
Abstract
Background
Treatment at high-volume facilities (HVF) has been associated with improved prognosis of HNC patients undergoing curative treatment. Whether this systemic factor influences survival outcomes of patients with HNC undergoing palliative treatment is unknown.
Aim
To investigate the impact of palliative treatment facility volume on overall survival (OS) in patients with head and neck cancer (HNC).
Design
The 2004 to 2018 National Cancer Database was queried retrospectively for patients with HNC undergoing palliative treatment.
Setting/participants
Patients were stratified based on treatment facility volume percentile. Multivariable binary logistic and Cox proportional hazards regression models were implemented.
Results
Of 8682 patients included, 1661 (19.1%) underwent palliative therapy at facilities with volume ≥80th percentile. Among 972 facilities included, 643 (66.2%), 182 (18.7%), 85 (8.8%), 44 (4.5%), and 18 (1.9%) had volume <20th, 20-40th, 40-60th, 60-80th, and ≥80th percentiles, respectively. 5-year OS rates of patients undergoing palliative therapy at facilities with volume <20th, 20-40th, 40-60th, 60-80th, and ≥80th percentile was 11%, 13%, 11%, 14%, and 23%, respectively (P < .001). Facility volume ≥80th percentile was associated with higher 5-year OS on multivariable Cox regression (aHR 0.34, 95% CI 0.16-0.69, P < .001). Surgical treatment (aOR 1.34, 95% CI 1.07-1.68, P = .012) was associated with undergoing treatment at facilities with volume ≥80th percentile.
Conclusions
Undergoing palliative treatment at HVFs is associated with higher OS in HNC. The survival benefit derived from high facility volume should be carefully considered in the context of other patient and facility characteristics in end-of-life management, with specific emphasis on patient-directed goals of care.
Keywords
Introduction
Head and neck cancer (HNC) has a global incidence of approximately 890,000 cases per year, and is typically treated with surgery, radiotherapy, and/or chemotherapy. 1 The prognosis of HNC depends on tumor site, stage, and etiology, with an overall 5-year survival rate ranging from 40% to 65%. 2 However, an estimated 15%-20% of patients with HNC are not amenable to treatment with curative intent, and may benefit from palliative treatment, which focuses on providing symptom relief, comfort, and support to patients and their families. 3 Studies across various cancer types have demonstrated that palliative treatment improves quality of life, depression, satisfaction with care, and survival for patients, and offers education on end-of-life caregiving, respite care, and psychological counseling for caregivers.4-12
HNC imposes significant functional challenges through the disruption of essential functions including eating, breathing, and speaking, potentially rendering patients psychologically and socially distressed.13-19 Palliative treatment modalities in HNC, including medical management, surgery, chemotherapy, radiation, and combination therapy, are intended to provide airway protection, nutrition,20-23 tumor debulking, delay complications, and improve the overall end-of-life experience, and may also extend life in some cases.24-26
Modifiable systemic factors such as treatment facility type and volume also impact patient survival in HNC. Several studies have demonstrated improved prognosis of HNC patients who undergo curative treatment at high-volume facilities (HVF), hinting that multidisciplinary teams with an array of specialists may help better manage the intricacies of HNC.27-31 However, there is a lack of research assessing whether facility volume is a prognostic factor of HNC patients undergoing palliative treatment. Our study of the National Cancer Database (NCDB) investigates facility volume in palliative treatment management of HNC and associated differences in overall survival (OS).
Materials and Methods
Data Source
The NCDB is a national database jointly sponsored by the Commission on Cancer (CoC) of the American College of Surgeons and the American Cancer Society (ACS) that accounts for >70% of newly diagnosed cancer cases in the United States.32-36 The NCDB has established criteria to ensure that submitted data meets specified quality benchmarks. The Rutgers New Jersey Medical School and University of Pennsylvania Institutional Review Boards exempted our study because of the de-identified nature of patient data. The ACS and CoC have not verified and are not responsible for the validity of data analysis or conclusions derived herein.
Inclusion Criteria
Our study sample was comprised of adults undergoing palliative treatment for histologically confirmed head and neck cancer (HNC) between 2004-2018 (Figure 1). The NCDB was queried for cases of HNC using International Classification of Diseases for Oncology, Third Edition (ICD-O-3) histology (conventional squamous cell carcinoma was defined as “8070-8072”), behavior (invasive: “3”), and topography (oral cavity: C00.0 [lip], C02.0-3 [anterior, overlapping, NOS tongue], C03 [gingiva], C04 [floor of mouth], C050, C05.8-9 [hard, overlapping, NOS palate], C06 [other, NOS mouth; major salivary glands: C07 [parotid gland], C08 [others, NOS]; sinonasal tract: C11 [nasopharynx], C30.0 [nasal cavity], C31 [accessory sinuses]; oropharynx: C01 [base of tongue], C02.4 [lingual tonsil], C05.1-05.2 [soft palate, uvula], C09 [tonsil],C10 [oropharynx]; hypopharynx: C12 [pyriform sinus], C13 [hypopharynx]; larynx: C32.0 [glottis], C32.1 [supraglottis], C32.2 [subglottis], C32.3, 32.8-9 [other, overlapping, NOS]) codes. Patients were included if they were determined by the NCDB to have undergone palliative treatment, defined as any care intended to “control symptoms, to alleviate pain, or to make the patient more comfortable.”
37
Patients were excluded if they underwent palliative treatment at >1 reporting facility or a facility other than the reporting facility. Patients undergoing treatment with curative intent, and those with unknown vital status or survival time were excluded from analysis. Patients referred to palliative treatment but not documented to undergo palliative treatment were also excluded. Inclusion criteria. Abbreviations. NCDB, National Cancer Database.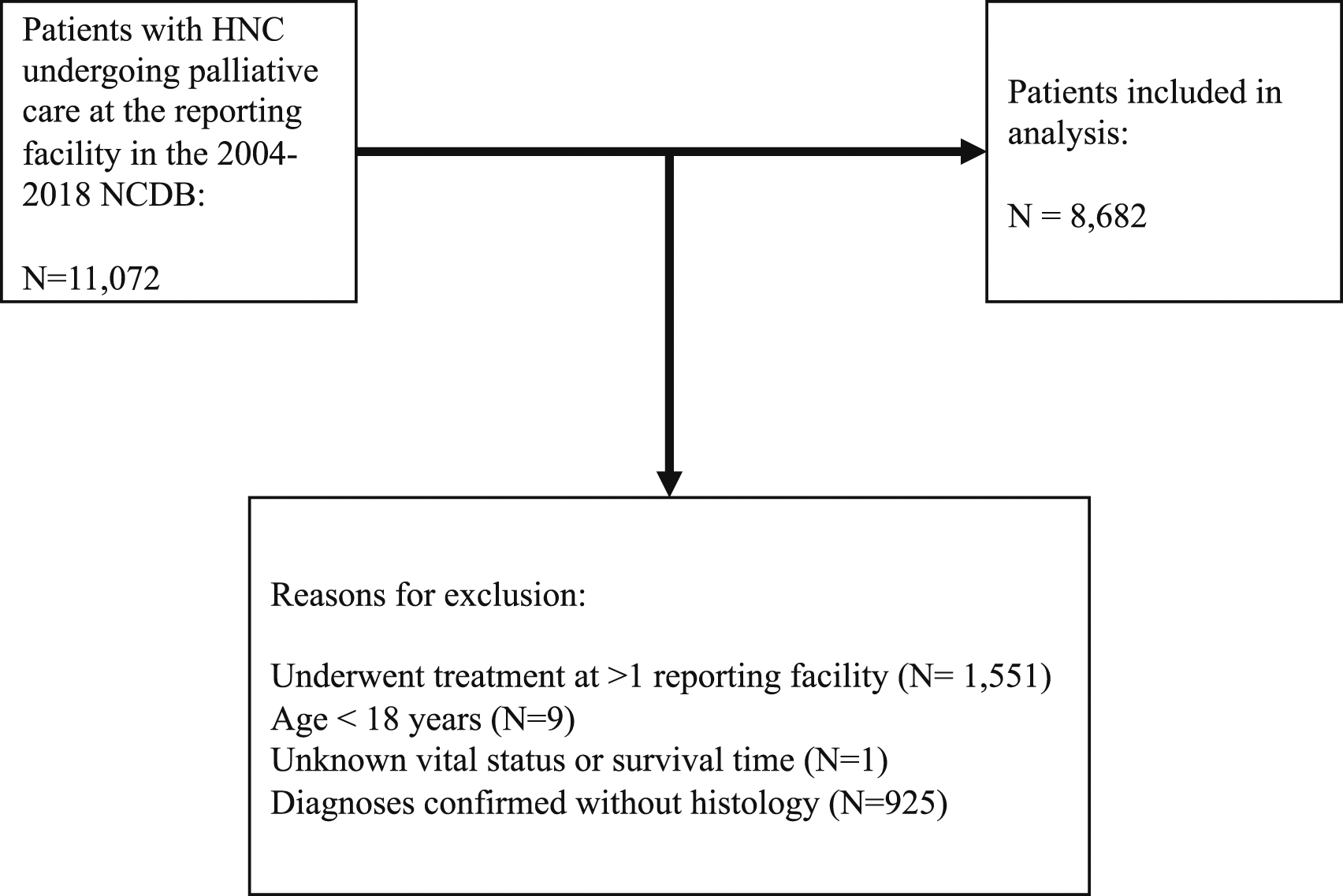
Variables
The following categorical variables were collected for each patient cohort: sex (male, female), race (White, Black, other), primary payer status (no insurance, private insurance, Medicaid, Medicare), median household income of residence zip code (<$40,227, $40,227-50,353, $50,354-63,332, ≥$63,333), population density (metro, urban/rural), facility type (academic/research, non-academic/research), facility location (New England, Middle and South Atlantic, Central, Mountain/Pacific), Charlson-Deyo comorbidity score (CDCS) (0, ≥1), history of prior malignancy, histology (conventional squamous cell carcinoma, other), primary site (oral cavity, major salivary glands, sinonasal tract, oropharynx, hypopharynx, larynx), HPV status (HPV negative, HPV positive, unknown), grade (low, high, unknown), clinical tumor-nodal-metastasis (cTNM) classification, pathologic extranodal extension (pENE), lymphovascular invasion (LVI), and palliative treatment (surgery alone, radiotherapy alone, chemotherapy alone, pain management alone, combination therapy, other). We also reported the following continuous variables: age at diagnosis, palliative treatment facility volume, distance (mi) to surgical facility, and survival time. Median household income was determined by the median household income in a patient’s zip code based on the 2012 American Community Survey data. Population density was categorized as metropolitan (>250,000 individuals) or urban/rural (0-249,999 individuals). A CDCS of 0 indicates no comorbid diseases. An academic/research facility is defined by the NCDB as an institution that records >500 newly diagnosed cancer cases each year, participates in postgraduate medical education and cancer-related research, and offers the full range of diagnostic and treatment services on-site. Non-academic facilities pools together community (records >100 but <500 newly diagnosed cancer cases per year), comprehensive community (records >500 newly diagnosed cancer cases per year), and integrated network (no minimum caseload but owns, operates, leases, or is part of a joint venture offering comprehensive services) facilities.
The NCDB utilizes the following designations for palliative treatment: (1) “surgery (which may involve a bypass procedure) to alleviate symptoms, but no attempt to diagnose, stage, or treat the primary tumor is made;” (2) “radiation therapy to alleviate symptoms, but no attempt to diagnose, stage, or treat the primary tumor is made;” (3) “chemotherapy, hormone therapy, or other systemic drugs to alleviate symptoms, but no attempt to diagnose, stage, or treat the primary tumor is made;” (4) “patient received or was referred for pain management therapy with no other palliative care;” (5) any combination of surgery, radiation therapy, chemotherapy, and pain management therapy; and (6) “palliative care was performed or referred, but no information on the type of procedure is available in the patient record” or palliative treatment was provided but does not fit the aforementioned descriptions. Patients were stratified into 5 cohorts based on the volume percentile of the facility at which they underwent palliative treatment: <20th, 20-40th, 40-60th, 60-80th, and ≥80th. The primary outcome of our study was 5-year OS. Survival time was calculated as the time from diagnosis to either death or 5 years of follow-up.
Statistical Analysis
Chi-square and Kruskal–Wallis H tests were used to compare categorical and continuous variables, respectively, by facility volume percentile. Multivariable binary logistic regression was performed to identify patient demographics, facility characteristics, cTNM classification, and treatment independently associated with undergoing palliative treatment at a facility with volume ≥80th percentile. The Hosmer-Lemeshow test was used to assess the calibration of the logistic regression model. 5-years OS was estimated using the Kaplan-Meier method and compared across cohorts using the log-rank test. A multivariable Cox proportional hazards regression adjusting for all significant variables in univariable Cox regression was used to identify factors independently associated with OS. 3 sensitivity analyses were performed: (1) facility volume was binarized at varying percentile thresholds, (2) 2-year and 3-year OS were utilized as primary outcomes to account for censorship and follow-up loss, and (3) sequential landmark survival analysis was performed for patients surviving
Results
Patient Factors and Palliative Treatment Modalities
Patient Demographics and Clinicopathologic Features by Facility Volume Percentile.
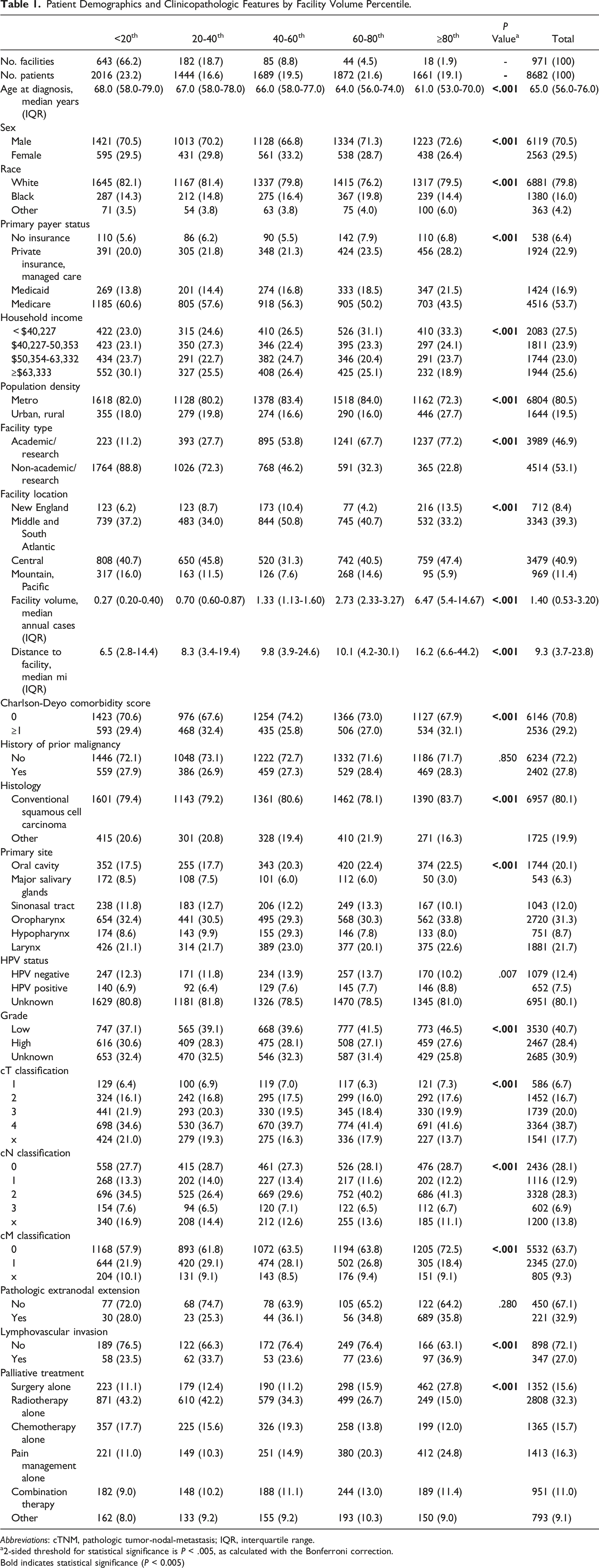
Abbreviations: cTNM, pathologic tumor-nodal-metastasis; IQR, interquartile range.
a2-sided threshold for statistical significance is P < .005, as calculated with the Bonferroni correction.
Bold indicates statistical significance (P < 0.005)

Trends in palliative treatment modalities between 2004 and 2018.
Univariable and Multivariable Binary Logistic Regression Models Identifying Factors Associated With Undergoing Palliative Treatment at a Facility With Volume
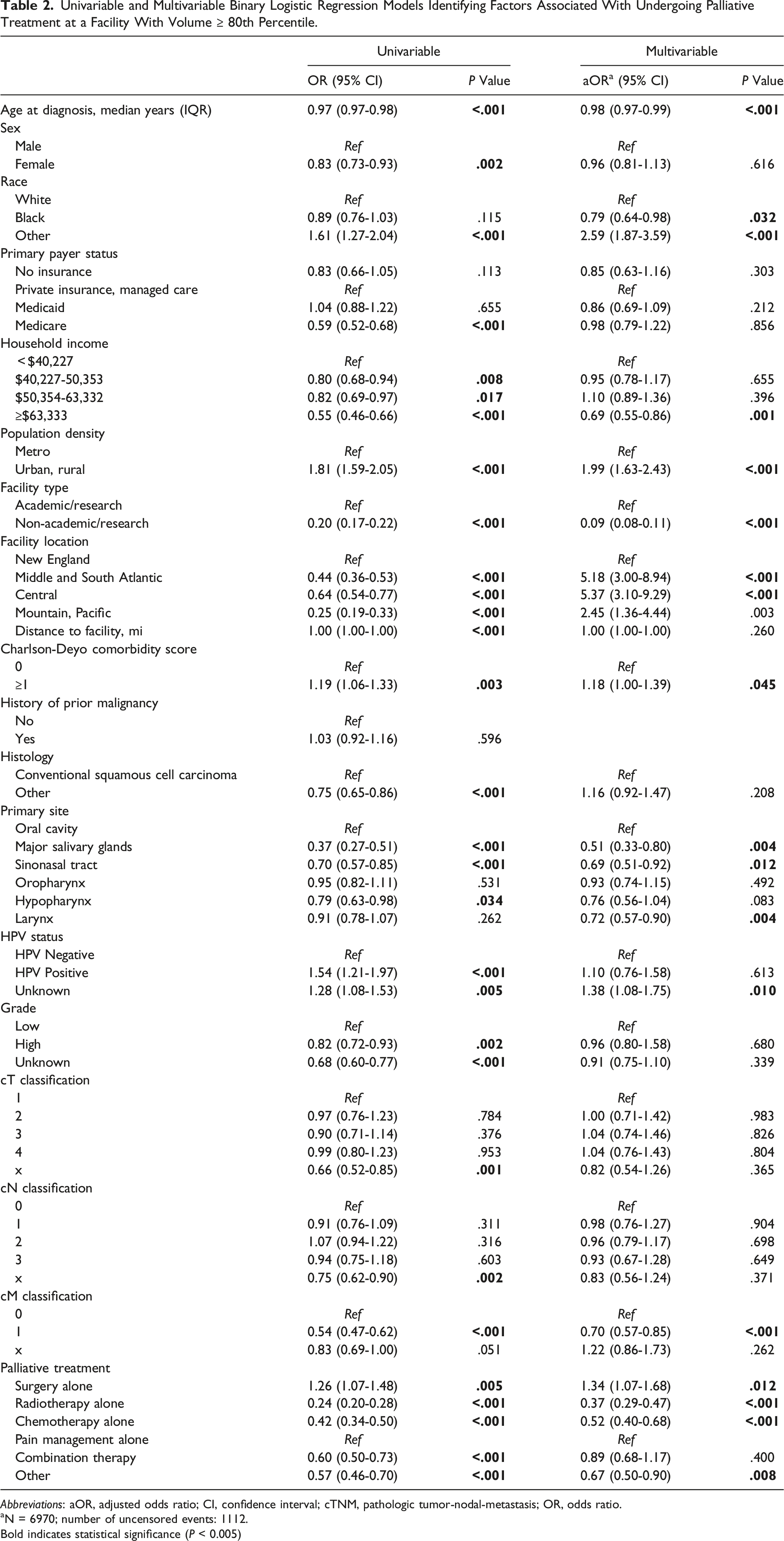
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; cTNM, pathologic tumor-nodal-metastasis; OR, odds ratio.
aN = 6970; number of uncensored events: 1112.
Bold indicates statistical significance (P < 0.005)
5-Year OS by Facility Volume and Prognostic Factors
Kaplan-Meier Analysis of 5-Year OS Rate (%) by Facility Volume Percentile.
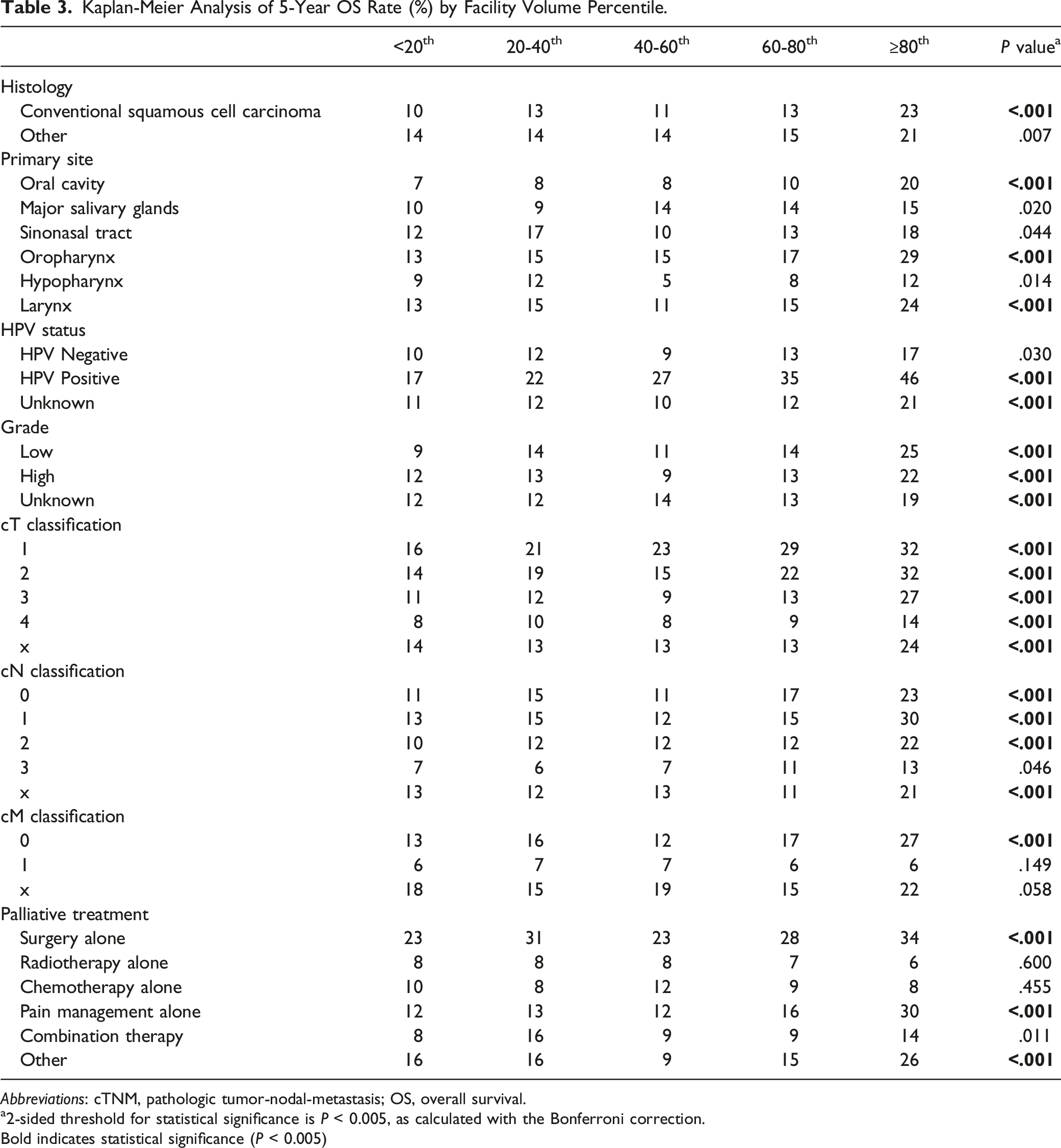
Abbreviations: cTNM, pathologic tumor-nodal-metastasis; OS, overall survival.
a2-sided threshold for statistical significance is P < 0.005, as calculated with the Bonferroni correction.
Bold indicates statistical significance (P < 0.005)
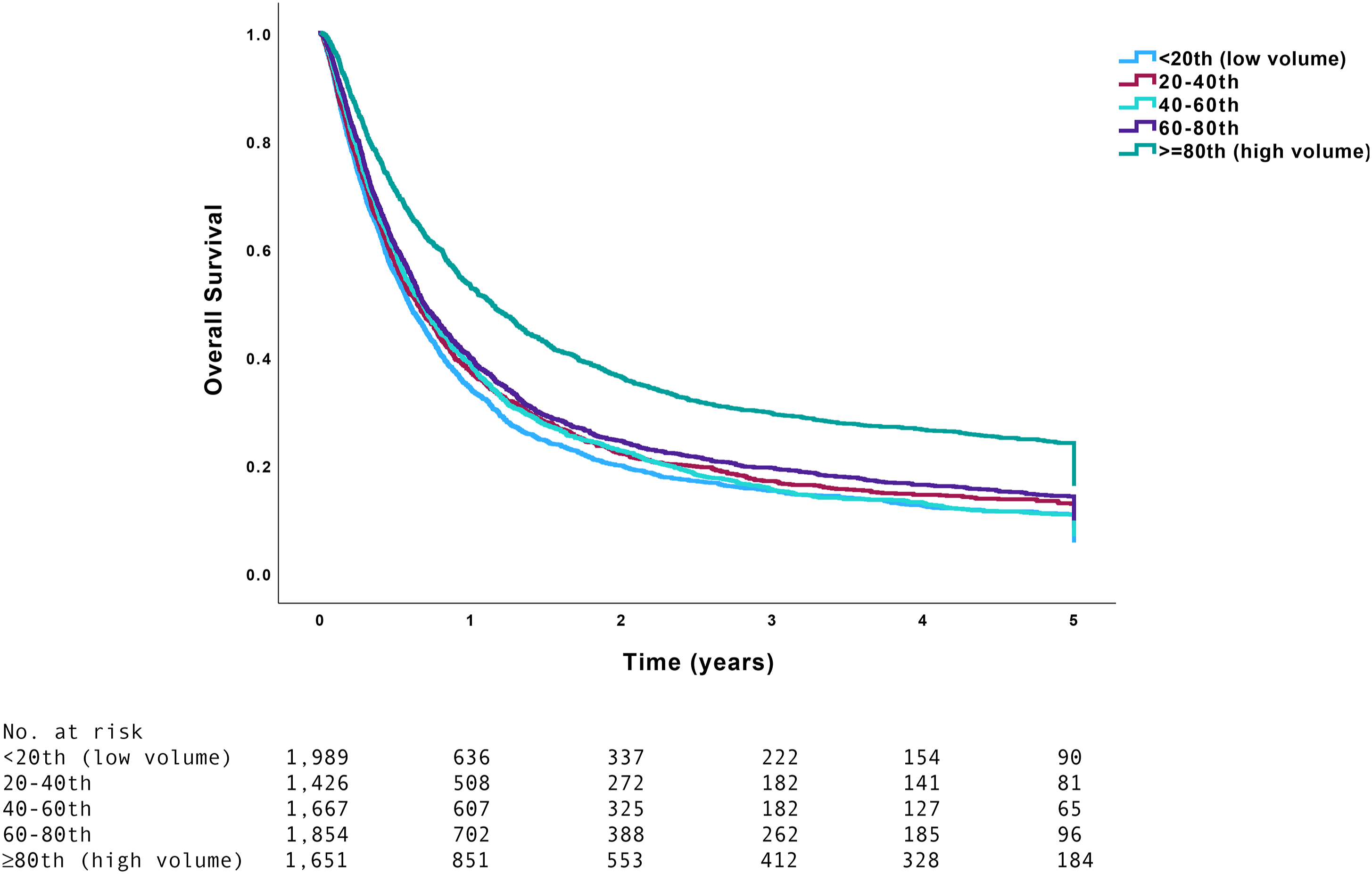
5-year overall survival by facility volume percentile. Significance derived from the log-rank test.
Univariable and Multivariable Cox Proportional Hazard Regression Models.
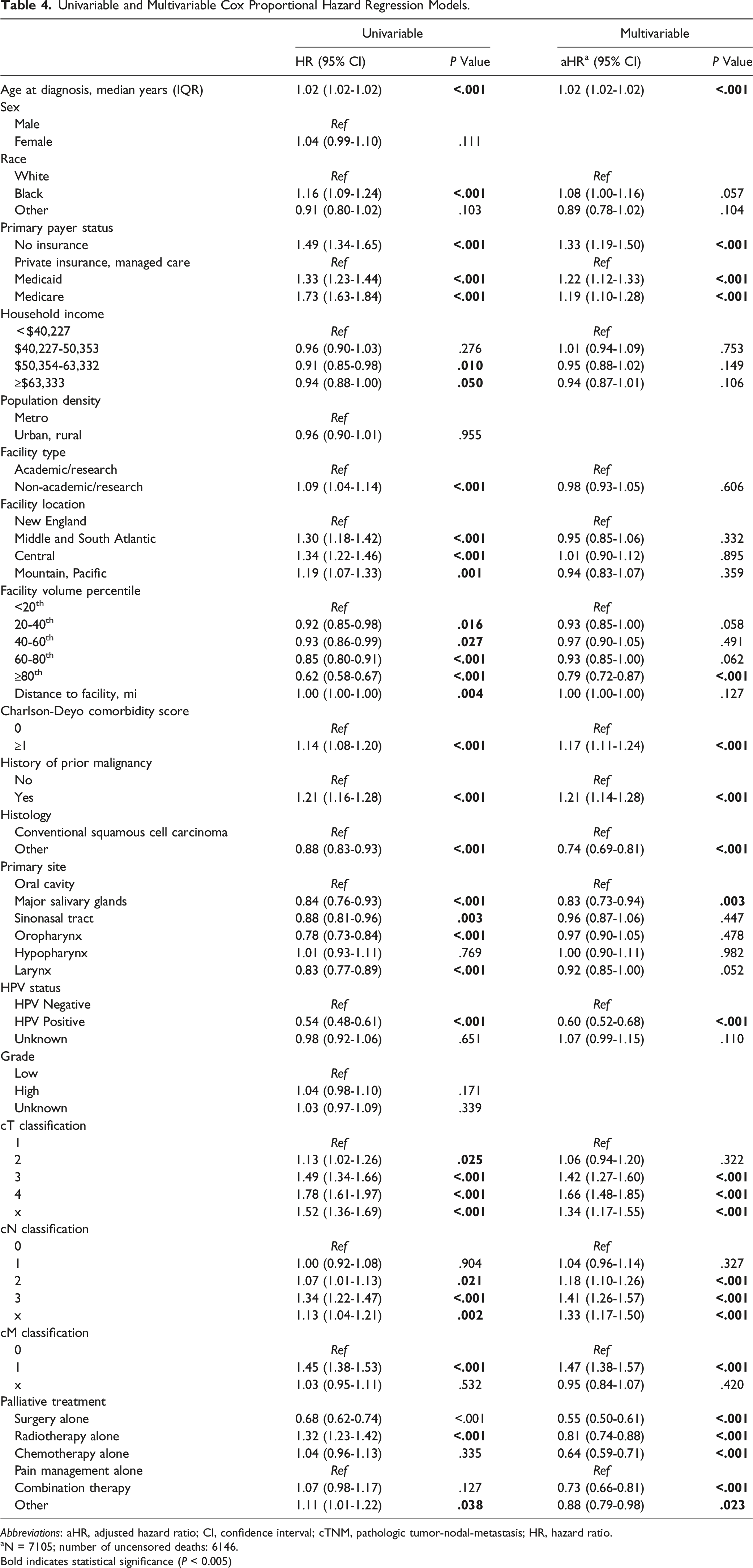
Abbreviations: aHR, adjusted hazard ratio; CI, confidence interval; cTNM, pathologic tumor-nodal-metastasis; HR, hazard ratio.
aN = 7105; number of uncensored deaths: 6146.
Bold indicates statistical significance (P < 0.005)
Kaplan-Meier Analysis and Multivariable Cox Proportional Hazard Regression Models of 5-Year OS After Binarizing Facility Volume at Varying Percentile Thresholds (Total Number of Facilities Included in Analysis: 984).
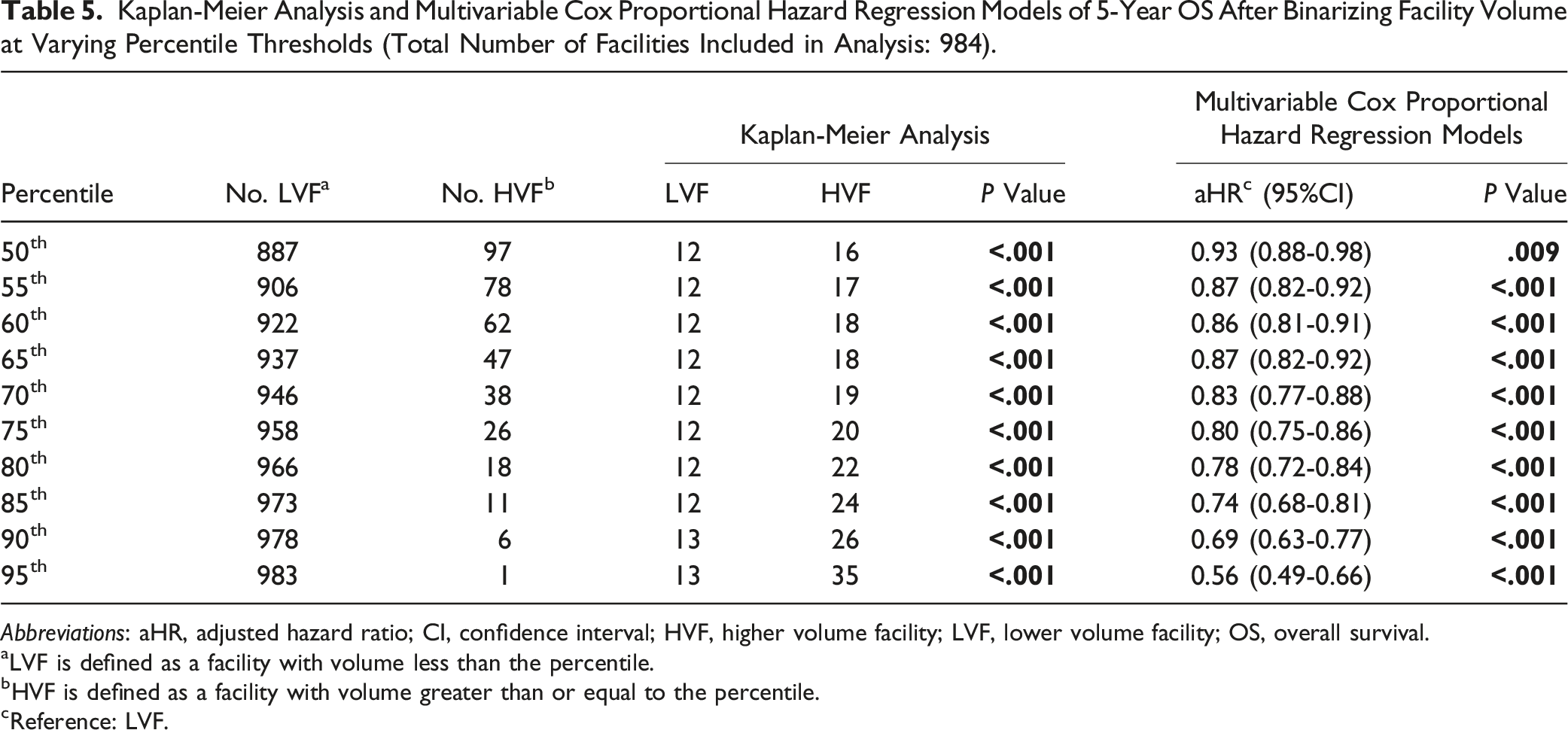
Abbreviations: aHR, adjusted hazard ratio; CI, confidence interval; HVF, higher volume facility; LVF, lower volume facility; OS, overall survival.
aLVF is defined as a facility with volume less than the percentile.
bHVF is defined as a facility with volume greater than or equal to the percentile.
cReference: LVF.
2-Year and 3-Year OS Sensitivity Analysis
Patients undergoing palliative treatment at facilities with volume <20th, 20-40th, 40-60th, 60-80th, and ≥80th percentile had 2-year OS of 20%, 22%, 23%, 25%, and 36%, respectively (P < .001), and 3-year OS of 15%, 17%, 16%, 19%, and 29%, respectively (P < .001). Undergoing palliative treatment at facilities with volume ≥80th percentile remained associated with higher 2-year (aHR 0.80, 95% CI 0.73-0.88, P < .001) and 3-year OS (aHR 0.81, 95% CI 0.73-0.89, P < .001) on multivariable Cox regression.
3-Month, 6-Month, and 12-Month Landmark Survival Analysis
1899 (21.9%) patients had survival time <3 months. After censoring survival time <3 months, facility volume ≥80th percentile (aHR 0.87, 95% CI 0.78-0.98, P = .020) remained associated with OS on multivariable Cox regression.
3506 (404%) patients had survival time <6 months. After censoring survival time <6 months, facility volume ≥80th percentile (aHR 0.94, 95% CI 0.82-1.07, P = .369) was not associated with OS on multivariable Cox regression.
5305 (61.1%) patients had survival time <12 months. After censoring survival time <12 months, facility volume ≥80th percentile (aHR 1.05, 95% CI 0.88-1.25, P = .630) was not associated with OS on multivariable Cox regression.
Discussion
Palliative treatment involving pain management and comfort care plays an essential role in offering support to patients with terminal illnesses and their families. 38 Higher OS has been demonstrated in patients with HNC undergoing curative treatment at HVFs.27-31 The results of our study suggest that undergoing palliative treatment at HVFs is independently associated with higher OS. Although treatment goals are shifted towards patient comfort in the palliative setting, improved survival may be an added benefit of successfully implemented palliative treatment regimens.
Undergoing palliative treatment at a facility with volume ≥80th percentile remained an independent predictor of improved survival after adjusting for patient and treatment factors. Further sensitivity analyses demonstrated that increased volume was associated with higher OS starting at the 50th volume percentile. This finding may be explained by the multidisciplinary teams and other resources in HVFs which facilitate complex procedures requiring extended LOS, intensive care, or outpatient care. 39 Moreover, the unique challenges of palliative treatment in HNC may be better addressed through coordination of multiple specialists, outpatient support staff, and comprehensive treatment plans. Collaboration among experienced professionals across all treatment modalities may aid in determining the most appropriate treatment for each patient and likely contributes to lower complication rates evident in HVFs. 40 It is, however, important to recognize that patient outcomes are multifactorial, and our study does not suggest that optimal care is exclusive to HVFs but highlights the potential benefits of improving access to these facilities. Most importantly, patient-directed goals of care should be the measure of success, as comfort, rather than prolonged survival, may be the priority for many patients undergoing palliative treatment.
Palliative management of HNC often involves various treatments to enhance patient quality of life. Our study found that palliative management most frequently involved radiotherapy (32.3%), pain management (16.3%), chemotherapy (15.7%), or surgery (15.6%) alone. Palliative surgeries, such as tracheostomy, enteral feeding procedures, and tumor debulking, aim to control symptoms and improve swallowing, nutrition, and airway in active and self-caring patients. 25 Surgical treatment was associated with undergoing treatment at HVFs, possibly attributed to greater access to resident doctors, hospital resources, and diverse multidisciplinary personnel which aid in performing complex palliative surgeries. Non-surgical treatment modalities, including pain management, were associated with decreased odds of undergoing palliative treatment at an HVF, as they may be more standardized, widely accessible, and less resource intensive, making them suitable for a variety of healthcare settings. Our analysis of palliative treatment is likely confounded by stage. Compared with those undergoing pain management, patients undergoing surgery likely had either less advanced disease increasing the likelihood of tumor eradication, or more advanced disease warranting surgical intervention for symptom palliation and restoration of bodily functions such as breathing. Patients undergoing palliative surgery may also have responded to induction therapy, which is not reported in the NCDB.
Our study found that undergoing surgery, radiotherapy, chemotherapy, or combination therapy was associated with higher OS than pain management alone in the palliative management of HNC, consistent with previous studies.41,42 Of note, a selection bias may account for patients with less advanced disease undergoing surgery, as these patients may have been more amenable to surgery or had already responded to induction therapy, but these factors are not documented in the NCDB.
5-year OS rates of patients undergoing palliative therapy were significantly greater at HVFs. Although HVFs have more experience with surgery, which remains the mainstay of HNC treatment, the survival benefit at HVFs did not persist among patients with distantly metastatic disease, which is generally managed with pain management or systemic therapy as opposed to intensive localized therapy (i.e., surgery or radiation). 43 Although speculative, this may suggest that the survival benefit of palliative treatment at HVFs may be most appropriate for patients amenable to localized therapies such as surgical resection, rather than those with metastatic disease.
Our study found increased comorbidities, prior malignancy, and more advanced tumors were associated with poorer survival, whereas HPV positive disease was associated with improved survival, consistent with previous studies.44-46 Older age was also a negative prognostic factor for survival, consistent with literature attributing this trend to greater comorbidities and diminished functional status.47,48 All primary payer statuses portended poorer survival compared with private insurance/managed care, consistent with prior studies in HNC.49,50 This underscores health insurance status as an important factor influencing healthcare decision-making, and possibly serving as a proxy for other socioeconomic factors impacting survival. 51 For example, tobacco use, a variable not reported in the NCDB, is twice as likely among patients with Medicaid compared with those with private insurance. 52
Despite the large sample size, our study is inherently limited by its retrospective study design and inability to establish causal relationships. Most importantly, factors relevant to palliative decision making such as quality of life, feeding dependence, and pain management, extend beyond survival alone and are often not sufficiently captured in large retrospective databases such as the NCDB. Although our study associated HVFs with higher OS, disease-modifying palliative treatments encoded in the NCDB do not capture the full spectrum of palliative care, previously defined as “an organized program providing specialized medical care, drugs or therapies for the management of acute or chronic pain and/or the control of symptoms administered by specially trained physicians and other clinicians; and supportive care services, such as counseling on advanced directives, spiritual care, and social services, to patients with advanced disease and their families.”38,53-55 Review of the NCDB presents the possibility of inaccurate histologic diagnosis and variable miscoding due to differing reporting standards across healthcare centers. Selection bias is also an inherent limitation, as patients reported in the NCDB undergo treatment in a select group of treatment facilities in the United States. The NCDB does not encode locoregional control and disease-free survival, potentially confounding survival analysis. The NCDB also lacks patient-level socioeconomic data, rather utilizing an ecologic approximation of resident zip code. 56 Although our multivariable analysis controlled for several variables, unmeasured confounders including socioeconomic status, comorbidities, functional status, and palliative treatment goals not reported in the NCDB likely influence OS, further restricting causal inference. Patients in our cohort may have undergone treatment with curative intent prior to palliative treatment, which is not encoded in the NCDB. Nevertheless, despite these limitations, our study found that HVFs were associated with higher OS in HNC palliative treatment. 57
Conclusion
Patients undergoing surgery had increased odds of undergoing palliative treatment at a facility with volume ≥80th percentile. After adjusting for patient demographics, facility characteristics, cTNM classification, and treatment, undergoing palliative treatment at a facility with volume ≥80th percentile was associated with higher OS, although this survival benefit was not observed for patients with cM1 disease. Older age, non-private insurance status, and non-surgical treatment were associated with worse OS. Facility volume alone does not determine survival outcomes and should therefore be considered as one of the many variables involved in maximizing quality of life during end-of-life care.
Footnotes
Author Contributions
Praneet C. Kaki: design, analysis, interpretation, manuscript writing; Aman M. Patel: conception, design, analysis, interpretation, manuscript writing; Lucy Revercomb: conception, design, analysis, interpretation, manuscript writing; Russell Maxwell: design, analysis, interpretation, manuscript writing; Robert M. Brody: design, analysis, interpretation, manuscript writing; Jason A. Brant: design, analysis, interpretation, manuscript writing; Ryan M. Carey: design, analysis, interpretation, manuscript writing, final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.