
Abstract
Background
The COVID-19 pandemic necessitated the transition from in person to virtual advance care planning (ACP) engagement efforts. This pilot initiative evaluated virtual group visits (GVs) and in-person GVs for ACP to determine their feasibility and effectiveness.
Methods
Participants included patients in a Geriatric Medicine clinic who were referred by their primary care physician to an ACP GVs intervention. The ACP GVs had 2 sessions, led by clinicians with ACP expertise who facilitated a discussion on patients’ values, goals, and preferences. Participants were provided with technical assistance to support use of the virtual platform. Evaluation included an ACP readiness survey, post-session feedback, GV observations, and electronic health record review at baseline and a 6 month follow-up for goals of care documentation and advance directives.
Results
Seventy patients attended 46 ACP GVs from August 2019 to February 2022, including 16 in-person GVs and 54 virtual GVs. At a 6 month follow-up, for virtual GVs participants (n = 54), goals of care documentation increased from 31% to 93%, and advance directives increased from 22% to 30%. For in-person GVs participants (n = 16), goals of care documentation increased from 25% to 100%, and advance directives increased from 69% to 75%. All surveyed patients in both formats would recommend ACP GVs.
Conclusion
ACP GVs are feasible and effective for supporting ACP, demonstrating an increase in both goals of care conversations and advance directives completion.
Keywords
Introduction
Advance care planning (ACP) is recognized as a process of preparing people and surrogate decision-makers for communication and medical decision-making.1-3 The concept of ACP has evolved into a holistic process over the life course that includes both in-the-moment and advanced decisions at every life stage. 4 Given the importance of implementing effective ACP interventions across the lifespan, primary care and ambulatory settings represent important opportunities to engage patients in the ACP process. Patients who have engaged in the ACP process have experienced higher goal-concordant care, improved quality of life, higher satisfaction with medical care, and eased burden of decision-making for families.5,6 Despite these advantages, many older adults do not take part in these conversations.
The Engaging in Advance Care Planning Talks (ENACT) Group Medical Visits for ACP has been shown to be an effective person-centered model, increasing older adult readiness to engage in ACP conversations and ACP documentation. 7 This ACP GVs intervention is based on Collaborative Learning Theory, which posits that: (1) learning is a social experience, (2) learners have diverse experiences and learning styles, and (3) learning includes the individual’s experiences alongside factual knowledge (ie, medical expertise). 7 The first of the 2-session GV format focuses on sharing personal experiences, consideration of personal values, and the role of surrogate decision makers. The second session focuses on challenges and questions from the first session and learning how to talk to a physician about medical decision making in the setting of serious illness. The ENACT GVs intervention was implemented as in-person GVs in a geriatric clinic and found to increase ACP outcomes including choosing a decision maker, completion of ACP documents, and ACP engagement. 7
Although telehealth approaches were not widespread prior to the COVID-19 pandemic, the COVID-19 pandemic necessitated the rapid transition from in person to virtual care. ACP engagement interventions became an important focus across health systems, including during hospitalizations, 8 emergency department visits, 9 and through the patient portal.8,10 Thus, although virtual GVs for ACP in older adults had not been previously studied, the increased use of telehealth and the need for ACP engagement suggested the need for a virtual ACP GVs intervention. Past studies have shown virtual GVs to be just as effective as in-person GVs for other medical care needs like diabetes mellitus GVs, Well-Child Visits, or fall-prevention workshops.7,11,12 This multi-year evaluation of a geriatric clinic ACP GVs initiative aimed to evaluate virtual GVs and in person GVs to determine their feasibility and effectiveness.
Methods
Setting and Population
The Geriatric Medicine Clinic at UCSD Health is staffed by geriatricians who care for more than 2600 patients aged 65 years and older per year. The average age of patients in the clinic is 81 years old, with 74% white, 8% Hispanic, and 39% male. The study included patients who were referred to in-person GVs between August 2019 and Feb 2020 and to virtual GVs between May 2020 and February 2022. The study was approved by the UCSD IRB as an exempt study.
Intervention: In-Person and Virtual Group Visits (GVs)
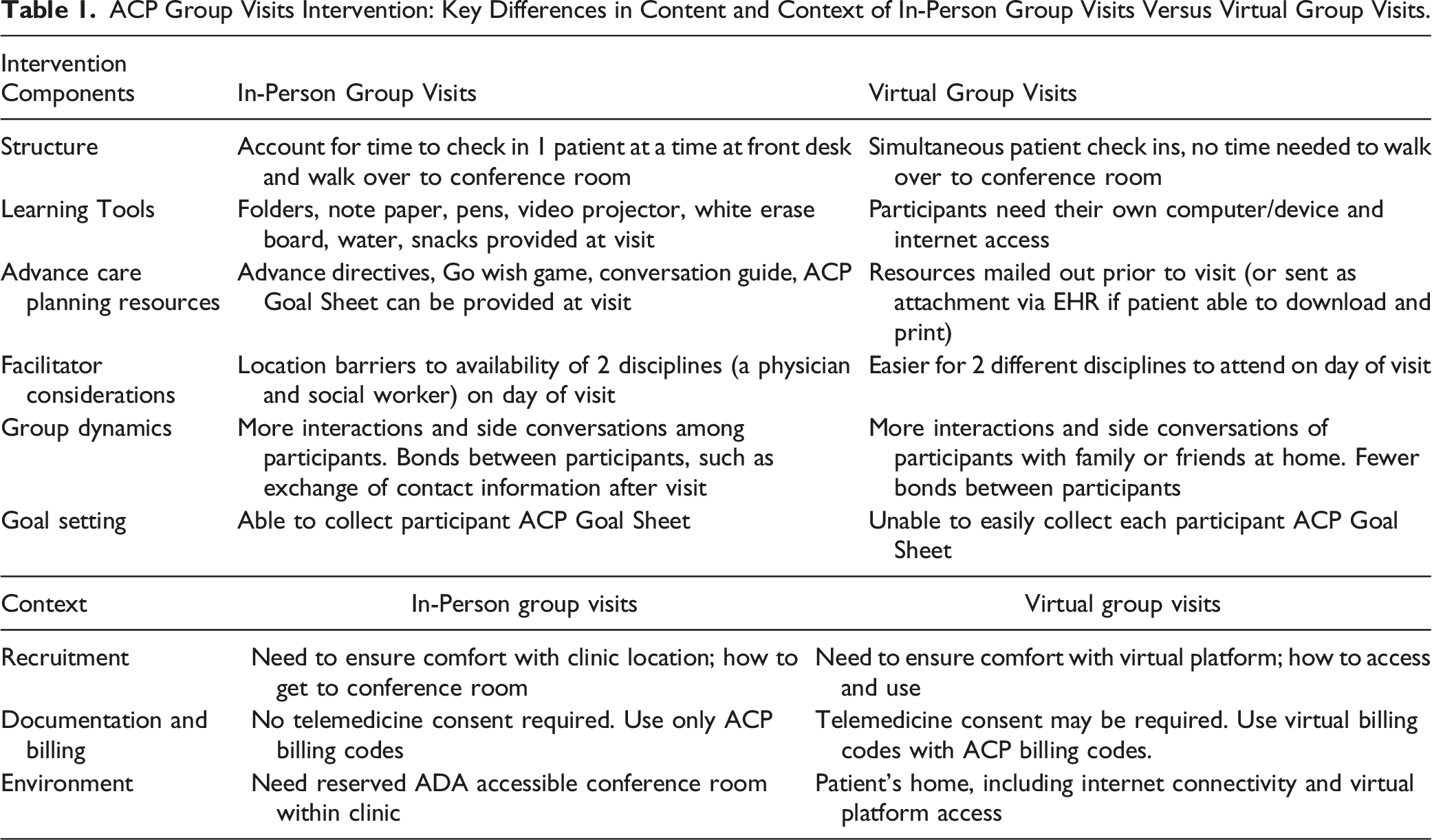
The ENACT GVs intervention was implemented as in-person GVs prior to March 2020 and as virtual GVs, starting in May 2020. Both visit formats invited a group of participants aged 65 years and older to participate in 2 group sessions that are each 2 hours long and 1 month apart. As described, the group facilitation focused on a discussion with interaction among patients about ACP topics. 11 The first ACP session focused on sharing personal experiences about ACP, consideration of personal values, and choosing and understanding the role of surrogate decision makers. The second session focused on follow up of ACP topics discussed in the first session and learning how to talk to a physician about end-of-life care. Participants were encouraged to complete a legal medical durable power of attorney form (MDPOA), or verbally choose a medical proxy if they were not yet ready to provide a written one. Family members were welcome and encouraged to attend with the patient, which was common for cognitively impaired attendees. Patients from both ACP GVs formats were encouraged to bring copies of preexisting or new advance directive documents or out-of-hospital orders to be scanned into the EHR the next time they came to the clinic.
ACP Group Visits Intervention: Key Differences in Content and Context of In-Person Group Visits Versus Virtual Group Visits.
Implementation Strategy
All patients in the geriatric medicine clinic were eligible for referral and primary care providers were asked to refer any English or Spanish-speaking patients who they felt would benefit from a facilitated discussion with their peers about ACP. From August 2019 to November 2020, participants were also referred to ACP GVs by flyers posted in clinic exam rooms or given to them at clinic appointments if they did not already have an advance directive on file. These flyers contained a phone number with instructions for participants to call to schedule. In December 2020, an EHR-based referral order was developed to enable primary care physicians to directly refer patients. Clinic administrative assistants utilized an EHR referral work queue to call and schedule patients for the GVs sessions, send appointment information via the patient messaging portal, and send patient materials via mail.
A large part of the implementation strategy was conducted by volunteers. The volunteers, mainly University of California at San Diego undergraduate students, did the UCSD health system volunteer training, as well as more specific training in palliative care (i.e. filling out their own advanced directive, becoming Communication and Advance Care Planning certified, reading papers, etc.). In this flow, volunteers called referred patients to confirm interest and conducted pre-visit surveys. They also ensured participants were prepared with the proper zoom link, zoom instructions, and reference materials received via mail. Clinic staff and volunteers were present to provide support, as well as take notes on each participant’s contributions to the discussion.
A physician facilitated all the workshops. Though it was originally planned for a social worker to also be present, there were only 3 sessions total in which a social worker was able to attend. The workshops as well were billed using ACP and/or Virtual Billing codes.
The interdisciplinary team, including geriatricians, nurses, administrative assistants, and student volunteers, met on a biweekly basis to coordinate upcoming roles and troubleshoot any issues.
Evaluation
All GVs were evaluated using the RE-AIM framework: Reach (percent of potentially eligible participants who attended a visit), Effectiveness (primary outcome of EHR-based clinical goals of care conversation note; secondary outcome of advance directives in EHR), Adoption (proportion of geriatricians who referred patients), Implementation (acceptability and participant feedback). 15 Maintenance was not evaluated. Referrals and attendance were tracked using a secure REDCap database. Patient demographics were collected from the EHR. Patient-level ACP data, which includes goals of care conversation and advanced directives, was from August 2019 to February 2022, including baseline prior to participating in an ACP GV and 6 month follow-up after participating in an ACP GV. With the continuation of virtual GVs for ACP throughout 2022, participant feedback on feasibility continued after February 2022.
All session attendees completed post-session evaluations to assess the ACP GVs’ acceptability using a 5-point Likert scale and a question with a free text response. 11 The survey included 7 statements such as (1) The group visit setting is better for talking about ACP than a normal visit, (2) The group visit gave me useful information, (3) I felt comfortable talking about ACP with other people in the group, (4) Talking with other people about ACP was helpful, (5) I feel the group visit addressed my specific concerns, (6) I feel able to discuss ACP with my regular healthcare provider, and (7) I would recommend these group visit sessions to a friend. The eighth question was a free-response question where participants could provide feedback about the session in general and regarding the virtual format (“Please let us know how it worked for you. What went well? What didn’t go well?”). Participant feedback was recorded verbatim. The free-text responses were read by 2 research team members and groups according to themes related to implementation of the group visits. Exemplar quotations of participant feedback are presented.
Volunteers did emphasize post-session evaluations, however patient participation in these evaluations was a consistent challenge. So, volunteers began conducting post-session evaluations at the end of each visit after the main information had been given to reduce the need for follow-up calls post-visit.
The ACP GVs implementation team conducted post-session debriefing. ACP GVs facilitators shared notes on unsolicited patient comments during the GVs and captured immediate impressions from group facilitators (volunteers) regarding the session, namely notable characteristics, barriers or limitations to patient engagement and areas for improvement.
Results
Reach
Demographics of ACP Group Visits Participants.
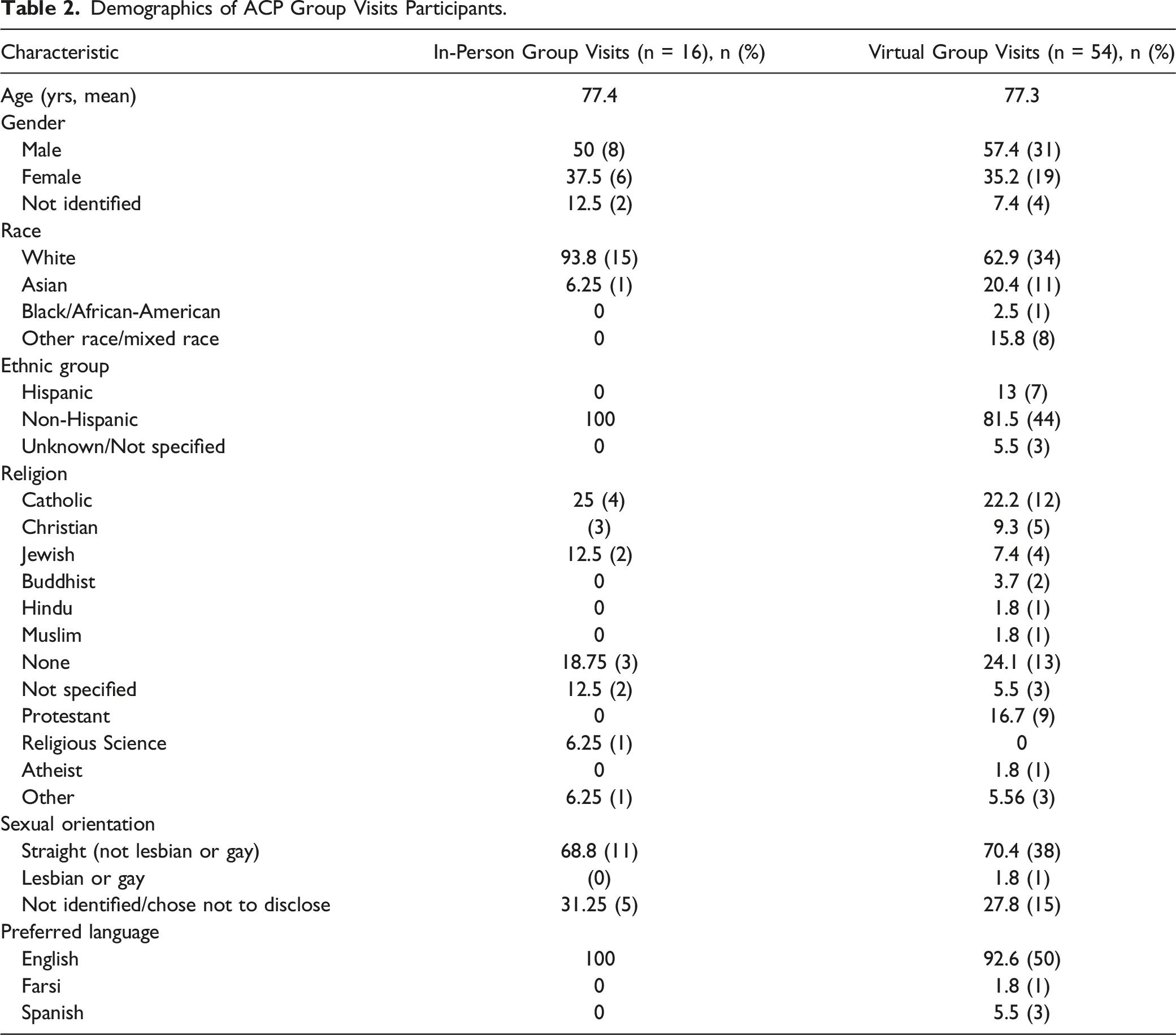
Of the 344 patients who were referred to ACP GVs in the EHR since its inception in December 2020, 17 participants attended. Thus, 1 assessment of reach, based on electronic referrals was 17 of 344 (4.9%). All other participants were recruited from study flyers given or seen by participants in the exam room.
While the goal for both visit types was 8 participants per session, actual group sizes ranged from 2-8 patients due to cancellations and no-shows. With the two-session visit format, the retention rate for the second session was 64% for in-person GVs and 48% for virtual GVs.
Effectiveness
Effectiveness of In-Person Group Visits vs Virtual Group Visits on ACP Outcomes.

Adoption
As a measure of adoption of virtual GVs for ACP, 5 of the 6 geriatricians in the clinic had a patient who participated in the virtual GVs. In addition, all of the Medical Assistants (2), LVNs (2), and RNs (1) demonstrated participation in referrals as evidenced by documentation in the EHR.
Implementation
As a measure of implementation, participants’ perspectives on acceptability of the in-person GV format vs the virtual GV are shown in Supplemental Figure 1. The post-session evaluation assessed the participants’ levels of agreement with 7 statements concerning the acceptability of the ACP GVs. Supplemental Figure 1 reflects the patient responses that indicated “5: Strongly Agree” to the evaluation prompts. (In-person GVs: n = 16; Virtual GVs: n = 54).
Participant Feedback Related to Virtual Group Visits.
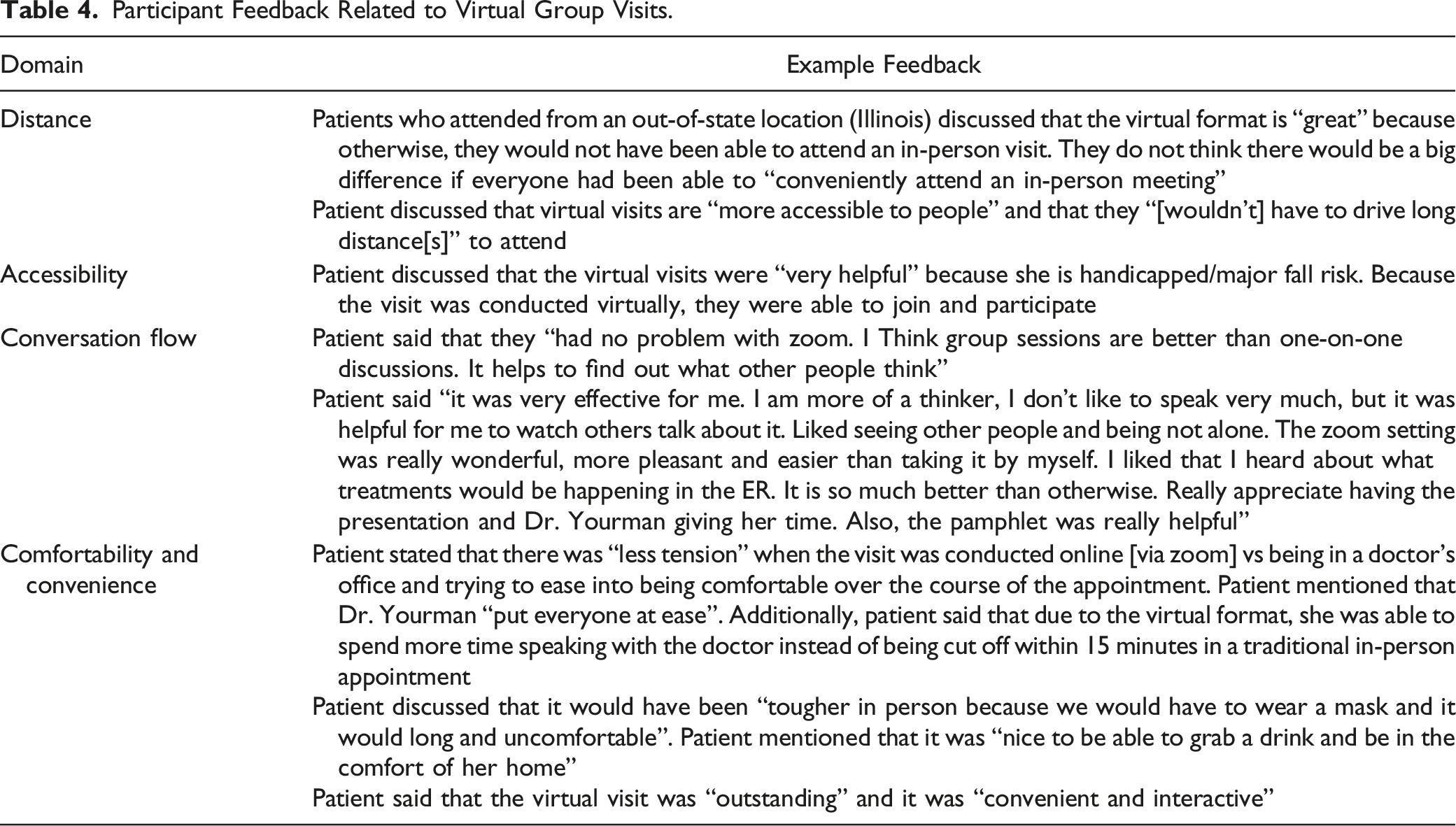
Using a telehealth platform also provided additional advantages of virtual technology (such as mute/unmute and start/stop video) allowing participants to determine the level of participation with which they were comfortable. Furthermore, features such as screen-sharing, text chat, and document sharing, allowed participants to send questions and interact with 1 another, group facilitators to present slides, and volunteers to address questions or concerns privately, send forms, links, or reference material via the chat feature throughout the session.
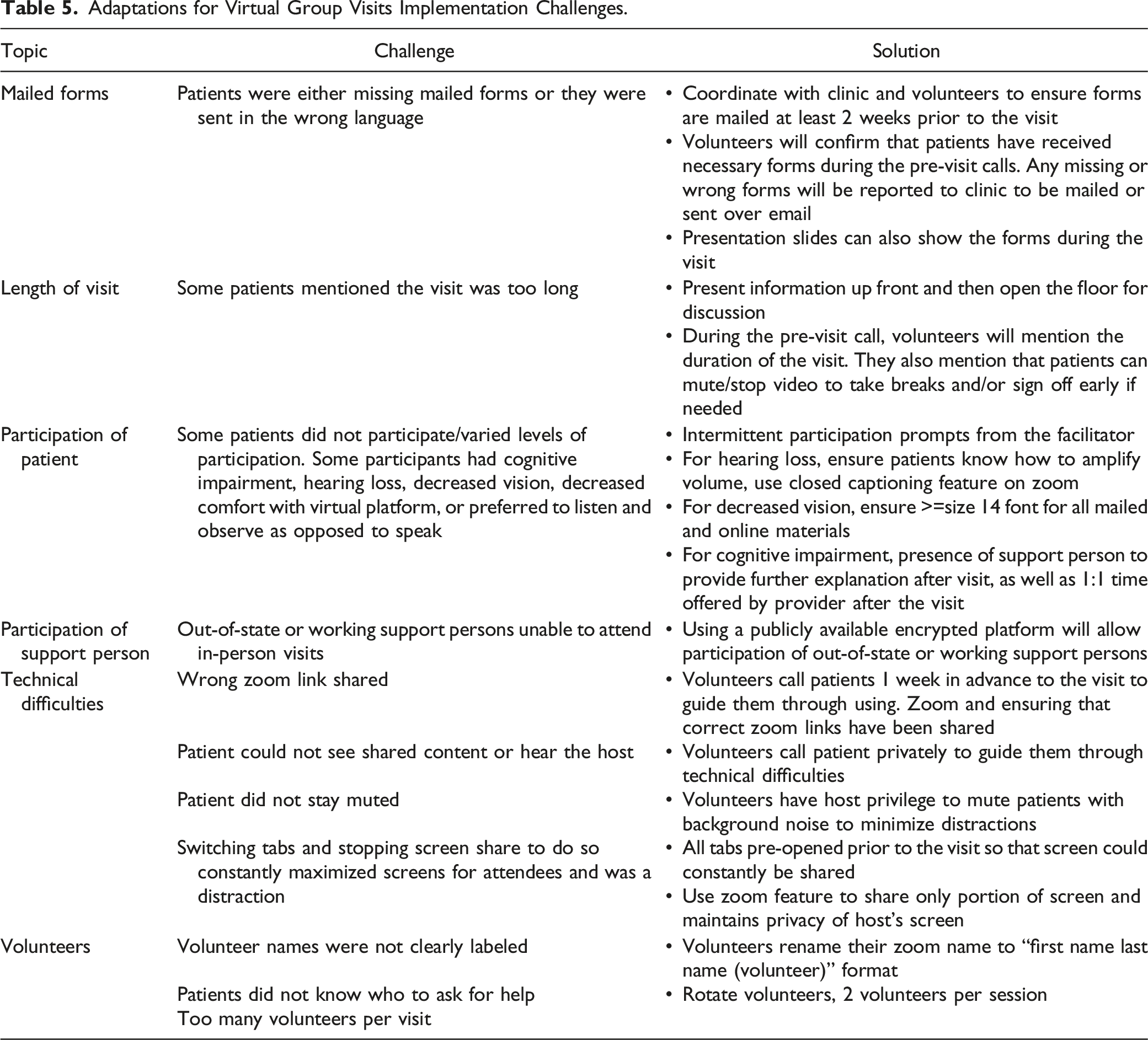
Adaptations for Virtual Group Visits Implementation Challenges.
Discussion
This study demonstrates feasibility, acceptability, and increased ACP outcomes through adapting an ACP GVs intervention to a virtual GVs format. The virtual GVs were effective at ACP engagement, increasing GOC conversations from 31% to 93% and completion of advance directives from 22% to 30% of virtual GVs participants. The prevailing participant feedback received indicated the acceptability of the virtual format over the in-person format.
Several considerations must be made to the implementation and sustainability of ACP virtual GVs. One consideration is that patients may have differential access to technology based on socioeconomic status and/or technological know-how. This study had a homogenous population that was predominantly older, white men, and the results may differ with a more diverse participant base. No data was collected on educational level, which could play a role in having these types of conversations. Another limitation is that virtual visits may not be ideal or possible for those with hearing or visual impairments, though in some cases the use of “closed captioning” features in virtual platforms can be helpful for older adults hearing impairment. Furthermore, a barrier may be the availability of volunteers or clinic team members needed for the logistical component of these virtual visits: mailing materials, outreach calls prior to group visits, post-visit calls, and telehealth technology troubleshooting. Finally, billing for GVs is not intuitive and represents a deviation from clinician protocols for individual patient visits, a potential barrier for clinician participation.
Reach and recruitment in ACP GVs were limited in our study, as demonstrated by the relatively lower 4.9% participation rate of referred patients relative to other studies on ACP GV. It is possible that the time commitment (2 2-hour sessions) may have been a deterrent for this particular ACP intervention, or that more broadly, engaging patients in ACP conversations remains challenging 16 and may relate to underlying fear and discomfort around serious illness discussions, lack of knowledge and awareness, and cultural and language barriers. However, challenges in engaging patients in ACP are not unique to GVs and there are many ways this challenge could be addressed in future studies, including by increasing clinician education and engagement around ACP, using patient testimonials, and other materials that are often used to attract patients and families to a behavioral intervention (e.g., food, posters, patient facing MyChart options, etc.). In addition, due to COVID-19 preclusion of in-person GV, relatively few patients participated in the in-person GV compared to virtual GV, thereby limiting any conclusions that can be drawn regarding differences between in-person vs virtual GV reach and recruitment.
An interesting follow up study, and thus limitation of ours, is looking at the comparison of ACP compliance with those who attended GV and those who did not. Because this study did not collect data from patients who did not attend ACP GV, we are unable to provide a comparison.
The study results have promising implications for the applicability of the virtual group format for other discussion-based health education beyond advanced care planning. The use of volunteers also demonstrates that expanding the definition of who comprises a healthcare team can alleviate much of the administrative burden and cost to make group visits a feasible way to deliver various health education topics. Other interdisciplinary team members can include administrative assistants, medical assistants, nurses, volunteers, social workers, and case managers.
In conclusion, virtual group visits for advance care planning were demonstrated in this study to be effective and feasible in our post-pandemic world. There is a plan in place to restart Group ACP once a new facilitator is found. In this coming time, further tests of change in the process of continuous quality improvement will be required in order to improve reach and effectiveness of Group ACP.
Supplemental Material
Supplemental Material - Feasibility and Effectiveness of Virtual Group Advance Care Planning Visits During the COVID-19 Pandemic
Supplemental Material for Feasibility and Effectiveness of Virtual Group Advance Care Planning Visits During the COVID-19 Pandemic by Lindsey Yourman, Alina Pollner , Jasmine Khatibi, Vanessa Ramos, Vaishnavi Melkote, Aoibhin O’Gorman
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dr. Lum is Supported in Part by the National Institute on Aging of the National Institutes of Health under Award Number R01AG066804. The Content is Solely the Responsibility of the Authors and does not Necessarily Represent the Official Views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.