorded. The full trial protocol was approved by the Johns Hopkins University Institutional Review Board and is registered at clinicaltrials.gov (NCT 04533594).
Intervention
This intervention tested the use of a four-chapter telenovela video series, “To Care,” as part of a theory-based educational intervention, NOVELA. Each chapter addresses one challenge, including, decisions regarding hospice care, pain management, healthcare decision-making, and finally the dying process. Four online educational intervention sessions were arranged over 4 weeks. HFCGs met with a trained interventionist via synchronous web-conferencing. Participants used a personal web-enabled device (computer, smartphone or tablet). During the sessions, the interventionist introduced the purpose and topic of the video, facilitated video viewing, and then answered questions and reinforced the main messages for each topic. Each virtual session was video recorded, with participant permission, to enable monitoring of intervention fidelity and feasibility.
Recruitment Process
Hospice agency leadership determined social workers should present the program to potential participants during home visits. The study Principal Investigator (PI) held virtual meetings to train social workers in study protocol and demonstrated the intervention by presenting one video. A brochure with this information and a suggested hospice staff script were provided. Using recruitment strategies proven effective in our prior research,1,8,9 all caregivers were screened by hospice staff within 48 hours unless they had opted out or their loved ones were actively dying (PPS < 20%). Hospice staff emailed the research team with referral information, including, patient name, caregiver name and phone number. Then a phone session was scheduled by the research staff to go over the study in detail and obtain verbal consent to participate in research activities. During this call, an informed consent form was read aloud to the participant, with contact numbers for additional information as well as contact information for the University Institutional Review Board (IRB). If eligible and willing to participate, participants verbally consented and were scheduled for their first intervention session. The consent form was attached to a follow-up email with the link to complete the baseline measures.
Fidelity Protocol
The fidelity plan was based on the NIH Behavior Change consortium. 10 We addressed fidelity by creating a theory-based intervention (design), and developing an intervention manual for the purpose of interventionist training (training). In addition, we provided personalized feedback based on the audio and video recordings of discussion content from this pilot (delivery), used a checklist for study session about intervention engagement (receipt), and participants discussed with interventionist questions regarding video topics and intention-to-change behaviors (enactment). During weekly study team meetings, the interventionist and study team discussed study sessions, reviewed content and opportunities to improve intervention fidelity. To further evaluate receipt and enactment, two research team members used a fidelity checklist as a tool. We then took a sample of intervention video recordings to calculate protocol compliance using the checklist.
Data Collection and Sources
Data on the number of referrals, recruitment (consented) and retention (received intervention), number of sessions attended, video viewing (total time viewed), time spent in discussing each video and content of discussion were obtained from video recording reviews. To evaluate intervention fidelity (receipt and enactment), two investigators (GM and DC) reviewed a random subset of intervention videos using a fidelity checklist (See Appendix) to calculate interrater reliability (IRR).
Data Analysis
Descriptive statistics for referrals, enrollment, sessions attended, and delivering the intervention were computed with SPSS® v24 11 using frequencies and percentages for categorical variables, and means and standard deviations (SD) for continuous variables. Interrater reliability analysis using Cohen’s Kappa (κ) statistics12,13 and percent agreement 14 was performed to determine consistency among raters (GM, DCO) for intervention fidelity.
Results
Figure 1 presents the flow diagram of participant recruitment, enrollment, and intervention delivery. Of 47 referrals received from two hospice sites, 20 HFCGs consented and participated. The two most common reasons for not consenting were ‘not interested/too busy’ or because the patient had died before completion of the baseline survey. Attrition due to death after consent, but before the first intervention session was 4% (n = 2), leaving 18 participants that received at least one intervention visit but only 10 HFCGs watched all 4 videos. Recruitment, Enrollment and Intervention Delivery Flow Diagram. Out of 47 HFCG referrals received from hospice agencies, 20 HFCG enrolled to participate, of which 18 received at least one intervention session and 10 completed all 4 sessions.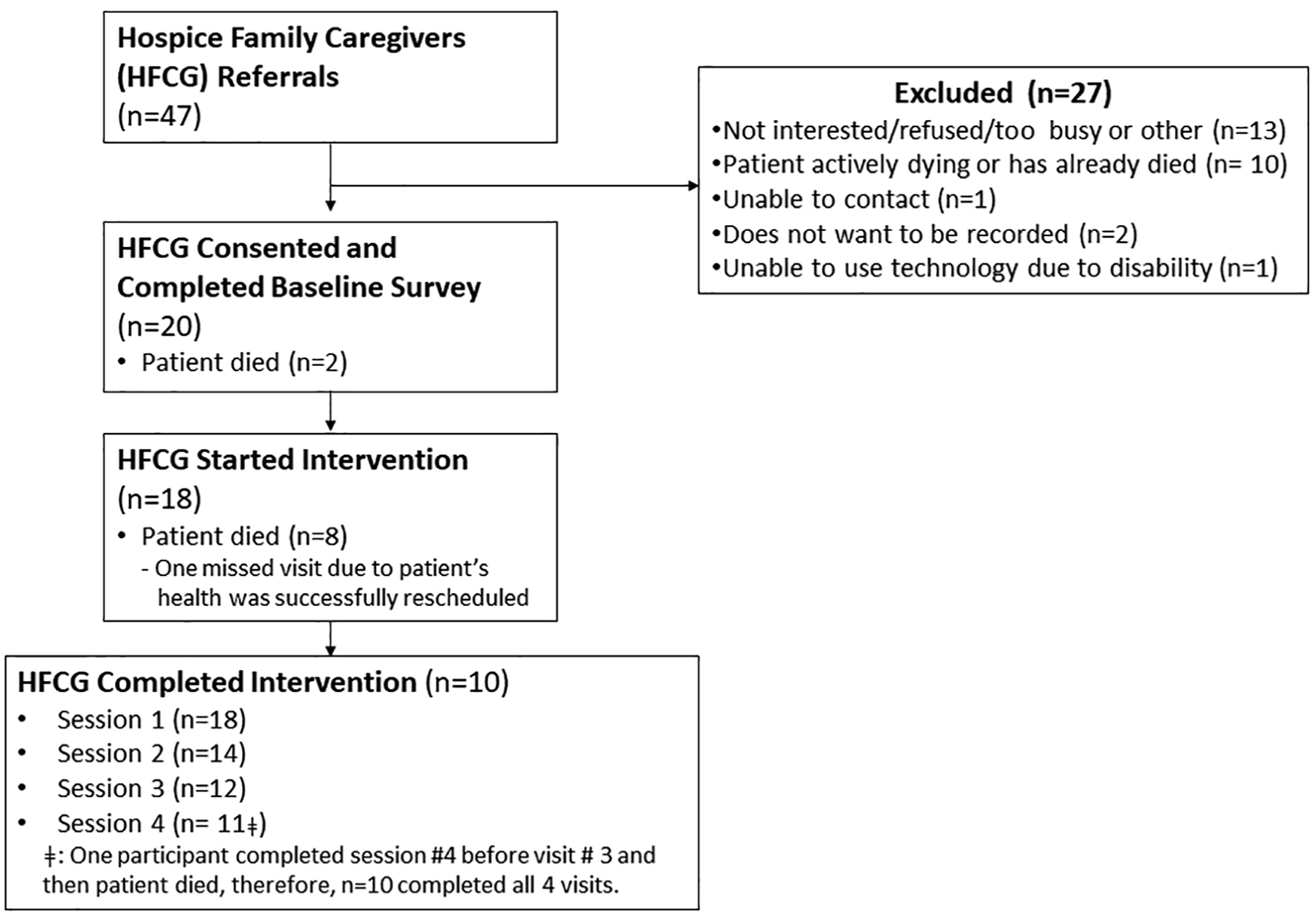
Recruitment Strategies Used Compared to Social Marketing Mix Framework (SMMF) (adapted from White et al. 2 ).
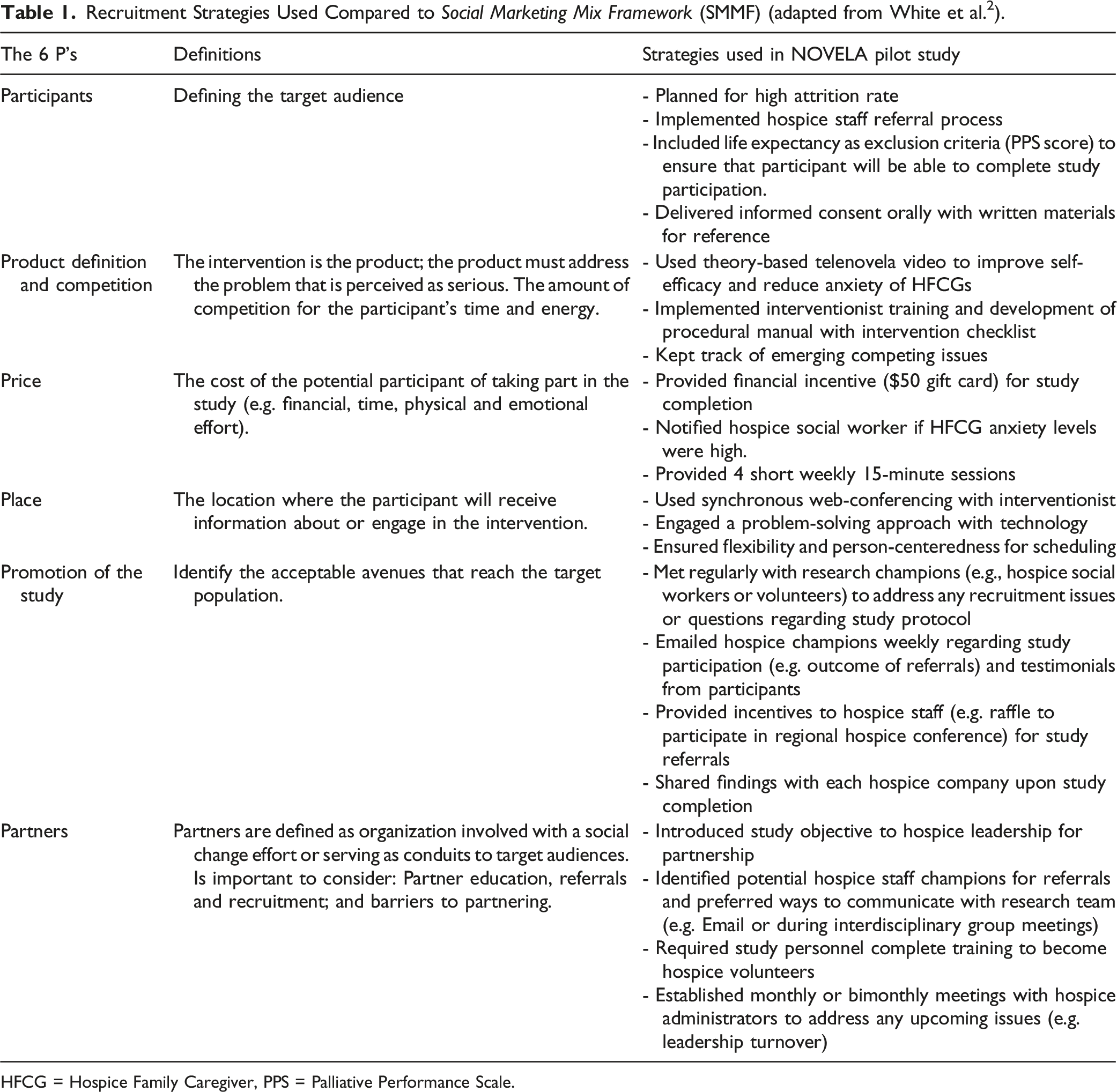
HFCG = Hospice Family Caregiver, PPS = Palliative Performance Scale.
The average hospice length of stay (LOS) was 139 days, average time in hospice before referral to the study was 69 days, and average time in the study was 48 days. After removing two outliers with more than 100 days on hospice, the average hospice LOS was 40 days (SD 19.44), average time in hospice before referral was 21 days (SD 18.95) and average time in study was 39 days. The average number of intervention sessions per person was 2.8 with each lasting an average duration of 13.5 minutes (range 8.0-25.7). Death occurred in n = 8 participants before completing the fourth telehealth session, and this was the sole reason for missing scheduled intervention sessions. While the average time of each video was 4.4 minutes, the average time introducing the video was 2.6 minutes and discussion averaged 6.5 minutes. A total of 55 telehealth sessions were performed. Intervention fidelity was demonstrated by 7.3 (out of 8 items) average number of items completed during each session and, overall, when calculating IRR there was substantial agreement, κ = .64 (P < .001, 95% CI (.26-1.00) 16 with 94% agreement 14 between the ratings of the two team members evaluating intervention fidelity.
Discussion
Improving hospice care depends in part on high-quality research. The challenges of conducting research in a hospice setting can be addressed through thoughtful study design that allows adequate time for preparation. 1 To date this is the second report describing HFCGs recruitment and research participation. We have implemented the NOVELA pilot study successfully in two hospices, enrolling caregivers amidst COVID-19 without any withdrawals.
Lessons Learned
Study procedures were designed to minimize burden to participants and hospice staff. Careful selection of inclusion and exclusion criteria helped us to avoid enrolling HFCGs of patients close to death (Participant). Even with careful planning, 8 patients died before the fourth video. The most important retention strategy was the virtual nature of NOVELA and the interventionist’s scheduling flexibility to work around HFCGs’ other demands (Place). Intervention duration of less than 15 mins/session and weekly frequency were acceptable to HFCGs (Price). This is in accordance with other studies17,18 suggesting that investigators must carefully weigh maintaining low burden against the desire for more participation time. It is important to lay the groundwork of connection from the first point of contact for an ongoing reciprocal relationship, using person-centered retention strategies. 17 Development and maintenance of a procedural manual helped to ensure that all members of the research team adhered to the approved protocol and that the interventionist’s delivery of NOVELA was consistent with the fidelity checklist (Product).
Preparation allowed us to establish relationships with hospice leadership and negotiate the recruitment process (universal screening vs referral-based). The support of the hospice medical directors helped us gain support from hospice leadership and teams (Partners). Training and involving hospice staff members in the study preparation process helped to minimize staff gatekeeping documented in other hospice studies. 19 Given the competing issues that emerged during study (e.g. leadership staff turnover and COVID-19 restrictions), adaptations to planned strategies included, engagement with hospice staff expanded beyond originally identified study champions, gift campaign to encourage 3 referrals per staff provided and recurrent participation in interdisciplinary group meetings established.
Both sites chose to use a referral process where their agency staff determined who was referred to the study, rather than an automatic referral process where the research team was allowed to screen all admissions. (Promotion). However, the referral process still allows a gatekeeping role and places the study referral burden on overworked hospice clinicians. The relationship with the staff was critical to a successful referral process. Our team was in constant contact with hospice staff and provided study insights as often as possible to help busy hospice clinicians remember to refer. Common limitations associated with provider referral studies include poor prognostic accuracy, gatekeeping, individual variation in interpreting eligibility, lack of time and incentive and poor generalizability. 17 In our study recruitment was hindered due to lateness of study referral, short hospice LOS and HFCGs’ time restraints. When a patient was too close to death the HFCGs’ ability to watch all 4 videos was impacted by their caregiving burden. As a result, only half of participants fully completed NOVELA. While universal screening on admission was not approved by either of our hospice sites, our results justify further hospice site engagement to consider alternative recruitment procedures. We have learned there may be value in obtaining the necessary privacy waivers and implementing a referral process that places the screening burden on the research staff at the time of hospice admission.
Limitations and Implications
This study is limited because the sample size was small and full analysis of the effects of time and intervention dosage was not possible. However, this pilot study provides important opportunities for modifying recruitment and intervention delivery in a follow up clinical trial. During study start-up ensuring hospice staff engagement was crucial for the initiation and maintenance of recruitment. The established relationships with hospice partners are ongoing and will be re-engaged into exploring ways to decrease hospice staff burden by considering a form of universal screening on admission. Further, a research team will be housed within each hospice to foster a sense of teamwork and promote sustainability of these efforts. Research referral earlier in the trajectory of hospice care could potentially enable delivery of at least 2 sessions per participant, as we think that one session is insufficient. Therefore, although virtual intervention delivery over 4 weeks was feasible, a shorter timeframe will increase the potential that more videos are seen. As we move forward, further exploration will allow us to determine the best way to tailor the videos to effectively meet the unique needs of each HFCG.
Conclusion
This report describes important lessons learned from recruitment, retention and intervention delivery of a pilot study with the intention of informing future studies with HFCGs. Research in hospice is vital to guide practice and improve patient care. While there are challenges, successfully run studies are possible when adequate attention is given to addressing study design issues and recruitment strategies put in place. Using the 6 P’s of SMM framework provides one potential structure to address these issues. 2 Our findings indicate that the current dosage of one intervention session per week is not sufficient to allow individuals to watch all videos before the caregiving burden becomes too great or the patient dies. Thus, an earlier study enrollment through universal screening is advised for advancing the timing of NOVELA.
Footnotes
Acknowledgments
We would like to thank Gilchrist Hospice, Seasons Hospice, and their family caregivers for their participation in this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Institute of Nursing Research (5U2CNR014637-09) through the Palliative Care Research Cooperative (PCRC) pilot project award. The content of this report is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Appendix
Fidelity Checklist
1. Greeted and checked in with participant on how he/she is doing
2. Introduced video
3. Followed most of the script
4. Performed at least one probe per required question
5. Took field notes of caregiver’s facial expressions, behaviors while watching video
6. Encouraged participant self-efficacy with successful use of caregiving strategies (i.e. Caregiver successfully managed pain; interventionist recognized progress and provided encouragement)
7. Ask learning lesson from video
8. Summarized main message of video emphasizing its learning point for participant to practice