
Abstract
Clinician-led conversations about future care priorities occur infrequently with end-stage renal disease (ESRD) patients on dialysis. This was a pilot study of structured serious illness conversations using the Serious Illness Conversation Guide (SICG) in a single dialysis clinic to assess acceptability of the approach and explore conversation themes and potential outcomes among patients with ESRD. Twelve individuals with ESRD on dialysis from a single outpatient dialysis clinic participated in this study. Participants completed a baseline demographics survey, engaged in a clinician-led structured serious illness conversation, and completed an acceptability questionnaire. Conversations were recorded, transcribed and thematically analyzed. The average age of participants was 68.8 years. The conversations averaged 20:53 in length. Ten participants (83%) felt that the conversation was held at the right time in their clinical course and eleven participants (91%) felt that it was worthwhile. Most participants (73%) reported neutral feelings about clinician use of a printed guide. Eleven participants (91%) reported no change in anxiety about their illness following the conversation, and five participants (42%) reported that the conversation increased their hopefulness about future quality of life. Thematic analysis revealed common perspectives on dialysis including that participants view in-center hemodialysis as temporary, compartmentalize their kidney disease, perceive narrowed life experiences and opportunities, and believe dialysis is their only option. This pilot study suggests that clinician-led structured serious illness conversations may be acceptable to patients with ESRD on dialysis. The themes identified can inform future serious illness conversations with dialysis patients.
Keywords
Introduction
Clinician-led conversations about goals and priorities with individuals with serious illness (serious illness conversations) are associated with enhanced goal-consistent care, including increased likelihood of a patient dying in their preferred setting, reduced hospitalization, less aggressive care at the end-of-life, and positive family outcomes.1-7 A randomized controlled trial of a systems-level intervention to improve serious illness conversations among patients with cancer found that intervention patients benefitted from more prevalent, earlier, and high quality conversations and experienced significant reduction in rates of moderate to severe anxiety and depression.8,9 Among dialysis patients, such communication has been shown to promote greater hospice utilization and may increase the likelihood that, in keeping with patient preferences, death will occur outside of the hospital setting. 10 However, these conversations occur infrequently in the dialysis population, 11 with some past efforts limited to promoting completion of documents for advance care planning and designation of health care proxies without deeper exploration of goals and values. 12
Barriers to serious illness conversations in the dialysis population include clinician reluctance to conduct conversations due to time constraints, prognostic uncertainty, and lack of communication skills training.
13
The Serious Illness Care Program is a multi-component healthcare delivery model that uses clinical tools and clinician training to address many of these barriers and facilitate serious illness conversations.14,15 The program promotes use of a Serious Illness Conversation Guide (SICG), which consists of open-ended questions about patients’ understanding of their illness, preferences for information, personal goals, fears and worries, sources of strength, critical abilities and tradeoffs, and how much their family knows about their wishes (Figure 1).
16
Using the SICG has been shown to be acceptable to patients with chronic kidney disease not yet on dialysis.
17
To inform dissemination efforts in the dialysis population, we piloted the SICG in a single dialysis clinic to assess acceptability of the approach and explore conversation themes and potential outcomes among patients with end-stage renal disease (ESRD) on dialysis. Serious Illness Conversation Guide reprinted with permission from Ariadne Labs.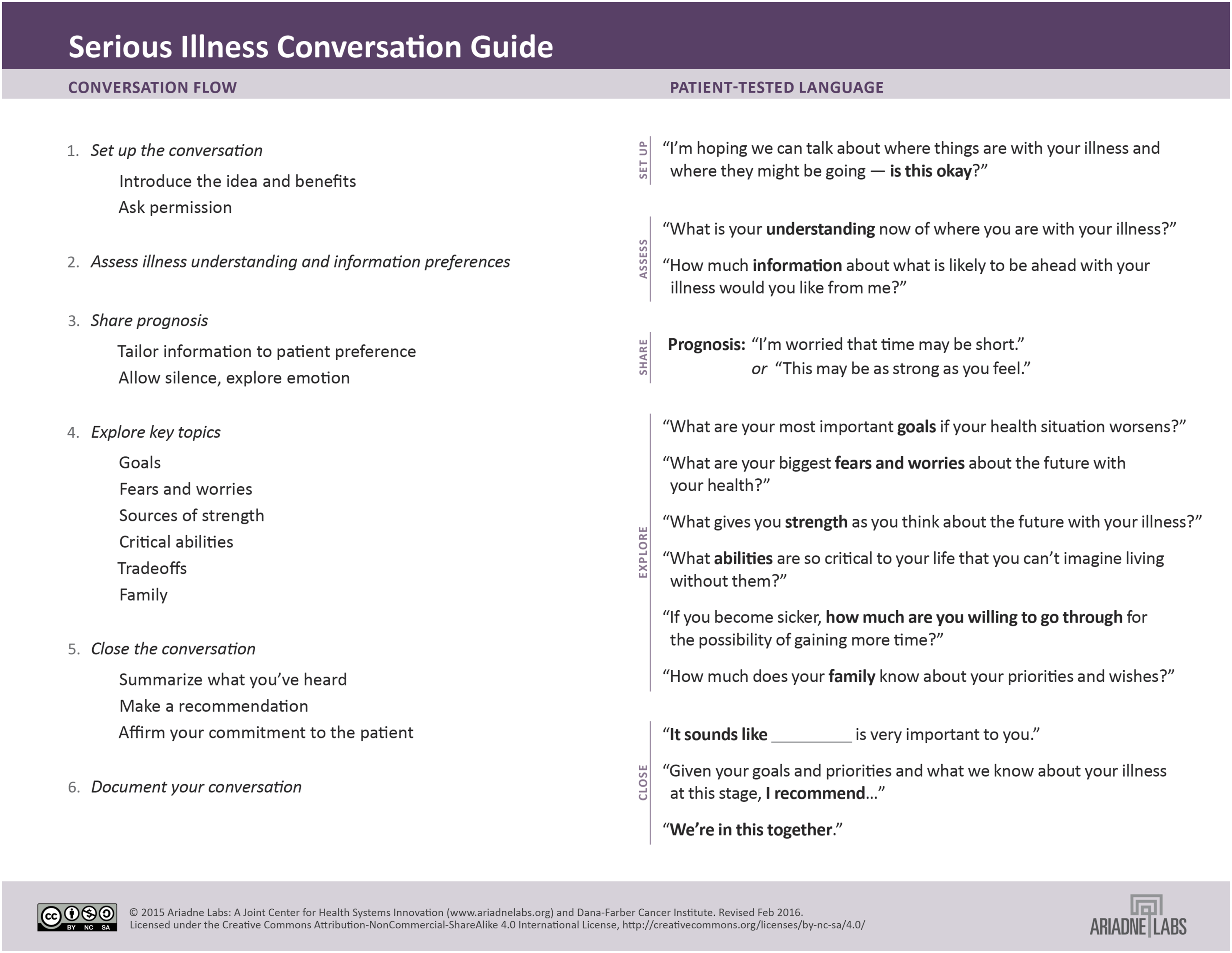
Methods
Design and Setting
This was a pilot study of clinician-led structured serious illness conversations using the Serious Illness Conversation Guide adapted for the dialysis population in a large, community-based dialysis clinic affiliated with a tertiary care center in Boston from October 2015 to August 2016.
Participants
English-speaking hemodialysis patients over 18 years of age at the dialysis clinic who were able to give consent were screened. All patients over the age of 60 were automatically eligible to participate. For patients under the age of 60, only those patients whose primary nephrologist answered “no, I would not be surprised” to the surprise question (“would you be surprised if this patient died in the next 12 months?”) were eligible to participate.
Enrollment Process
A non-study staff member approached eligible individuals and asked whether they would be willing to discuss participation in the study with a study staff member (pre-consent). For those willing, a study staff member explained the study and answered any questions, and individuals who agreed to participate were then consented and enrolled. The study protocol was approved by the Partners Healthcare Institutional Review Board as well as by the dialysis clinic parent company’s Administrative Review Office.
Intervention and Instruments
At baseline, enrolled participants completed a demographic questionnaire, clinical data was abstracted from the electronic medical record, and a conversation was scheduled with a dialysis clinician.
Dialysis clinicians included two credentialed nephrologists and a dialysis social worker, all of whom had been trained in a 2.5-hour session on the use of the SICG. Prognostic data was provided to clinicians in advance of the conversation in the form of 6-month, 12-month, and 18-month mortality predictions for maintenance dialysis using the Cohen 6-month Mortality Predictor. 18 By design, conversations conducted with the social worker did not include prognosis. Conversations were audio-recorded and transcribed.
After having a conversation using the SICG, participants completed an acceptability questionnaire and received a guide to help them communicate with family. Participants’ dialysis clinic electronic medical records were reviewed to ascertain status of documentation of the conversation within an average of 30 days of the conversation. Participant dialysis clinic charts were also reviewed at enrollment and 90 days after the conversation to assess for any changes in advance directives or identification of a healthcare proxy.
Analysis
Before performing the thematic analysis, a preliminary list of codes to categorize the data was established from the literature on serious illness communication and dialysis. Two study staff members (EIM, NJP) then independently coded the same set of three transcripts to identify additional codes and confirm coding. After finalizing the list of codes, NJP coded the remaining transcripts with EIM coding every third to ensure continued inter-coder reliability. EIM and NJP met to review and resolve disagreement by consensus. Investigators then conducted a structured thematic analysis. Coding and analysis were performed using the qualitative data analysis software program NVivo 10.0 (QSR International).
Results
Participant Characteristics
We screened 126 patients, of whom 62 were eligible. Forty-six agreed to the pre-specified pre-consent process and were approached by study staff (Figure 2). Thirty declined to enroll, with lack of desire to be part of a study as the most common reason, and four who initially enrolled did not complete the conversation (due to death, loss to follow-up, study withdrawal, and subsequently determined ineligibility due to language criteria). Twelve patients completed the study and were included in the analysis. Ten participants were over the age of 60; two under the age of 60 met eligibility criteria on the surprise question criterion. Those eligible but declining to enroll were of similar age (all eligible mean age 69.9 years vs baseline enrollee mean age 68.8 years) but more patients who declined enrollment had their clinician answer “no” to the surprise question compared to those who did enroll (36% compared with 17%). Screening and enrollment.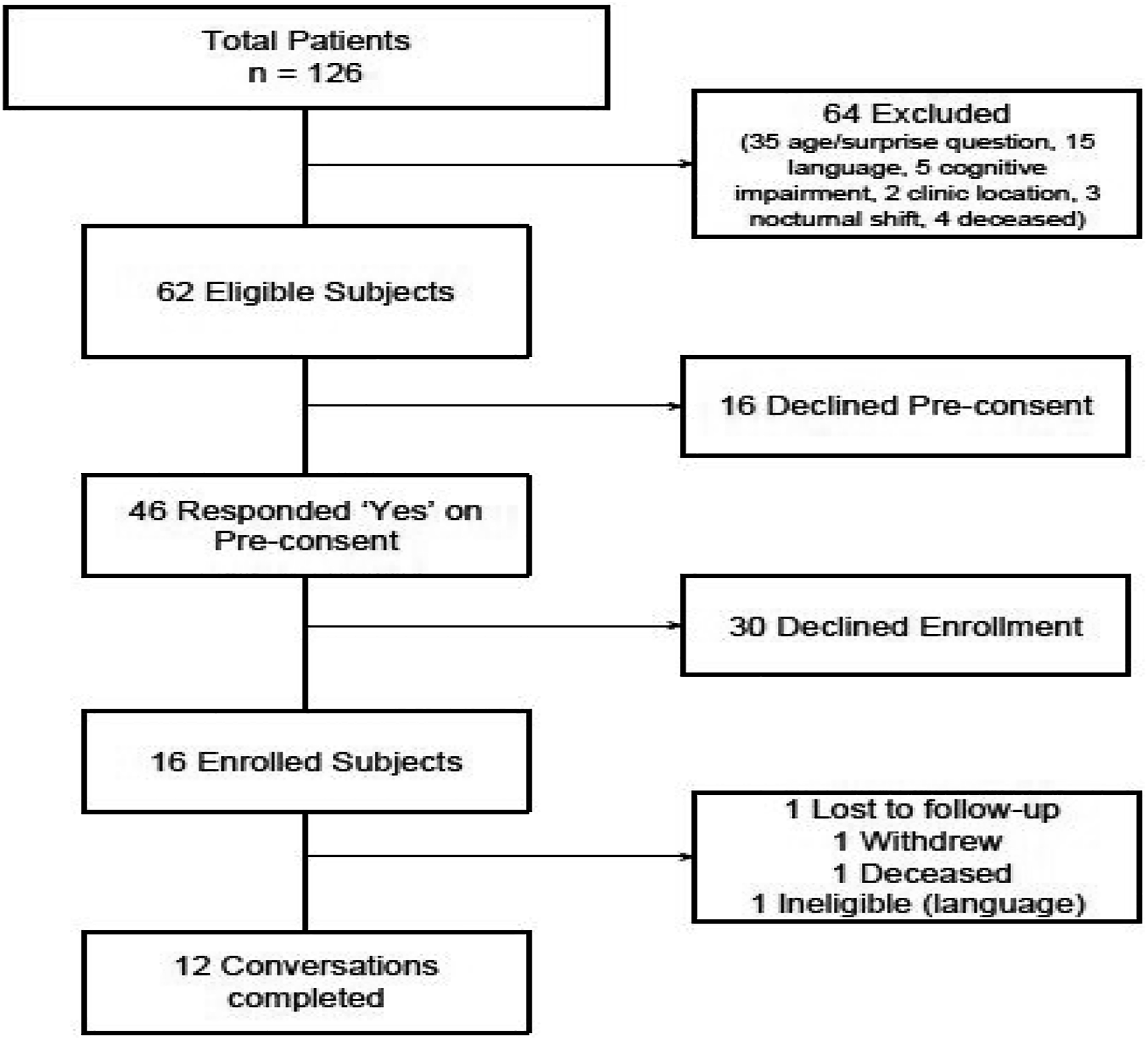
Baseline Characteristics of Patients at Enrollment.
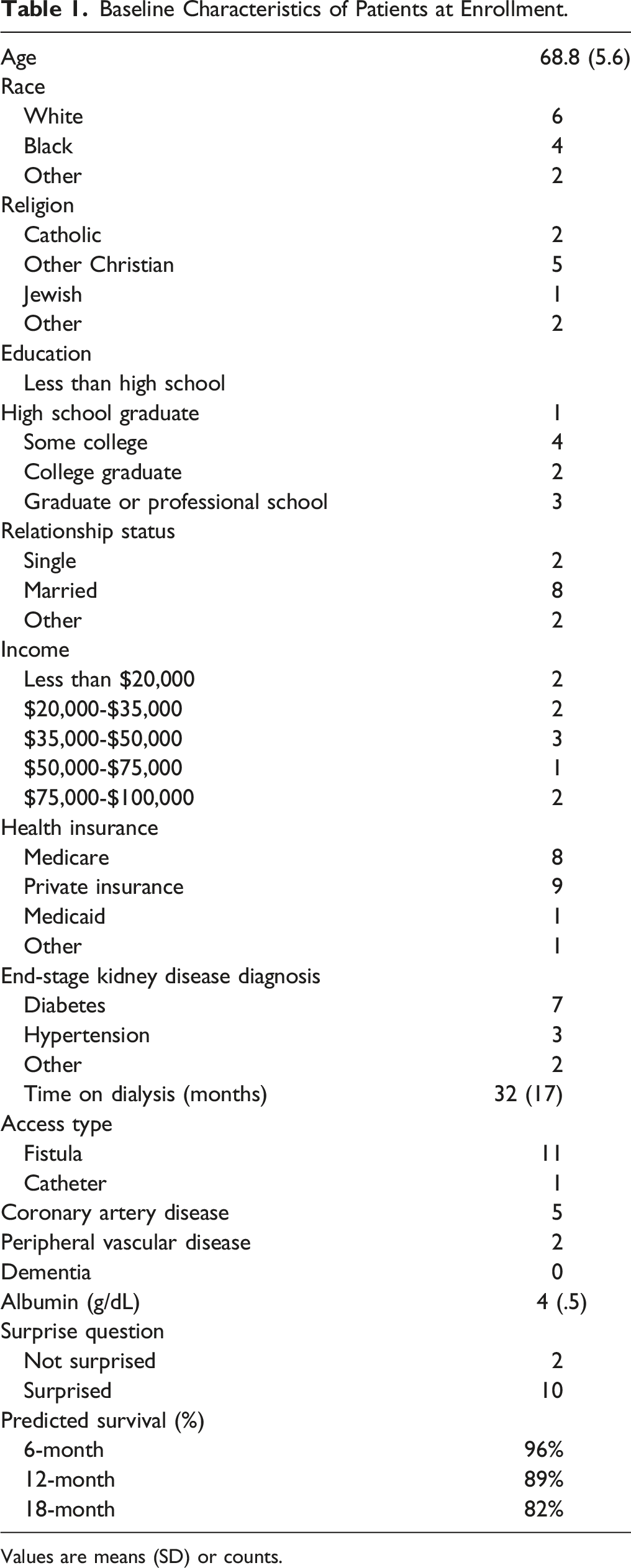
Values are means (SD) or counts.
Conversation Characteristics
The twelve conversations were all conducted at the dialysis unit. Three were conducted in a separate private room after dialysis due to clinician preference, while nine were conducted at the participants’ chairs during dialysis. Three were conducted by the patients’ primary nephrologist, five by the patients’ primary social worker, and four by the nephrologist-palliative care champion. Conversations were an average of 20:53 (SD 12:24) minutes in length. Nine (75%) conversations were documented in the EMR, eight of nine using free text and one using a provided template.
Post Conversation Survey
One third (33%) of participants noted they received the exact amount of information they wanted, 42% noted they received more than they wanted, and the remainder (25%) noted they received less than they wanted. Eighty-three percent felt the clinician had the conversation with them at the right time and 91% reported it was at least slightly worthwhile to have this conversation with the clinician. Nearly three-quarters (73%) reported a neutral (“did not notice” or “neither liked or disliked”) reaction to the clinician using a written guide during the conversation. Finally, 91% noted no change in their anxiety about their illness after the conversation, while 46% noted that the conversation increased their hopefulness about their quality of life in the future.
Content and Themes of Conversations
Thematic analysis of the transcribed and coded conversations yielded the following themes with representative quotes:
Patients View Their Experience with In-Center Hemodialysis as Temporary
Participants viewed their current experience with dialysis itself as temporary. This theme emerged in the context of discussing both goals and fears. Some participants viewed dialysis as temporary because they anticipated receiving a kidney transplant:
Clinician: What is your understanding now of where you are with your illness?
Patient: Ah, nearing a transplant. My whole goal right now to stay as
healthy as I can until I get a kidney.
Others were hoping to change schedule or modality, such as moving to a nocturnal shift or home hemodialysis to regain some control and independence:
I have plans to buy a motor home and get a smaller machine...do home dialysis
On the other hand, some participants understood dialysis to be temporary in that it would be beneficial and effective only for a limited period of time until it failed to provide necessary kidney replacement therapy and they would need to prepare for the end-of-life:
Am I going to be long-term on dialysis and if so how long would a person need to be on dialysis before, you know, it’s not really doing the best job for me….kind of wondering about how long dialysis can go until it doesn’t do its job.
Patients Compartmentalize Their Kidney Disease
Several participants did not see their kidney disease or dialysis treatment as the primary serious illness exerting the strongest influence on their health and survival. Some specifically noted that dialysis was only one of several serious illnesses they were facing, while others envisioned future morbidity and mortality exclusively outside the realm of dialysis and treatment-related concerns:
Keep in mind that the kidney business is not my only serious illness….I’m dealing with a couple of ‘em.
it’s that COPD [it] knocks [it] outta ya.
Patients Describe a Narrowing of Life Experiences and Opportunities
Participants described a narrowing of their life experiences and life choices as a result of beginning on dialysis:
In my life, I always considered myself a very dependable person. I tell you I’m going to do something I do….I now say to people ‘I am not that dependable anymore’….my life has become very, very small.
Participants also described the reality of their lives on dialysis as being characterized by poorer quality of life related to limitations in how they felt day-to-day and the extent to which they could engage in their usual activities:
I used to do this. I used to do that. It finally hit me, well you don’t do that anymore. That’s not who you are anymore. Face the facts, you know? This is who you are now. This is your life now.
Finally, several participants noted the limitations on travel that they perceived dialysis treatment to engender, negating their once-valued goals to travel to visit family overseas, explore for pleasure, or simply get away for an occasional weekend:
I was going to travel…I had already planned the places we’d go.
my goals would be…do the normal things I used to do…like trying to go places.
Patients describe choosing dialysis by default
Participants often perceived dialysis to be their only option. They described being presented alternatives to dialysis that included choosing either hospice or death:
When given the choice between hemo and I think my doctor was trying to be dramatic and he said ‘well, if it’s not hemo, it’s hospice.’
he said ‘you really don’t have a choice. It’s a hard decision but you know you are going to live or die.’
Impact of Conversations
Five of twelve individuals did not have an identified health care proxy (HCP) prior to the study. Only one of twelve individuals had a completed Medical/Physician Order for Life Sustaining Therapy (MOLST/POLST) or an Advance Directive, other than identification of an HCP, prior to the conversation. No new Advance Directives or MOLST/POLST documents were completed or created during the 3 months of follow-up. However, two of the five individuals without a designated HCP designated an HCP during the 3 months of follow-up.
Discussion
This pilot study explored the acceptability of the Serious Illness Conversation Guide as a tool to conduct serious illness conversations and promote advance care planning in the dialysis population. Despite a small sample size, the successful completion of a serious illness conversation for 86% (12/14) of those eligible and ultimately enrolled, the successful documentation of 75% (9/12) of the conversations, and the new identification of an HCP in 40% of those without a prior HCP, demonstrate the potential of employing a structured serious illness conversation guide such as the SICG in the dialysis population.
The time required for the conversation, approximately 20 minutes, is consistent with other advance care planning interventions as well as trials of the Serious Illness Conversation Guide in other populations8,15 and can be compatible with the work flow in the dialysis unit. Our approach provided options for conversation location which served to promote successful implementation, as both chairside and private room conversations were available and employed. Similarly, our approach to documentation was flexible, providing both a structured template and free text space, both of which were employed by clinicians based on their preference.
Clinician use of a structured conversation guide, which can increase the confidence of clinicians newly trained in conducting serious illness conversations, was acceptable to patients, with nearly three-quarters reporting a neutral response to its use. In contrast to study findings in those with cancer, who experienced significant and sustained reductions in moderate to severe anxiety, 9 participants in this study reported no change in anxiety about their illness after completing the serious illness conversation. However, nearly half noted increased hopefulness about their future quality of life, an effect similarly described in the cancer study. 19 A majority reported that the conversation was worthwhile and occurred at the right time.
Implications for Future Implementation
Several important lessons from this study may guide future implementation of the program in the dialysis population. Implementation requires a strategy to prioritize among existing dialysis patients. Our approach employed a simple age cut-off as well as a clinical metric, the answer to the “surprise question,” to capture younger patients most in need of a serious illness conversation. However, because few younger patients with clinician answer of “no, I would not be surprised” met eligibility, an age cut-off alone may be the best first approach in future implementation. In sharing prognosis, we primarily used a time-based approach, informed by the Cohen mortality predictor. 18 Future implementation could include a broader approach to prognosis communication beyond time-based prognosis, such as language to describe how one’s functional status might change, or one that emphasizes prognostic uncertainty coinciding with the possibility of sudden decline. 20 Our pilot used three different members of the interdisciplinary dialysis team to conduct conversations – the primary nephrologist, a non-physician member of the dialysis care team (social worker), and a nephrologist-palliative care champion embedded in the clinic. This three-pronged approach helped to mitigate the limited success in engaging primary nephrologists, a hurdle that needs to be overcome in future implementation. Yet this remains concerning as conducting serious illness conversations and promoting advance care planning for dialysis patients has been associated with enhanced goal-concordant care 21 and incorporates the shared decision-making approach that should be considered standard of care.22,23 Based on our experience, it may be that other members of the dialysis care team, such as social workers or advanced practice providers, are better positioned to receive training in, and conduct, these conversations.
The content of the conversations and the themes identified are also instructive. The theme that dialysis is seen as temporary has not, to our knowledge, been previously reported. Prior studies have reported that some patients regret their decision to start dialysis.11,24-26 Despite this regret, perseverance on hemodialysis may be explained by patient views that dialysis, or their current experience of dialysis, is temporary, pending clinical improvement, transplant, or switching to a preferred modality or schedule. Moreover, the notion that they will eventually fail dialysis or dialysis may cease to work for them may contribute to their continuing a therapy they otherwise regret having commenced, as they await an imminent and inevitable end to their dialysis experience. Perhaps most importantly, patients’ recognition of the limitations of dialysis and the need to prepare for end-of-life demonstrates the importance of, and the opportunity for, conducting serious illness conversations in this population. Similarly, the perceived limitations on quality of life and narrowing of possibilities that dialysis engenders also demonstrates the need for serious illness conversations to explore goals and preferences, and to repeat them as the patients’ clinical course, prognostic awareness, and priorities evolve.
Limitations
This pilot study has limitations. Consistent with previously reported data,13,27,28 we met resistance from nephrologists who declined to conduct the conversations with their own patients for a variety of reasons, including lack of time and discomfort with discussing serious illness. While utilizing a nephrologist-palliative care champion helped mitigate this challenge, few dialysis clinics have an embedded nephrologist-palliative care champion available to conduct serious illness conversations, limiting generalizability of the approach. We also experienced challenges in enrolling patients, with a large number expressing a lack of desire to participate in any research studies, making patient engagement another area for further exploration and improvement in future studies. While the participants who did enroll were of varying race, sex, religion, and socioeconomic status, their attained education level was particularly high, which, together with the small study size and the exclusion of non-English speaking individuals, significantly limits the generalizability. Finally, the limited success in enrolling eligible patients, as well the notably high predicted rates of survival among those choosing to enroll, raises the possibility of selection bias and further limits generalizability. Despite these limitations, this pilot study demonstrates one potential approach to implementing serious illness conversations and advance care planning in the dialysis population.
Conclusion
This study demonstrated some of the promise and challenges of using the Serious Illness Conversation Guide in a dialysis unit. Analysis of the content of the conversations yielded important themes that can inform future serious illness conversations with dialysis patients about their goals and values. This study was an important first step towards understanding the feasibility and value of larger-scale implementation of the Serious Illness Care Program in the dialysis population.
Footnotes
Acknowledgments
The authors wish to acknowledge the invaluable contributions of Ariadne Labs members, especially Richard Lawson, PhD and Christopher Kohberger, BA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Rx Foundation.