
Abstract
Background
Disparities in advance care planning (ACP) among older Latinos necessitate targeted interventions to enhance engagement and knowledge in end-of-life care. This study aimed to evaluate the effectiveness of a resource-efficient, culturally tailored educational intervention in improving ACP readiness and knowledge among older Latino adults in the community.
Methods
A quasi-experimental pretest-posttest design was used to assess the impact of the intervention. The study involved community-dwelling older Latinos (aged 61-94) in the U.S. attending community wellness centers. Measures included participants’ knowledge of ACP, care options, familiarity with hospice and palliative care, and attitudes toward hospice, assessed using pre- and post-intervention surveys.
Results
Statistically significant improvements were observed in ACP knowledge, understanding of care options, and attitudes towards hospice and palliative care post-intervention. Demographic factors influenced knowledge scores, with no significant gender differences in the intervention’s efficacy.
Conclusions
The educational intervention effectively enhanced end-of-life care planning readiness and knowledge among older Latinos. The study highlights the potential for sustainable, accessible, and culturally sensitive educational strategies to reduce disparities in ACP knowledge and possibly engagement.
It is widely known that the U.S. older adult population is growing rapidly and projected to reach 83.7 million (20% of the population) by the year 2050. Racial and ethnic minorities represent one of the fastest growing groups within this population. Between 2008 and 2019, the racial and ethnic minority older adult population in the United States nearly doubled, reaching over 12 million. This population is expected to continue to grow at a significantly greater rate (125%) than non-Hispanic white Americans (32%). By 2040, the size of the racial and ethnic minority older adult population is projected to reach almost 28 million, representing 34% of all older adults. 1 Despite the growing numbers, older Latinos are underrepresented in hospice care, and as a group exhibit rates of advance care planning (ACP) completion that are lower than their non-Hispanic, white counterparts. 2 ACP refers to “the process of planning for future medical care in the event that the patient is unable to make his or her own decisions” and involves discussing goals of care and documenting preferences. 3
There is evidence that discussing, and documenting, end-of-life wishes can be beneficial for patients and their families. ACP is associated with enhancing patient autonomy and control, reducing family decisional burden, and improving experiences with care.4,5 Having an advance care plan in place has also been shown to reduce the number of unwanted and invasive interventions that patients undergo near end-of-life, thus reducing healthcare costs. 6 There are also benefits to engaging in end-of-life preparation before medical conditions require it. Declines in physical or cognitive capacities due to disease trajectories often hinder individuals’ ability to articulate their care preferences. The Institute of Medicine has noted that approximately 45%–70% of patients have impairments that affect their capacity to communicate and record their care choices. 7
There are two generally accepted categories that make up end-of-life care options: (1) life-sustaining treatments, and (2) palliative care. Life sustaining treatments focus on keeping the patient alive when vital bodily functions fail. The goal of care with life-sustaining treatments is curative, and treatments aim to maintain the patient alive for as long as possible. Life-sustaining treatments can include cardiopulmonary resuscitation (CPR), mechanical ventilation, artificial administration of nutrition, fluids, and medicines, and other medical treatments intended to treat the patient. 8 By contrast, palliative care focuses on improving the quality of life of patients and families faced with terminal illnesses. 9 The goal is palliative rather than curative, and care focuses on preventing or making suffering less severe and maximizing the quality of life. While palliative care focuses on symptom management and quality of life, it can be used alongside curative treatments (e.g., patient receiving chemotherapy and palliative care). Hospice care, however, is a specific type of palliative care focused solely on comfort care for individuals with terminal illnesses who are no longer pursuing life-prolonging treatments. The National Hospice and Palliative Care Organization 10 reports that, in 2020, more than half of all White Medicare decedents received hospice care, compared to only one third of Latino/Hispanic Medicare decedents.
Despite incentive to increase rates of ACP completion (e.g., insurance reimbursements), 2017 estimates from the Center of Disease Control and Prevention (CDC) suggest that as many as 70% of Americans do not have an advance care plan. 11 Several studies have attempted to explain the disparities that exist in end-of-life planning, since non-Hispanic whites are more likely than Black, Asian, and Hispanic/Latino patients to prepare for their end-of-life. Explanations salient in the literature pertain to socioeconomic factors, 12 attitudes toward the healthcare system,13–15 attitudes about death and dying,15–17 and cultural beliefs about autonomy vs independence.12,15 Though most of the studies examining these hypotheses use African American/Black samples, a growing number of them have focused on Asian and Hispanic/Latino patients. Studies with Hispanic/Latinos, specifically, find that this group is also significantly less likely than non-Hispanic whites to engage in formal end-of-life planning.18,19 Among older Latinos, preference for family-centered decision-making, low health literacy, language, and cultural barriers with providers are all challenges impacting ACP participation.20–23 For Spanish-speakers, poor communication among health care providers, patients, and surrogates, exacerbated by poor health literacy, contribute to poor ACP.3,4 Family members of Latino patients cite a lack of knowledge for their incongruence with patient preferences.2,3 Patients, for their part, indicate that their families know their wishes as the main reason for not having an ACP. 24 Furthermore, ACP discussions are often introduced late, following an emergency hospitalization or when death is imminent. 25
Various interventions have been tailored to engage Spanish-speaking populations in ACP. One of the forefront tools in this endeavor is the “PREPARE for Your Care” online platform, which has been made available in both English and Spanish, offering culturally relevant guidance for individuals navigating ACP. 26 Another key initiative is the “Respecting Choices®” model, an evidence-based approach that involves structured interviews and has been translated to meet the needs of Spanish-speaking communities. 3 “Five Wishes,” a comprehensive ACP document designed to navigate end-of-life considerations, has been made available in multiple languages, including Spanish. Additionally, using community health workers (CHW) to actively engage in ACP conversations has proven effective within Latino communities. CHWs have been successful in addressing cultural sensitivities and nuances by providing culturally competent communication and bridging gaps between healthcare professionals and patients. 27 These interventions, whether digital platforms, structured models, or community-based efforts using CHWs, all have made strides in making ACP more accessible for Spanish-speakers. Yet, most of these interventions lack the real-time, interactive component that is essential for individuals navigating complex end-of-life decisions. The self-guided or predetermined nature of these tools does not offer participants the flexibility to seek clarifications, ask spontaneous questions, or engage in dynamic conversations that evolve based on individual concerns and cultural nuances.
The few programs that engage Spanish-speakers directly are done within clinical settings, or through cost and resource-intensive initiatives, resulting in low uptake outside of clinical and research settings. 28 Furthermore, recent studies have indicated that after attending clinical ACP sessions, patients frequently have significant misunderstandings about life-prolonging treatments. 29 Thus, there remains a need for a community-based educational intervention that is not only culturally tailored and interactive but also crafted to require minimal resources, ensuring long-term sustainability and accessibility. The current study developed and tested a community education presentation, with the long-term goal of training adult-day center staff to integrate it within their programming.
Methods
This pilot study involved a quasi-experimental pretest-posttest design with Spanish-speaking older Latinos living independently in the community and engaged with community wellness centers. The intervention involved an educational presentation that covered topics such as ACP, end-of-life care options including curative and palliative models of care and sharing relevant resources. The survey measured participants’ knowledge of ACP, knowledge of care options, familiarity with hospice and palliative care, attitudes toward hospice, and perceived readiness for engaging in ACP.
Intervention
The intervention involved a PhD-level social worker delivering a didactic presentation, in Spanish, to Spanish-speaking older adults engaged in community wellness centers and whom had intact cognition. The social worker facilitator is a Spanish-speaking Latina with experience working with this population. Along with the presentation, participants were provided a pamphlet that contained information mirroring the items discussed in the presentation and containing a list of resources and a notes page. The contents of the presentation and pamphlet were developed based on existing literature describing effective intervention components and cultural considerations cited in community interventions tested with Spanish-speakers specifically. 30
Sample and Setting
Eligibility criteria included identifying as Hispanic/Latino, being 60 years of age or older, speaking Spanish as their primary language, and scoring a 13 or higher on the Brief Interview for Mental Status (BIMS) exam, indicating intact cognition. The BIMS is a screening tool used to measure attention, temporal orientation, and recall. It takes about 3 minutes to complete and was conducted along with the eligibility checklist, prior to enrolling the participant into the scheduled presentation. Participants were excluded from the study if they had already engaged in ACP documentation, or did not have decisional capacity (i.e., had a surrogate decision-maker or scored below 13 on the BIMS). The age of 60 was used as the minimum instead of the traditional 65, as it is believed that reaching a younger cohort of older adults may increase the likelihood that they are healthy or in early stages of disease progression, and thus be able to use the information to engage in ACP themselves.
Participants were recruited from community wellness centers (CWC) serving in predominantly Spanish-speaking communities across a metropolitan city in a southern U.S. state. CWCs in this context are multifaceted facilities that provide a blend of health services, social activities, and educational programs, often with a focus on holistic well-being. These centers often serve as communal spaces where older adults with similar cultural backgrounds congregate, making them suitable for this community-based intervention. Recruitment flyers were hand delivered to the contact person within each CWC. The CWC then posted flyers and made announcements to their participants about the opportunity. The PI also visited the CWCs and provided a brief overview of the study and answered questions. Interested participants were screened using an eligibility checklist (including the BIMS) and enrolled into the study if eligible. Enrolled participants were then given details about the scheduled presentation, which would take place at a later day at the CWC.
Study Measures
Demographics
Participant’s age, gender, religion, country of origin, time in the United States, and highest level of education were recorded during the pre-intervention survey.
Advance Care Planning Knowledge
The six true/false statements (shown in Appendix 1) tested knowledge of ACP. A summary score was generated by converting the variables to either correct or incorrect and then generating a sum score for each participant, where a 6 indicated perfect knowledge. This measure was used in prior research, where reliability was reported to be low 31 (<.60), consistent with our study findings (<.50).
Knowledge of Care Options (KOCO)
KOCO is a validated scale measuring knowledge of curative, palliative, and hospice care. It contains 11 true/false items (shown in Appendix 2) and a point is awarded for each correct response, with 11 indicating a perfect score. In addition to exploring each item individually, a summary score was generated, by converting the variables to either correct or incorrect and then generating a sum score for each participant on the total number of correct responses. The reliability of this measure was reported to be .89 in a prior study 32 but was low in our Spanish-translated version (Cronbach’s α < .60).
Hospice and Palliative Care Familiarity
Two sets of questions asked participants to indicate whether they had heard the terms hospice or palliative care (yes/no). Then, they were asked to rate their familiarity with hospice and palliative care using a 3-point scale (1 = not very familiar, 2 = somewhat familiar, 3 = very familiar). This measure has been used in prior research. 33 An additional question asked participants to indicate whether they understand the differences between palliative care and hospice care (y/n).
Importance of End-of-Life Issues
To evaluate participants’ priorities for end-of-life care, participants rated the importance of eight issues (shown in Appendix 3) using a 3-point scale (0 = not at all important, 1 = somewhat important, 2 = very important). A summary score of the importance of EOL concerns was generated (max 16). This measure has been used in prior research, but reliability was not reported.34,35 Our Spanish-translated version produced a Cronbach’s alpha of .60.
Hospice Intention and Opinion
Participants’ intention to use hospice was measured using a single dichotomous question, asking “If you were dying, would you want the support of hospice services?” (y/n). An additional question asked participants to rate their opinion of hospice using a 3-point scale (0 = not at all favorable, 1 = somewhat favorable, 2 = very favorable).
Analysis
Univariate analyses were conducted to provide an overview of sample characteristics. Frequencies and percentages are reported for each categorical variable. Means and standard deviation are reported for respondent age and self-rated perceived preparation to engage in ACP. Chi-square tests were conducted to test associations between pre and post categorical outcomes. Paired t-tests were conducted for continuous variables. Data were analyzed using STATA 18.0. The study was approved by the University of Central Florida Institutional Review Board (IRB approval #STUDY00002961).
Results
Sample Characteristics
Sample Demographics (n = 47).
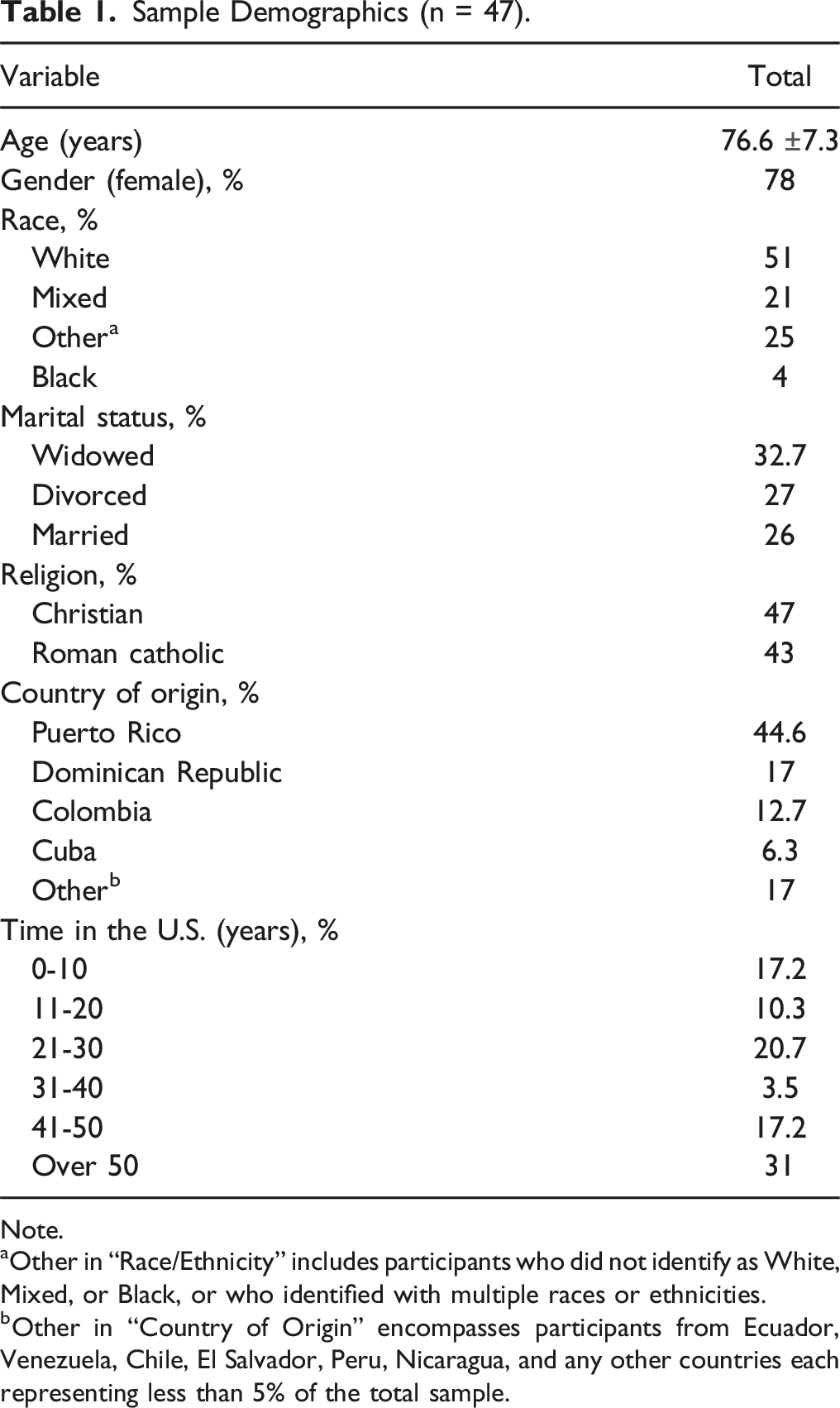
Note.
aOther in “Race/Ethnicity” includes participants who did not identify as White, Mixed, or Black, or who identified with multiple races or ethnicities.
bOther in “Country of Origin” encompasses participants from Ecuador, Venezuela, Chile, El Salvador, Peru, Nicaragua, and any other countries each representing less than 5% of the total sample.
The primary aim of the study explored the effectiveness of the intervention in improving ACP knowledge among community-dwelling older adults. Secondary aims included changes in knowledge of care options, the importance assigned to end-of-life issues, and knowledge and intentions regarding hospice and palliative care.
Advance Care Planning Knowledge and Knowledge of Care Options
Paired Samples t test Results.
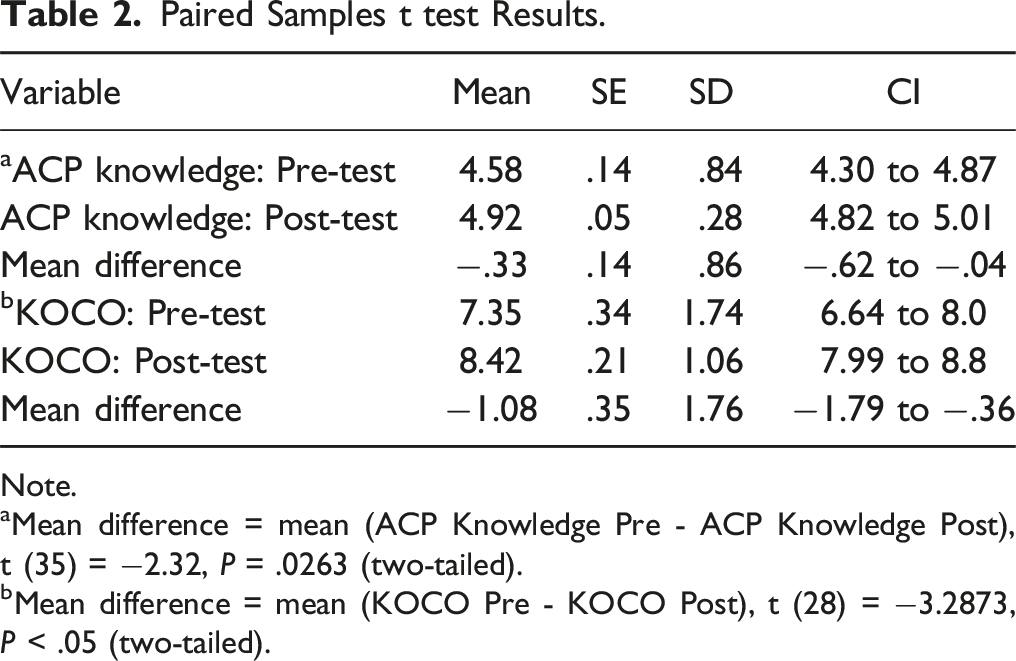
Note.
aMean difference = mean (ACP Knowledge Pre - ACP Knowledge Post), t (35) = −2.32, P = .0263 (two-tailed).
bMean difference = mean (KOCO Pre - KOCO Post), t (28) = −3.2873, P < .05 (two-tailed).
Importance of End-of-Life Issues
The mean score for the importance of EOL issues pre-intervention was 13.38, indicating a generally high level of importance attributed to these issues by the participants from the start. Post-intervention, this score increased to 15.49. The paired t test revealed that this increase was statistically significant (P < .001), suggesting a meaningful enhancement in the perceived importance of EOL concerns following the intervention.
Hospice Knowledge and Intentions
Impact of Intervention on Importance of EOL Issues and Hospice Use Intentions.

In summary, the intervention had a positive impact on participants’ knowledge, opinions, and interest in hospice and palliative care. Certain demographic factors like age, marital status, and education level were significantly associated with knowledge scores. No significant gender differences were observed in the pre- and post-tests across the variables (except for knowledge of palliative care above), indicating that the intervention was similarly effective for both genders.
Discussion
The present study evaluated the effectiveness of an educational intervention designed to enhance knowledge and attitudes concerning advance care planning (ACP), hospice and palliative care, and other end-of-life care options among community-dwelling older adults. Our findings confirm the study’s primary and secondary aims, revealing statistically significant improvements across multiple domains. This aligns with existing research affirming the efficacy of targeted educational interventions in improving older Spanish-speakers’ knowledge of and attitudes toward ACP and hospice care.36,37
The observed increase in ACP knowledge post-intervention substantiates the role of educational interventions in fostering ACP among older adults. 26 Likewise, participants demonstrated significant improvements in their knowledge of care options. The statistical significance of these findings underscores their practical importance and adds empirical weight to existing literature.36,38 This finding highlights the interplay between cultural and knowledge-based factors in shaping ACP preferences among Latinos. Traditionally, academic literature has emphasized cultural norms and family dynamics as primary determinants of ACP engagement in Latino communities.39,40 Our study shows, however, that enhancing knowledge through educational interventions can significantly influence attitudes and preferences related to end-of-life care. This suggests that the lower rates of ACP completion among Latinos might not solely be a result of cultural reticence but could also stem from a lack of accessible information and understanding. Therefore, addressing informational gaps may be as crucial as respecting cultural nuances in promoting ACP among Latino older adults.
The lack of gender differences in the intervention’s efficacy contrasts with the general trend of gender-related disparities in health literacy. 41 This uniform effectiveness across genders in our study may suggest that well-designed educational interventions can overcome traditional barriers and reach diverse audiences effectively, or that other factors account for the previously observed differences. The associations observed between demographic variables like age, marital status, and education level with knowledge scores offer valuable insights for future interventions. For example, the findings that older participants had better knowledge scores highlights the potential need for age-specific or life stage-specific educational approaches. Younger cohorts of older adults may require more foundational information on ACP and its relevance at an early age. It also highlights the importance of age-appropriate delivery methods to bridge knowledge gaps. Virtual and interactive formats may be more effective for younger cohorts of older adults, whereas in-person community programs such as this one might better engage older cohorts. These findings underscore the necessity of tailoring ACP educational materials to specific demographic characteristics to enhance their effectiveness.
The high importance participants ascribed to end-of-life issues resonates with the cultural shift towards more proactive engagement in these matters, as noted by Steinhauser et al. 42 This is an important shift, considering the historical reluctance in discussing end-of-life care among many cultures, including Latinos. Furthermore, the intervention’s success in not only increasing awareness but also in positively shifting opinions towards hospice and palliative care is particularly noteworthy. Beyond offering the intervention in Spanish, we employed culturally sensitive communication strategies informed by prior research, acknowledged family values and religious beliefs that are prevalent among Hispanic cultures, and discussed how ACP aligns with these values (e.g., reducing burden and family disputes). That, coupled with the ethnic concordance of the facilitator, set the intervention apart and adds to its potential to be delivered on an ongoing basis by trained community wellness center staff, as a resource-efficient strategy. This finding aligns with prior studies reporting that positive attitudes towards hospice and palliative care are predictive of future utilization of these services, as we found positive opinions to be associated with intention to use hospice.43,44 Our study adds to this body of literature by demonstrating that targeted educational interventions can effectively modify perceptions and potentially influence care decisions among older adults, including simple, cost-effective interventions implemented within community settings. 45
While our study demonstrates the positive impact of educational interventions on knowledge of ACP and opinions of end-of-life care options, it is important to note that prior research has shown education alone does not translate to actual ACP engagement. 46 Barriers to ACP engagement extend beyond knowledge gaps and include communication with providers and healthcare coverage, for example. 46 Therefore, effective ACP engagement strategies often require a multi-pronged approach that encompasses not only education but also various advocacy efforts for patients and families. These could include facilitating discussions about ACP within families, developing easy-to-use digital tools to document goals at the time of the family discussion, and training community providers to guide ACP conversations and documentation effectively, outside of clinical settings.
Limitations
Methodological limitations, including the sample size and use of measures not validated with older Spanish-speakers, demand cautious interpretation of the results. The sample size of 47 participants limited our ability to conduct several analyses and might not effectively detect smaller effect sizes. A key socioeconomic status variable, income, was initially included but had to be dropped due to significant missing data. This omission is notable considering that income has previously been associated with lower engagement in ACP. Lastly, the measures used were not always validated with Spanish-speakers and had to be translated by the research team, contributing to the observed low Cronbach’s alpha scores. Future research is needed to focus on validation and refinement of these measures for use with Spanish-speaking populations.
Future research should also focus on the long-term sustainability of the intervention’s impact. It is essential to understand whether the increased knowledge and positive attitudes towards ACP observed in the study persist over time and lead to actual completion of ACP documents. Furthermore, exploring how factors such as ethnicity and religious beliefs might influence ACP outcomes could provide a more nuanced understanding of ACP engagement in diverse populations. While this study contributes valuable insights into enhancing ACP engagement among older Spanish-speaking adults, the limitations outlined here highlight the need for further, more comprehensive research to validate and expand upon these findings.
Conclusion
In summary, this study’s educational intervention has demonstrated promising improvements in end-of-life care planning readiness and knowledge among community-dwelling older Latinos. The intervention’s design, emphasizing minimal resource requirements, highlights its potential for long-term sustainability and accessibility in community settings. These findings add a robust empirical layer to the existing literature, advocating for tailored, resource-efficient educational strategies in end-of-life care planning. An important next step is to prepare community wellness center staff for delivering this training, examining the acceptability and feasibility of this approach. This phase is crucial to determine whether such staff can effectively implement the intervention in a way that is both impactful and practical.
The success of the intervention in increasing understanding and positively shifting attitudes towards ACP, hospice, and palliative care among older Latino adults underscores the value of well-designed, culturally sensitive, and cost-effective educational approaches. By equipping community wellness center staff with the necessary tools and knowledge, we aim to extend the reach of this intervention, making it more accessible to a broader audience. This approach aligns with our commitment to developing educational interventions that are not only culturally resonant but also sustainable and accessible, especially in resource-constrained environments. These initiatives are anticipated to not only empower older adults to make informed decisions about their end-of-life care, thereby enhancing their autonomy and quality of life in their final years, but also to reduce the observed disparities in engagement with advance care planning and mitigate the negative outcomes frequently observed among underrepresented groups, particularly in the context of end-of-life care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Learning Institute for Elders at University of Central Florida, Inc.