
Abstract
Keywords
Introduction
Amyotrophic lateral sclerosis (ALS) is an incurable neurodegenerative disease of the upper and lower motor neurons, resulting in progressive voluntary muscle weakness and eventual paralysis.1,2 It is a multisystem disease with symptoms that can include respiratory dysfunction, communication and swallowing difficulties, cognitive and behavioral changes, and numerous psychosocial challenges.1,3
The heterogeneity in presentation and natural progression of symptoms in ALS introduce considerable risk of unmet biopsychosocial needs.2,4,5 A small but growing body of research on the experiences of people living with ALS (pALS) highlights many opportunities to strengthen clinical services. Increased ALS education, enhanced biopsychosocial support, access to resources to preserve independence, caregiving support, facilitation of goals of care conversations, and proactive palliative education and involvement in end-of-life care are among the most commonly cited recommendations.2,6,7
Palliative Care for pALS
Palliative care focuses on relieving the symptoms and stress of serious illness, aiming to optimize patients’ quality of life. 8 In addition, for patients experiencing life-threatening illnesses such as ALS, it can play an important role in supporting planning for future healthcare needs. 9 Although there is an emerging consensus that palliative services often enhance ALS care,5,10-12 if, when, and how palliative care should be provided to pALS remains unclear.2,3,5 For example, recent research has shown support for the feasibility and utility of a model in which referrals to palliative specialists are universal within a multidisciplinary ALS clinic, 12 but the cost-effectiveness and acceptability of this model have yet to be determined. 11
Although previous qualitative research has identified potential benefits of palliative care services for pALS, 2 quantitative examination of the needs those services are intended to address has been limited to date. A comprehensive understanding of the variable needs and experiences of pALS is imperative to guide the integration of palliative and ALS care and to inform future research investigating palliative care’s impact on both clinical and patient-centered outcomes among pALS. To address this gap in the knowledge base, our interdisciplinary team of researchers and clinicians conducted a national survey to measure unmet palliative care needs among pALS and to examine relationships among those needs. We aimed to extend current understandings of the needs of pALS by examining understudied topics (eg, emotional and physical intimacy) and incorporating consideration of illness progression. Further, we sought to build on existing qualitative research2,3 by investigating relationships among pALS’ needs and relevant clinical and patient-centered outcomes, including advance care planning behaviors and quality of life.
Methods
Three team members (KTW, SM, AKM) developed our survey instrument. Informed by a biopsychosocial model of illness, 13 a review of the relevant scientific literature, and clinical expertise in providing neuropalliative care, we first developed a list of key constructs we sought to measure. We then identified validated instruments (including subscales and individual items) to measure those constructs, introducing modifications and researcher-generated items as needed, particularly when brevity was desired to minimize respondent burden. 14 Members of the Northeast Amyotrophic Lateral Sclerosis (NEALS) 15 Palliative Committee (primarily clinicians and researchers) and I AM ALS 16 (primarily pALS and their family members and friends) reviewed and provided feedback on survey drafts and assisted with respondent recruitment by disseminating study information and the Qualtrics (Provo, UT) electronic survey link via email and social media. Survey data were collected from November 2022 to July 2023. The Washington University in St. Louis Institutional Review Board reviewed and approved all research activities (#202205064). All respondents provided informed consent before completing the survey instrument.
Our final survey instrument asked respondents to provide basic demographic information (10 items) in addition to data obtained via the following measures: 1. ALS Specific Quality of Life-Revised (ALSSQOL-R): Overall Quality of Life (1 item), Emotional Intimacy (2 items), and Physical Intimacy (2 items): We asked respondents to rate their overall quality of life, taking into consideration multiple dimensions, such as their physical, social, emotional, spiritual, and financial quality of life. Response options ranged from 0 (very bad) to 10 (excellent). We also asked respondents to indicate their level of agreement (0 = strongly disagree to 10 = strongly agree) with statements indicating that, over the past week, they had a strong desire for [emotional or physical] intimacy or had shared [emotional or physical] intimacy with others. 2. Needs Assessment Tool: Progressive Disease (NAT: PD; 7 items):
17
We modified individual NAT: PD items to allow respondents to indicate the extent to which they were concerned about 7 wellbeing indicators (eg, unresolved physical symptoms, problems completing activities of daily living, financial challenges) using a scale of 0 (not at all concerned) to 10 (very concerned). 3. Measuring What Matters “Heard and Understood” Measure (1 item):18,19 We modified this single-item, self-report measure to ask respondents to indicate their level of agreement (0 = strongly disagree to 10 = strongly agree) with the following statement: “I feel heard and understood by my doctors, nurses, and other members of my healthcare team.” 4. Advance Care Planning (ACP) Behaviors Researcher-Generated Items (3): We asked respondents to indicate (yes/no) whether they had talked with family members or friends about their wishes for end-of-life care, talked with healthcare provider(s) about their wishes for end-of-life care, or formally documented their wishes for end-of-life care in writing. 5. Illness Progression Researcher-Generated Items (2): Because we did not individually assess respondents or have access to their medical records, we developed 2 items to allow us to estimate respondents’ disease progression according to the King’s staging system,
20
inquiring as to each respondent’s use over the prior week of a feeding tube and/or a device to help with breathing.
Data Analysis
We began our analysis by examining descriptive statistics for the sample and our measured variables, including means, standard deviations, medians, and ranges for continuous variables and frequencies for categorical variables. Responses to researcher-generated items assessing respondents’ illness progression were used to categorize respondents as having either early or advanced ALS. Respondents who indicated they had neither used a feeding tube nor a respiratory device during the prior week were considered to have early-stage ALS. Those who used a feeding tube and/or non-invasive or invasive ventilation were considered to have advanced-stage ALS.
To determine relationships among variables, we employed logistic and linear regression techniques. For our modeling procedure, we used a block-wise approach. The first model in our process was a bivariate regression, which included our proposed explanatory variables (feeling heard and understood by one’s healthcare team, stage of illness progression) and outcome variables (ACP behaviors, quality of life). In the second model, we added demographic covariates (age, gender, and highest level of formal education; race and ethnicity were initially included but ultimately dropped, given our sample’s racially and ethnically homogenous nature). We examined estimates and significance values for individual variables and the model’s overall fit to the data. We also calculated odds ratios (OR) and their 95% confidence intervals (CI) for our logistic models. We considered P values <.05 as statistical evidence of an association between predictors of interest and outcomes. We also performed model diagnostics using scatterplots for residuals and fitted values, normal q-q plots, and variance inflation factors. Missing data were handled using list-wise deletion.
Results
Sample Characteristics (N = 112).
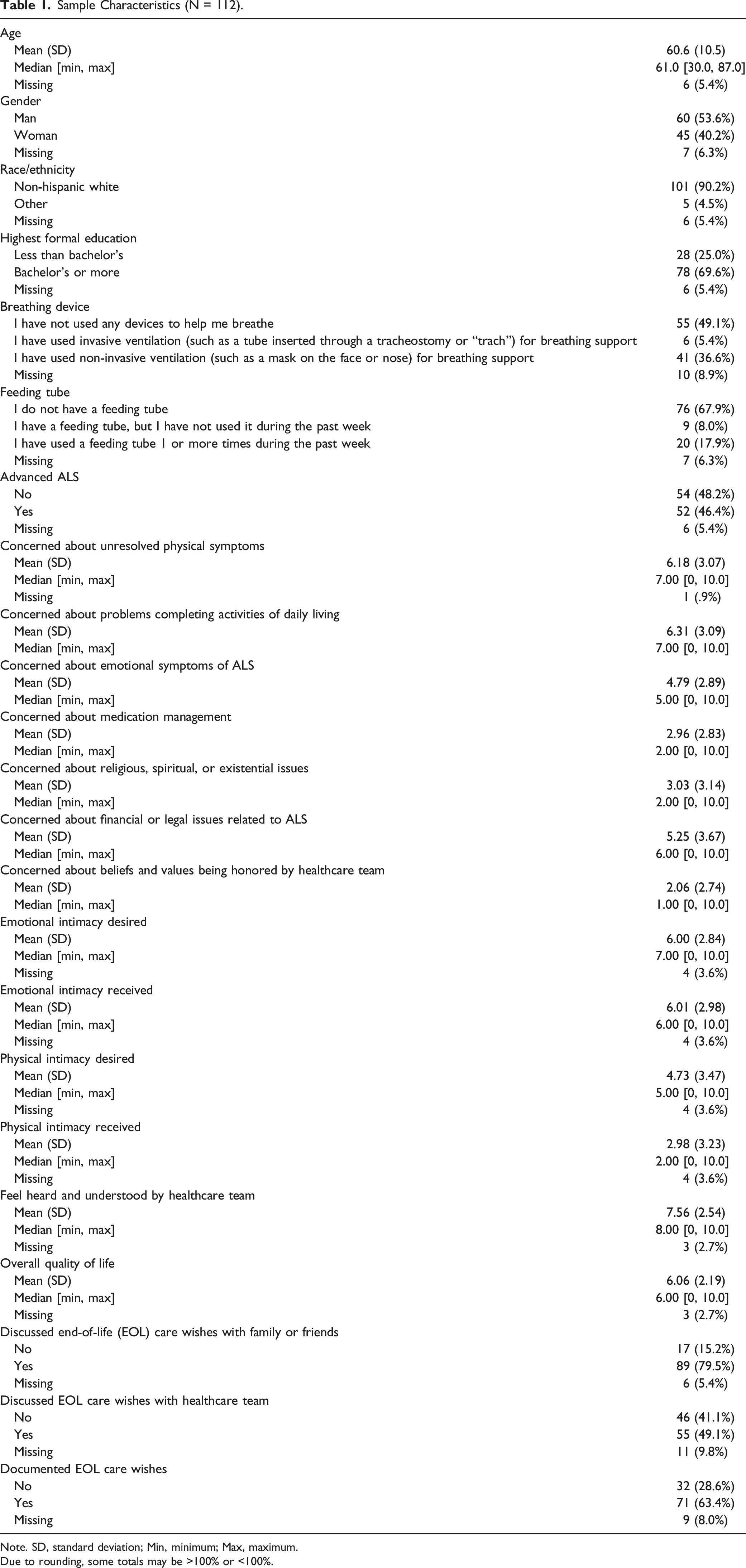
Note. SD, standard deviation; Min, minimum; Max, maximum.
Due to rounding, some totals may be >100% or <100%.
Logistic Regression Results for Illness Progression and Advance Care Planning Behaviors.
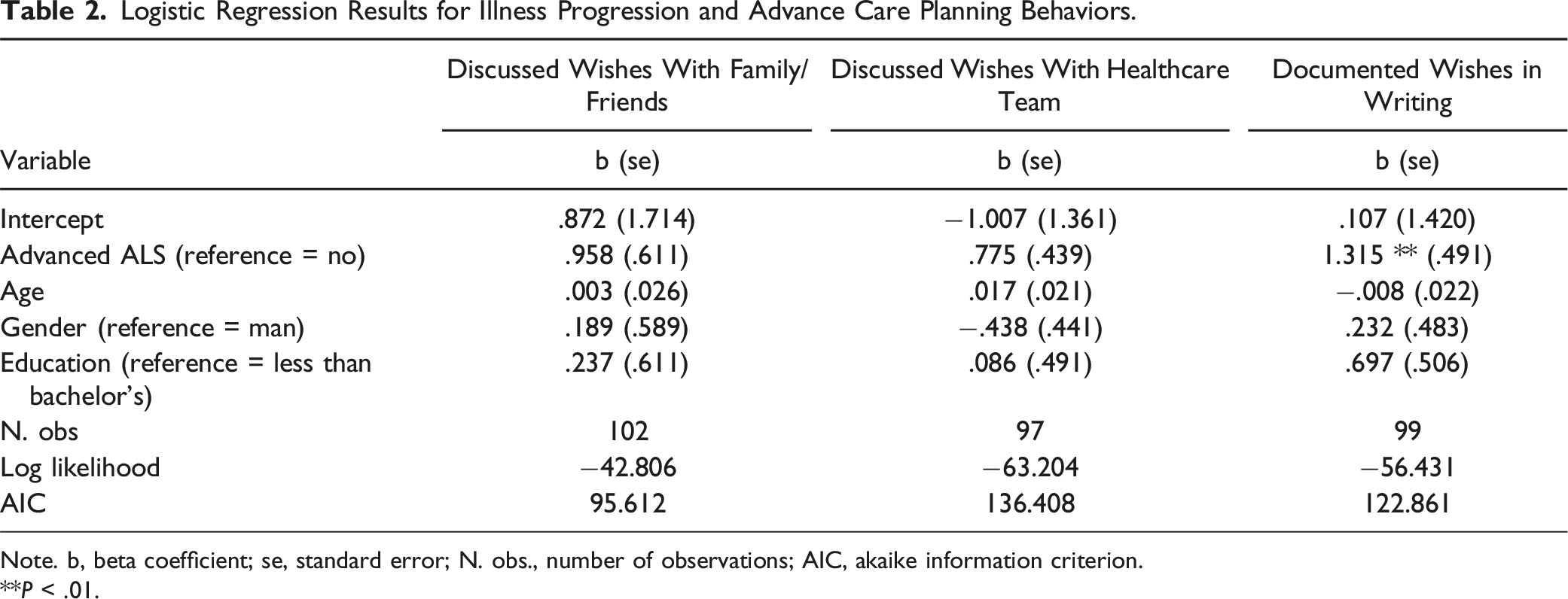
Note. b, beta coefficient; se, standard error; N. obs., number of observations; AIC, akaike information criterion.
**P < .01.
Odds Ratios and Confidence Intervals for Illness Progression and Advance Care Planning Behaviors.
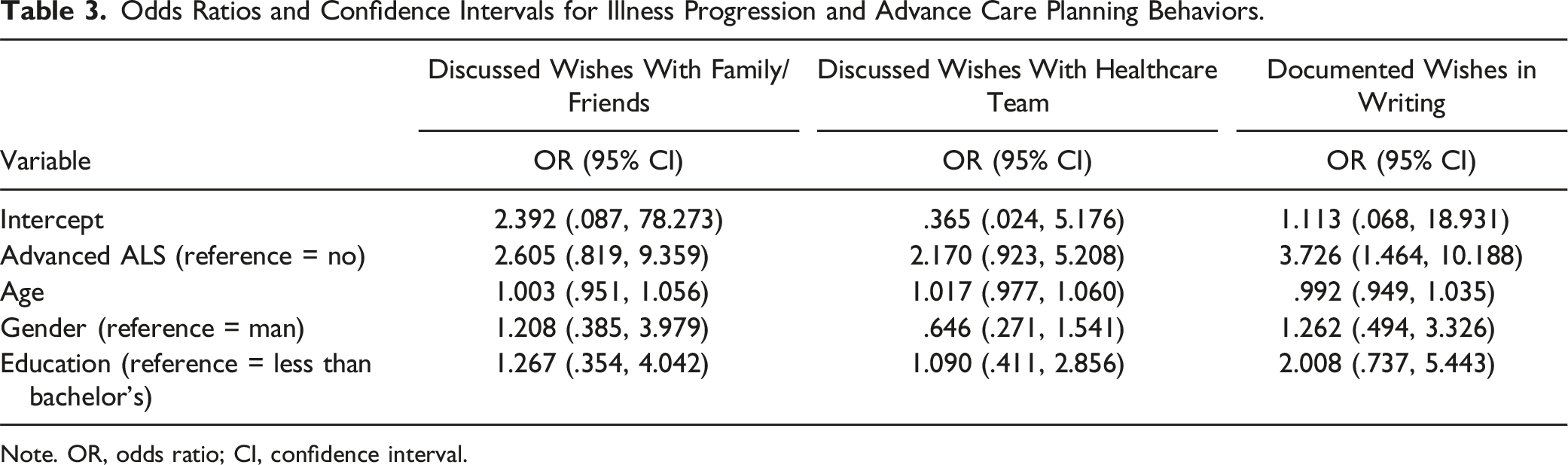
Note. OR, odds ratio; CI, confidence interval.
Logistic Regression Results for Feeling Heard and Understood by Healthcare Team and Advance Care Planning Behaviors.
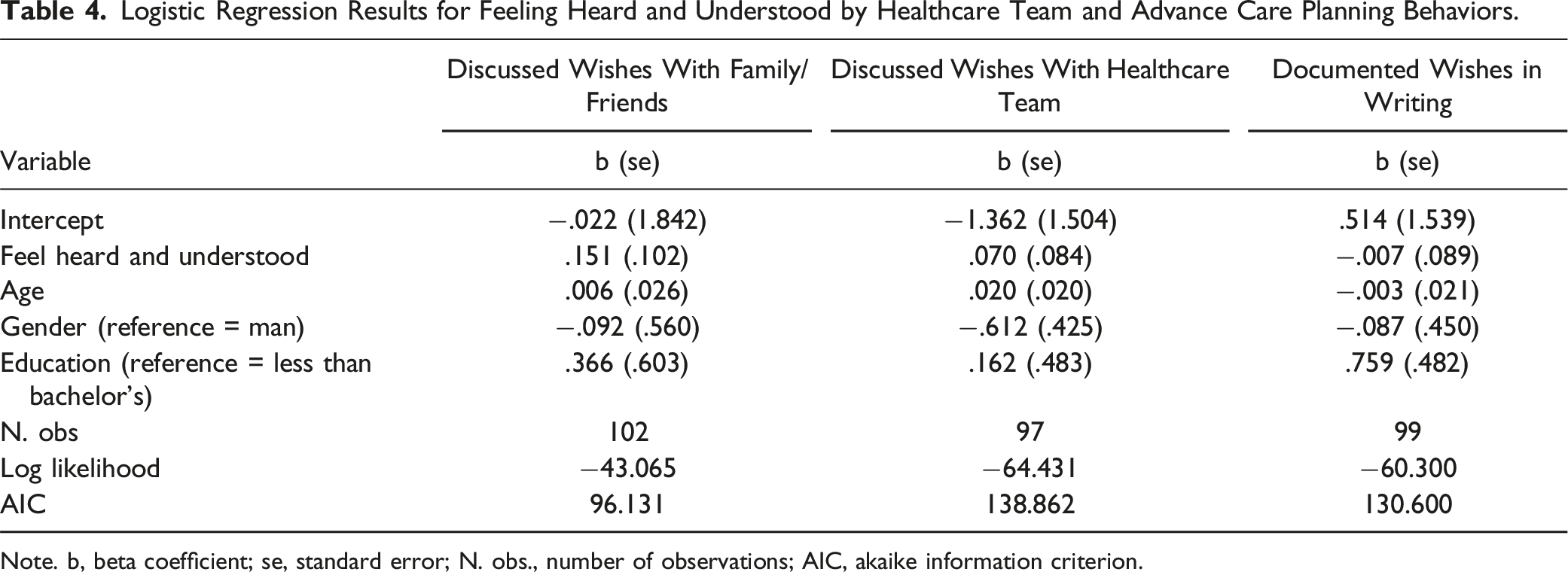
Note. b, beta coefficient; se, standard error; N. obs., number of observations; AIC, akaike information criterion.
Odds Ratios and Confidence Intervals for Feeling Heard and Understood by Healthcare Team and Advance Care Planning Behaviors.
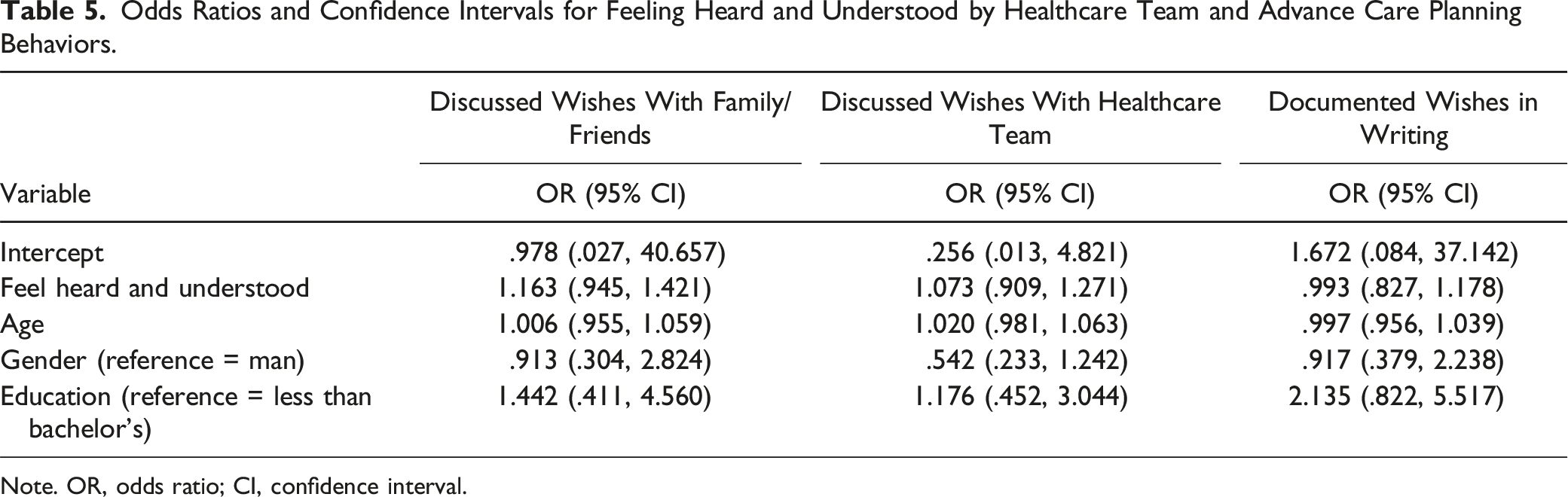
Note. OR, odds ratio; CI, confidence interval.
Linear Regression Results for Quality of Life Models.
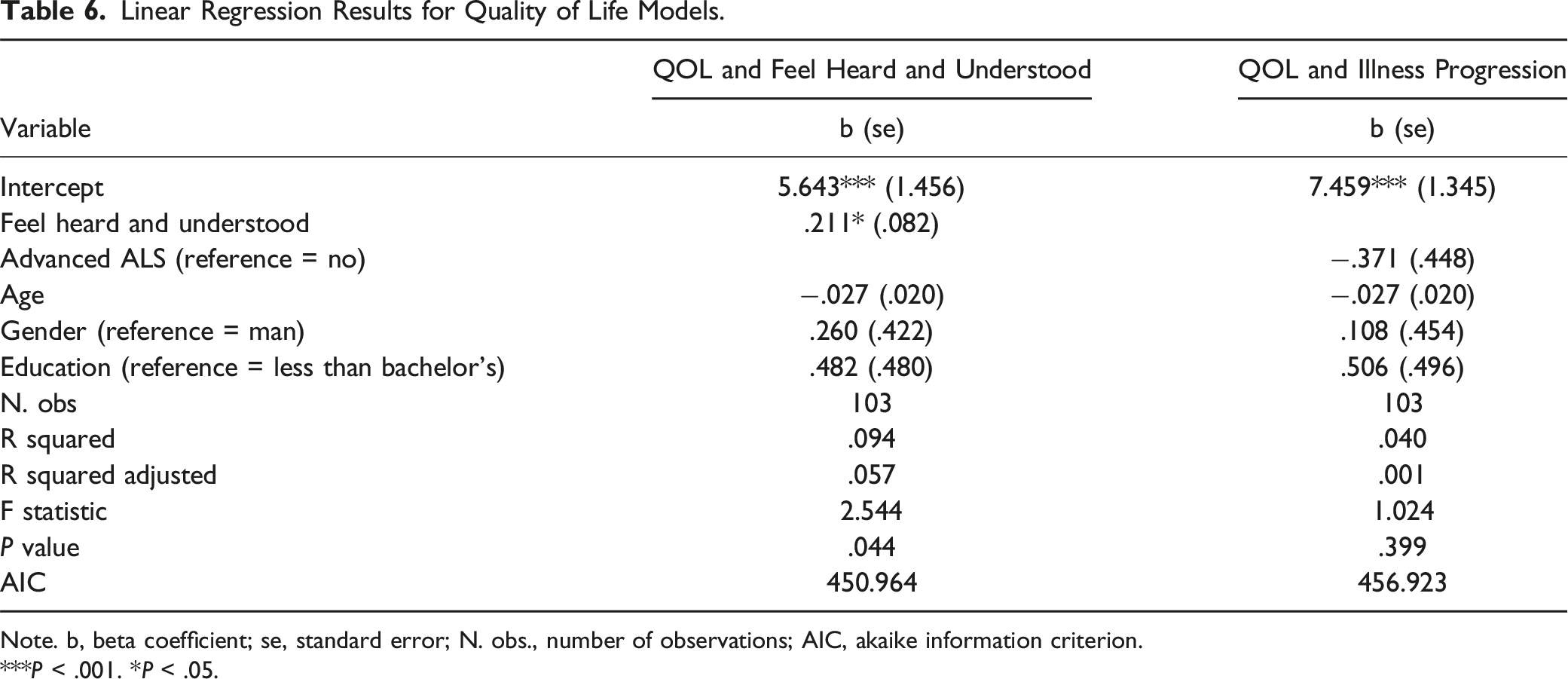
Note. b, beta coefficient; se, standard error; N. obs., number of observations; AIC, akaike information criterion.
***P < .001. *P < .05.
Discussion
Survey results suggest numerous opportunities for palliative care involvement in ALS care. Respondents expressed high (ie, >5 out of 10) levels of concern regarding problems completing activities of daily living, unresolved physical symptoms, and financial and legal issues related to ALS, all of which fall within the purview of palliative care. 21 Importantly, in addition to highlighting potential roles for palliative care more broadly, these findings emphasize the need for robust, interdisciplinary teams of palliative care physicians and advanced practice providers, nurses, social workers, and others who can support pALS in addressing the full range of issues they experience.
In the interpersonal realm, respondents’ mean scores for emotional intimacy received and desired were nearly identical, while, on average, respondents reported wanting more physical intimacy than they received. There were also gender differences with regard to physical desire, with men, on average, having greater desire for physical intimacy than women. These findings strengthen recent calls for increased attention to intimacy-related concerns in palliative care 22 and suggest that, should palliative clinicians heed these calls, they would be well positioned to improve the lives of pALS, who may require specialized interventions to support physical intimacy amid often pronounced functional limitations. 23
Finally, while advance care planning behaviors were higher in this sample than in the general population, 24 a significant minority of pALS reported having neither documented their wishes for end-of-life care in writing nor having discussed their wishes for end-of-life care with others. This was an unexpected finding, given the often rapid progression and universally fatal nature of ALS; it warrants additional attention in future studies. Relatedly, recent research indicating that the facilitation of advance care planning is a leading reason for palliative care referrals among pALS 9 highlights yet another potential benefit of palliative care’s integration into ALS care.
Study Limitations and Strengths
Several limitations should be considered when interpreting these findings. First, we note that our survey was cross-sectional in design, which precluded the identification of potential changes in pALS’ needs over time. Second, we estimated ALS staging from self-reported respondent data. Although our estimation criteria were developed in collaboration with a board-certified neurologist and clinical neurophysiologist (SM), which bolsters our confidence in their appropriateness, we lack access to the medical data that would be needed to make a conclusive determination regarding their accuracy. Third, respondents were self-selected, overwhelmingly non-Hispanic white, and disproportionately college-educated relative to the general U.S. population, 25 limiting the generalizability of the survey’s results (however, respondents’ race and ethnicity may, in part, reflect the baseline prevalence of ALS among non-Hispanic white individuals in the U.S. 26 ). Finally, we intentionally minimized respondent burden when creating our survey instrument and, as a result, did not obtain data capturing the full context and nuances of respondents’ experiences and perspectives. Additional research is needed to address these important considerations.
Notwithstanding these limitations, this study provides important knowledge. It informs the rich and very much ongoing discussion in the field concerning questions such as: Should palliative care be integrated into ALS care? If so, when? For whom? How? 11 It underscores the need for robust, interdisciplinary support for pALS and identifies, quantifies, and examines relationships among specific needs in the biopsychosocial realm. Finally, it suggests reasonable clinical and patient-centered outcomes for palliative care in ALS care, equipping future researchers and clinicians with valuable tools to evaluate the benefit (and, if indicated, the cost benefit) of this potentially beneficial yet unarguably limited healthcare resource. 11
Footnotes
Acknowledgments
The authors gratefully acknowledge I AM ALS and the Northeast Amyotrophic Lateral Sclerosis (NEALS) Consortium. Members of both organizations provided input into the study design, particularly with regard to survey development and respondent recruitment. In addition, the authors acknowledge and extend appreciation to the individuals with ALS who volunteered as survey respondents.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.