
Abstract
Background
Antibiotics are frequently prescribed at the end of life, though the benefits and harms are not well understood.
Methods
We abstracted relevant findings from articles published in English in the past 25 years to answer questions generated by discussion among the authors and with stakeholders in Palliative Care and Infectious Diseases.
Findings
Prescribing practices vary based on individual situation and geographic location. Patients with cancer and those hospitalized receive more antibiotics than those enrolled in outpatient hospice. Urinary tract infections and pulmonary infections are the most common conditions treated with antibiotics at the end of life -most often with penicillin derivatives and vancomycin in the hospital, fluoroquinolones in outpatient, and cephalosporins in both settings. When asked, patients most often prefer limiting antibiotics to symptom management at the end of life. Physicians’ over-estimation of patient preference for antibiotics and the increased probability of misdiagnosis increases antibiotic prescription rates. Antibiotics can improve symptoms when used for specific diseases at the cost of drug reactions, resistant organisms, and delayed discharge. Antibiotic use has variable results on survival duration. Antimicrobial stewardship exists in hospital and long-term care facilities, but not outpatient hospice groups. Stewardship interventions could increase proper use of antibiotics, but more information is needed to apply these interventions to hospice groups.
Conclusions
Antibiotics at the end of life are impactful and efforts to educate patients and providers will be invaluable in optimizing care.
Introduction
Death is a natural part of life. The transition from life to death takes many forms: sometimes painful, sometimes peaceful; sometimes unexpectedly, sometimes long-anticipated. Medical care in the period prior to death is similarly variable, with some patients receiving intense care in the hospital or intensive care unit (ICU) or others focusing on comfort and time with family at home. 1 In all scenarios, antibiotics are often used to treat suspected or confirmed infections or to palliate symptoms.
Choosing when to use antibiotics at the end of life is rarely straightforward. Clinicians must identify infection and match antibiotics with suspected organisms, all while weighing benefits and risks for the patient. Patient and family goals often shift to prioritize quality of life over survival when the end of life approaches. 2 At the end of life, the balance of risk and benefit from aggressively treated infection shifts as antibiotic toxicities and side effects can be amplified by patients’ terminal illnesses. Prescribers must approach these situations thoughtfully, guided by patient preferences and the best available scientific evidence in this unique patient population.
At the end of life, care varies depending on the patient’s care goals, location of care, and overall medical condition. For example, patients with cancer are often treated in the outpatient setting by their oncologists, while others with advanced illness such as advanced dementia or heart failure are managed by primary care providers, hospitalists, or palliative and supportive care clinicians. While a majority of patients die in a medicalized setting rather than at home, rates of dying at home are increasing.1,3,4 Infectious Diseases specialists are most often not involved in goals of care discussion or initial antibiotic selection unless patients are hospitalized for infection. However, the insights and education infectious disease experts can provide when involved are invaluable. 5 We will consider the diverse types of patients managed at the end of life, pointing out distinctions as appropriate.
In this narrative review, we will assess the literature to answer relevant questions for clinicians managing antibiotics at the end of life. Primary outcomes include the current state of care, and secondary outcomes focus on how this care is changing and what efforts have been made to improve care at the end of life. How often are antibiotics used and for what conditions? What are patient, physician, and family perspectives of antibiotic use? What are the impacts of these antibiotics – both positive and negative? How can antimicrobial stewardship efforts best address these unique populations?
Methods
The authors discussed dilemmas relevant to providers caring for patients at the end of life, particularly in the palliative or hospice setting. From these discussions, common themes were identified and used to generate a list of questions. These were further discussed with physician and pharmacist specialists in Palliative care and Infectious Diseases.
We then conducted a review of literature published in English in the past 25 years. We started with a search of Embase and Medline using keywords “palliative care, terminal care, hospice care, antibiotic agent.” Articles were reviewed for relevance and findings relevant to previously generated questions were abstracted to a database. Further articles were identified from references of those articles reviewed. This yielded 80 articles which were reviewed, 41 of which were deemed to be relevant to the questions identified.
Findings
How Are Antibiotics Used at the End of Life?
How Often Are Antibiotics Prescribed at End of Life?
Antibiotics are prescribed in up to 96% of patients hospitalized with cancer and 18%-52% of patients enrolled in hospice or palliative care, representing hundreds of thousands of prescriptions. 6-9
Rate of Antibiotics Based on End-of-Life Scenario.
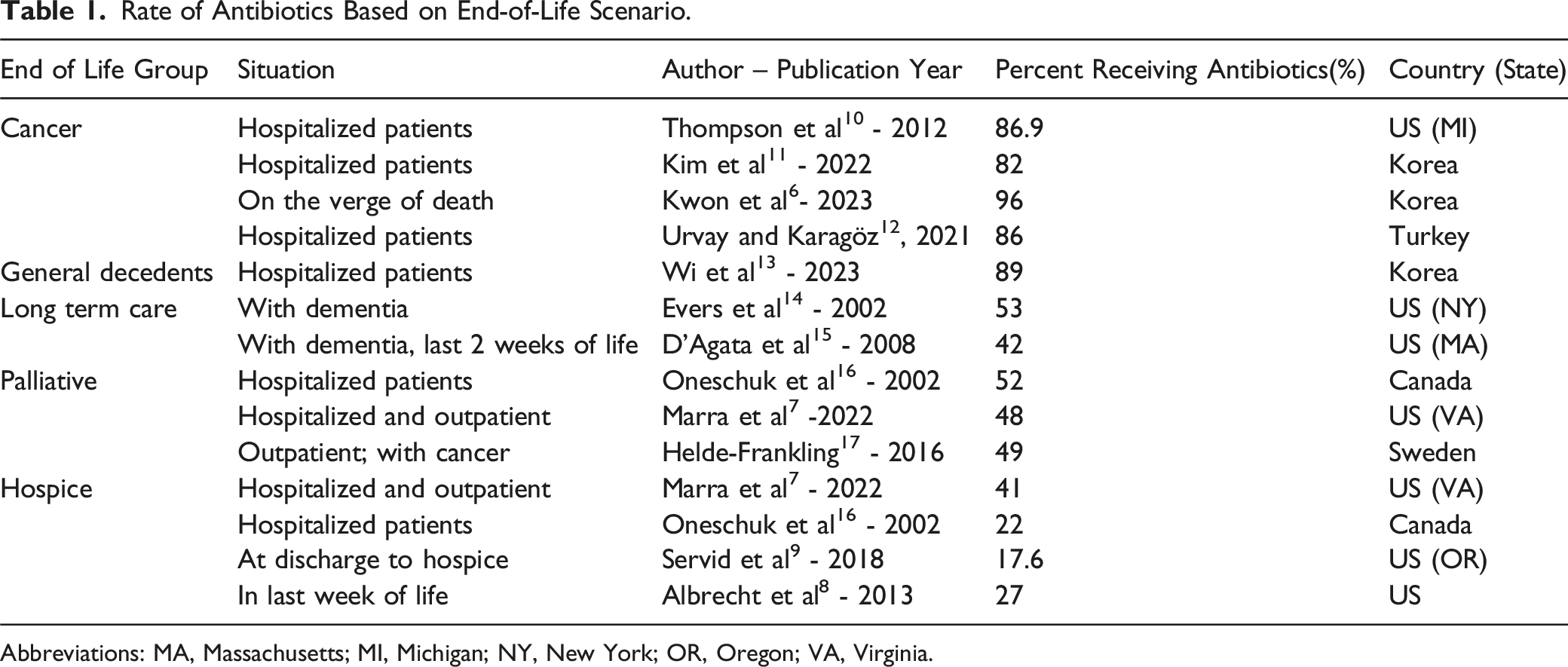
Abbreviations: MA, Massachusetts; MI, Michigan; NY, New York; OR, Oregon; VA, Virginia.
Patients with cancer commonly receive antibiotics at the end of life, up to 96% admitted to the hospital “on the verge of death.”6,10-12 This includes 81% receiving antibiotics up to the date of death. Patients with cancer are generally considered immunosuppressed due to their malignancy and treatment. Thus, antibiotics are often used more liberally in response to non-specific signs and symptoms common in advanced cancer – fever, hypotension, cough, hypoxia, or leukocytosis.
Patients dying in the hospital similarly receive antibiotics frequently.13,14 A nationwide study of patients dying in the hospital in Korea found 89% of decedents received antibiotics, and 44% of all patients received a carbapenem. 13 There is a relatively lower rate of prescribing among those with dementia than those hospitalized for cancer, though still 40-52% of these patients receive antibiotics at the end of life.14,15
Patients admitted under palliative hospital services similarly receive antibiotics around half of admissions.7,16,17 This percentage falls for those after enrollment or discharge into hospice services, falling from 41% of patients in the hospital down to 17.6% at time of discharged to home hospice.7-9,16 Given that 1.5 million patients were enrolled in hospice in 2020, this minority of patients represents hundreds of thousands of antibiotic courses yearly. 18 Only 15% of patients receiving antibiotics in the last week of life had an infection-related diagnosis recorded at the time of starting antibiotics. 8
The largest study to date by Marra et al from the Iowa Veterans Administration (VA) assessed 9808 Hospice and 40 796 Palliative patients matched to patients not enrolled in these services. 7 41% of patients in hospice received antibiotics within 14 days of enrollment, compared to 25% in the matched cohort. 48% of patients enrolled in palliative care received an antibiotic compared to 27% of matched patients. This trend may represent increased interaction with physicians. For comparison, in hospitalized cancer patients who transitioned from full code to comfort measures only, 35.4% continued antibiotics. 10
Antibiotic use is very common at the end of life. Potential benefits and risk of adverse effects or resistance are great, making efforts to improve stewardship crucial, as will be discussed later.
What Conditions Are Treated With Antibiotics at the End of Life?
The most common conditions treated with antibiotics in patients at the end of life are urinary tract infections (UTI) and pulmonary infections.19-26
Site of Infections Treated with Antibiotics.

Abbreviations: NR, none reported; PPX, prophylaxis; SUP, Suppressive.
Bold indicates the class of infection that is most common, showing that UTI and pulmonary infections were the most common.
Which Antibiotics Are Used at the End of Life?
Cephalosporins are the most common class of antibiotics in both inpatient and outpatient settings; vancomycin and penicillin-derivatives are more common in the hospital, fluoroquinolones are more common in the outpatient setting. 10,19,21,22,27-29
Antibiotics Used.
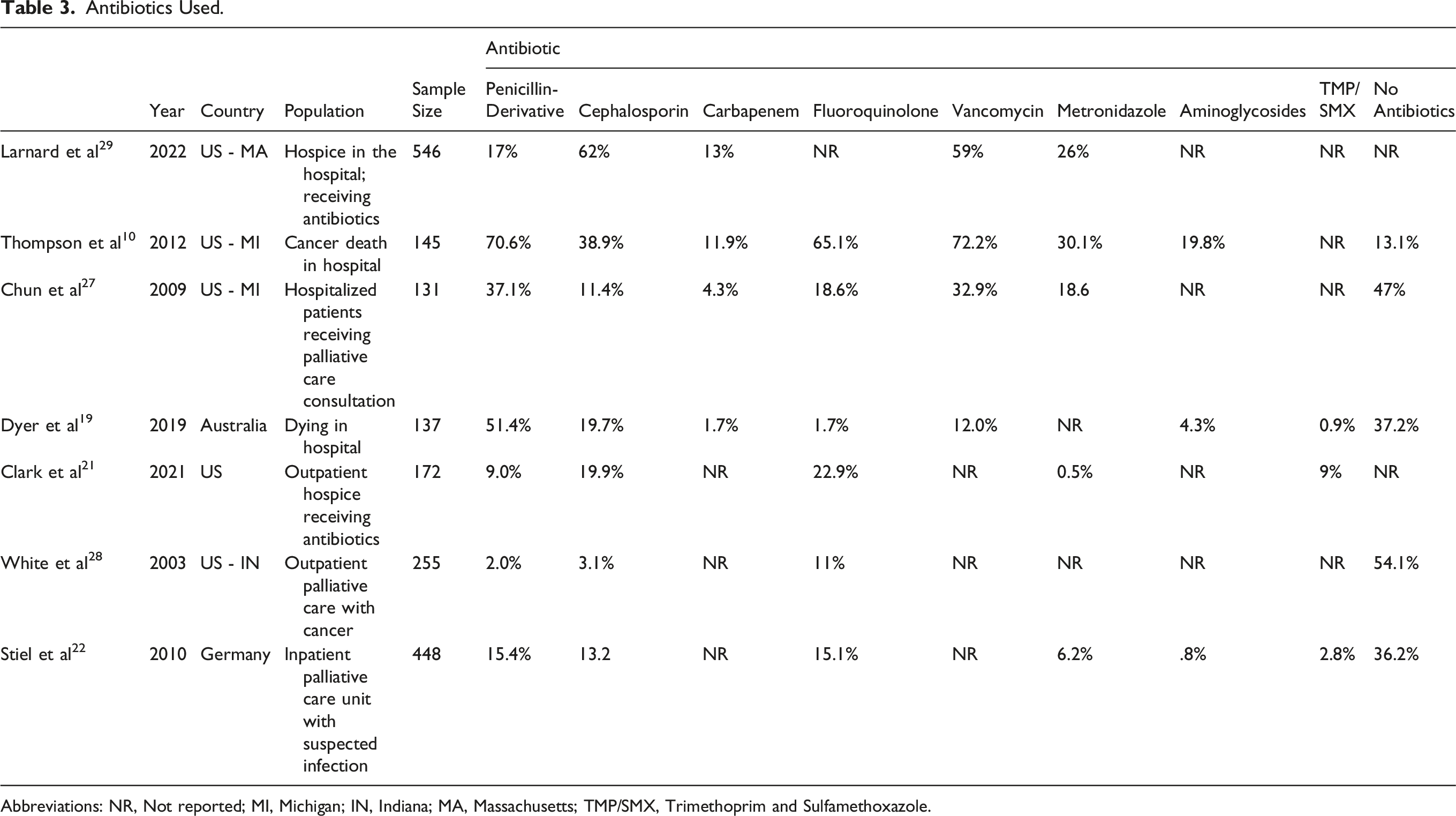
Abbreviations: NR, Not reported; MI, Michigan; IN, Indiana; MA, Massachusetts; TMP/SMX, Trimethoprim and Sulfamethoxazole.
Data on outpatient antibiotic prescription at end of life are older and more limited. Fluoroquinolones, trimethoprim/sulfamethoxazole (TMP/SMX), and cephalosporins were the most commonly prescribed antibiotics.21,22,28 TMP/SMX was the most commonly used antibiotic for UTIs (13/54 cases) while levofloxacin was the most commonly used for respiratory tract infections (13/45). 28 Cephalexin was most common for skin and soft tissue infection (6/12 cases).
What Are Physician, Patient and Family Perspectives About Antibiotic Use?
Patients often prefer limited antibiotic use, though physicians default to more aggressive use in the absence of clearly stated requests from patients and their families. 11,23-26,28-30
Physicians report concern for patient or family wishes drive antibiotic use at the time of enrollment to hospice or when death is expected imminently.23,24,28,29 41% of US clinicians surveyed stated they “often” continued antibiotics after a patient is transitioned from treatment of disease to comfort measures only (CMO). 29 Patient/family preference was the most common reason given for continuing antibiotics (78% of respondents) followed by palliation of symptoms (62%). 28% reported “completing an outlined treatment course,” which may indicate treatment inertia despite a change in management context. A key study of 255 patients with advanced cancer were asked at the time of enrollment into hospice whether they would prefer 1) antibiotics for suspected or proven infection, 2) antibiotics for management of symptoms only, or 3) no antibiotics. 28 Of the patients, 79.2% chose either no antibiotics or only if used to treat symptoms. There was significantly less antibiotic use in those requesting only for symptom management (36.6% of patients receiving) or not at all (2.5%), compared to in any infection (56.6%). There may be cultural differences, though, as 45.8% of patients in Taiwan expressed a wish for antibiotics even in terminal stage, with 26.4% desiring no antibiotics. 25
Care is likely to be more intense if wishes are not adequately discussed. In one study, palliative care consultation at the end of life significantly reduced the percent of patients with terminal cancer in the hospital who received antibiotics, from 82.2% to 73.5% in those with consultation. 11 However, a large study by the US Veterans Administration (VA) found more patients who were enrolled in hospice or palliative care in the outpatient setting had a higher rate of antibiotic use than matched decedents who were not enrolled. 7 Rather than showing regional variation, we interpret this to reveal a better connection to medical care facilitated by these specialty clinics.
Internal Medicine subspecialists who provide care at the end of life in the US were surveyed regarding their practices. Of them, 81% would consider withholding antibiotics if a patient’s terminal condition worsens and 66% considered additional IV antibiotics to be an escalation of care. 26 While 96% of these physicians believed decisions should involve patients and surrogates, only 51% reported discussing antibiotic use during goals of care. 31 They reported concerns about overwhelming families and a lack of specific training in end-of-life discussion.
Antibiotic decision-making practices in palliative care vary significantly across different countries. In Germany, the national “Hospice and Palliative Evaluation” (HOPE) provider survey assessed antibiotic decision making for real patients admitted with active or suspected infection. 22 They showed 44.1% of the time, the decision to start an antibiotic was made solely by the treating physician, and 25.5% were “team decisions.” The decision to stop antibiotic therapy, however, was made solely by the physician 21.1% of the time and “as a team” 42.1% of the time. When Brazilian physicians treating advanced palliative patients in their respective hospitals were given hypothetical cases, they started antibiotics in 88-100% of suspected infections for patients with terminal diseases, depending on the syndrome, with one exception - respondents opted to use antibiotics for Bronchopulmonary infection in a patient with severe dementia 45% of the time. 30 They then asked if clinicians would continue antibiotics if there were no improvement in 72 h. With the exceptions of dementia and multi-organ failure, most clinicians would continue antibiotics. 30 Younger doctors and those with specialty training in Palliative care felt more comfortable stopping antibiotics if there was no improvement.
These results highlight the benefits of improving communication skills for
What Are the Impacts of Antibiotics Prescribed at the End of Life?
Antibiotics targeting specific syndromes can be effective to relieve symptoms, but it is unclear whether they provide more or better quality of life. IV antibiotics delay discharge.
Ethical considerations prevent randomized study of antibiotic administration at the end of life. It would be unethical to prevent initiation of antibiotics that both clinicians and families believe are necessary and beneficial, and it would be difficult to compare treated patients with those who could have been treated with antibiotics but were not. Most literature on the topic identifies a cohort of patients who die and work backward to evaluate the therapeutic decisions in the week prior or during their terminal hospitalization.8,17,31-33
Antibiotics are usually given to forestall death, but it is unclear if this goal is reached in patients already dying from non-infectious causes. Compared to patients whose antibiotics were continued after a message from pharmacist, there was a shorter time to discharge and a lower mortality rate in those whose antibiotics were discontinued. 17 Another study of outpatient palliative care found no difference in survival between the group who requested antibiotics and those who did not. 28 In a study of patients with delirium, treatment of positive urine culture was associated with two additional days of life on average, but no change in need for symptomatic medications. 34
Symptom relief is thus often the primary goal of antibiotics at the end of life. Treatment of pneumonia improved survival, but worsened subjective comfort. 35 Treated urinary tract infections often resolved completely with antibiotics (92% of those treated with TMP/SMX), but less than half of respiratory tract infections, skin or soft tissue infections, or bacteremia resolved with antibiotics. 28 Levofloxacin was the most effective for respiratory infections (46% resolution of symptoms). Thus, antibiotics may resolve infectious symptoms, but this is far from guaranteed. In outpatient hospice, 49% of antibiotic courses fully resolving targeted symptoms, with about 20% of oral courses stopped due to inadequate symptom improvement. 20 However, patients enrolled in inpatient palliative care experienced no difference in outcomes with antibiotics. 32 The HOPE survey found that German physicians reported “good” or “very good” outcomes on antibiotics 45.5% of the time, and “poor” or “very poor” outcomes 20% of the time. In Australia, parenteral antibiotics have been reported to show improvement in 52.9% of cases in confirmed infection in inpatient palliative settings. 36 This is not considered an option in the hospice setting, though, as parenteral treatments increase patient discomfort and caregiver burden.
In hospitalizations in the last 6 months of life, many patients receive care that could be considered non-beneficial
Like other therapies, antibiotics carry the risk for adverse drug reactions (ADR). A study of patients admitted to palliative care found 57.4% of them had an ADR with antibiotic use. 37 These side effects include C. difficile infection, rash, and anaphylaxis. Remarkably, the authors deemed 81.5% of all these ADRs preventable. A recent study of patients older than 65 with solid organ cancer on chemotherapy in the US showed that patients who received antibiotics were twice as likely to have adverse drug reactions. 38
Antibiotics pose a potential benefit if there is a clearly identified infection, but this diagnosis is complicated by limitations of diagnosis and treatment toward the end of life. As patients develop complications from their life-limiting illness, side effects and interactions of antibiotics preclude their use. As patients transition to hospice, diagnostic testing and IV access becomes progressively more limited. There may be survival benefits, though studies differ.
What is the Role of Antibiotic Stewardship in Treatment of Patients at the End of Life?
Stewardship efforts exist in the hospital setting and are now being implemented in long-term care facilities, but these are not tailored to the unique needs of patients at the end of life. Hospice-embedded stewardship programs do not currently exist.6,10,20,23,33,39-43
The development of antibiotic resistance is a concern for all patients, especially those at the end of life and in assisted living facilities. Among veterans in skilled nursing facilities (SNFs) sequentially cultured to determine acquisition of resistant organisms, 72% of residents were colonized with ciprofloxacin-resistant gram-negative bacteria (from 34% at enrollment), 63% with Methicillin-resistant S. aureus infection (MRSA) (from 13% at enrollment), 18% with vancomycin-resistant enterococcus (VRE) and 26% with ceftazidime-resistant gram-negative bacteria within 3 months. 39 A study in Israel found that 19% of patients admitted for at least 48 hours to the ICU develop MDRO. 33 While not the goal of Do Not Resuscitate (DNR) orders, resistant organisms were isolated more often from those without an order for DNR (Odds Ratio 2.62 95% CI 1.21-5.68). In another study, 5.6% of patients with cancer treated with antibiotics on average 13 days developed C. difficile. 10 These resistant organisms increase in frequency with antibiotic administration.
Like in other settings, many antibiotics are likely unnecessary. In patients enrolled in outpatient hospice who received antibiotics for UTI, 36% had no recorded symptoms, 44% had foul odor, and 44% had altered mental status, none of which are considered signs of UTI. 40 Dr Loeb and colleagues created a tool using consensus of diagnostic clinical criteria to define “minimum criteria” for common infections. 41 58% of antibiotic regimens for outpatient hospice failed to meet these Loeb’s Minimum Criteria. 20 These criteria do not involve lab results, but still show that clear diagnosis is hindered in Hospice care. Further, many antibiotics are prescribed in clinical uncertainty.
The primary goal of antimicrobial stewardship programs (ASPs) is to ensure that patients receive the appropriate antibiotic, dosed correctly, via the best route, for the ideal amount of time. The role of ASP at the end of life is complicated as there are competing priorities of enhancing patient comfort and reducing the promotion of resistant organisms. ASP may also be underrecognized, as a study in Korea showed 70% of physicians taking care of patients with terminal cancer were not aware of ASP in general. 6 As mentioned before, the expertise of Infectious Diseases physicians and pharmacists can play a role here, providing more awareness of these resources and improving care.
In a stewardship project in Singapore, ASP pharmacists recommended cessation of broad-spectrum, intravenous antibiotics in patients identified as at the end of life. 23 82% of antibiotic cessation recommendations made by the team were implemented. This intervention had no effect on rate of death from infection but allowed significantly faster discharge (10.5 days in those who continued antibiotics vs 6 days in those who stopped antibiotics). The most common reason intravenous antibiotics were continued after a message advising discontinuation was due to physician’s preference (45.5%), with only 4% of continued antibiotics due to family’s decision to continue. 23
The Physician Orders for Life-Sustaining Treatment (POLST) is a key, though underutilized tool to assist with stewardship of resources at the end of life.
44
It is a form designed for patients experiencing chronic or debilitating illness, particularly those illnesses likely to result in death (Figure 1). While the form can vary from state to state, the POLST asks questions related to care at the end of life, including CPR, care in hospital, antibiotics, and artificial nutrition. Use of the POLST resulted in a reduction of antibiotic use in patients with terminal cancer (IRR, 0.73; 95% CI, 0.59-0.90), largely driven by those specifying request for no antibiotics.
42
This finding refutes a previous study that reported no difference in antibiotic use if POLST was filled out.
43
The difference is likely due to larger power and more homogenous population in the newer study. The POLST serves as a starting point for discussion of patient wishes for antibiotic that can foster education for patients and families and prevent unwanted exposure to antibiotics. There is poor utilization for with less than a third of patients filling one out with their provider.6,42 Patient treatment preferences on Minnesota POLST.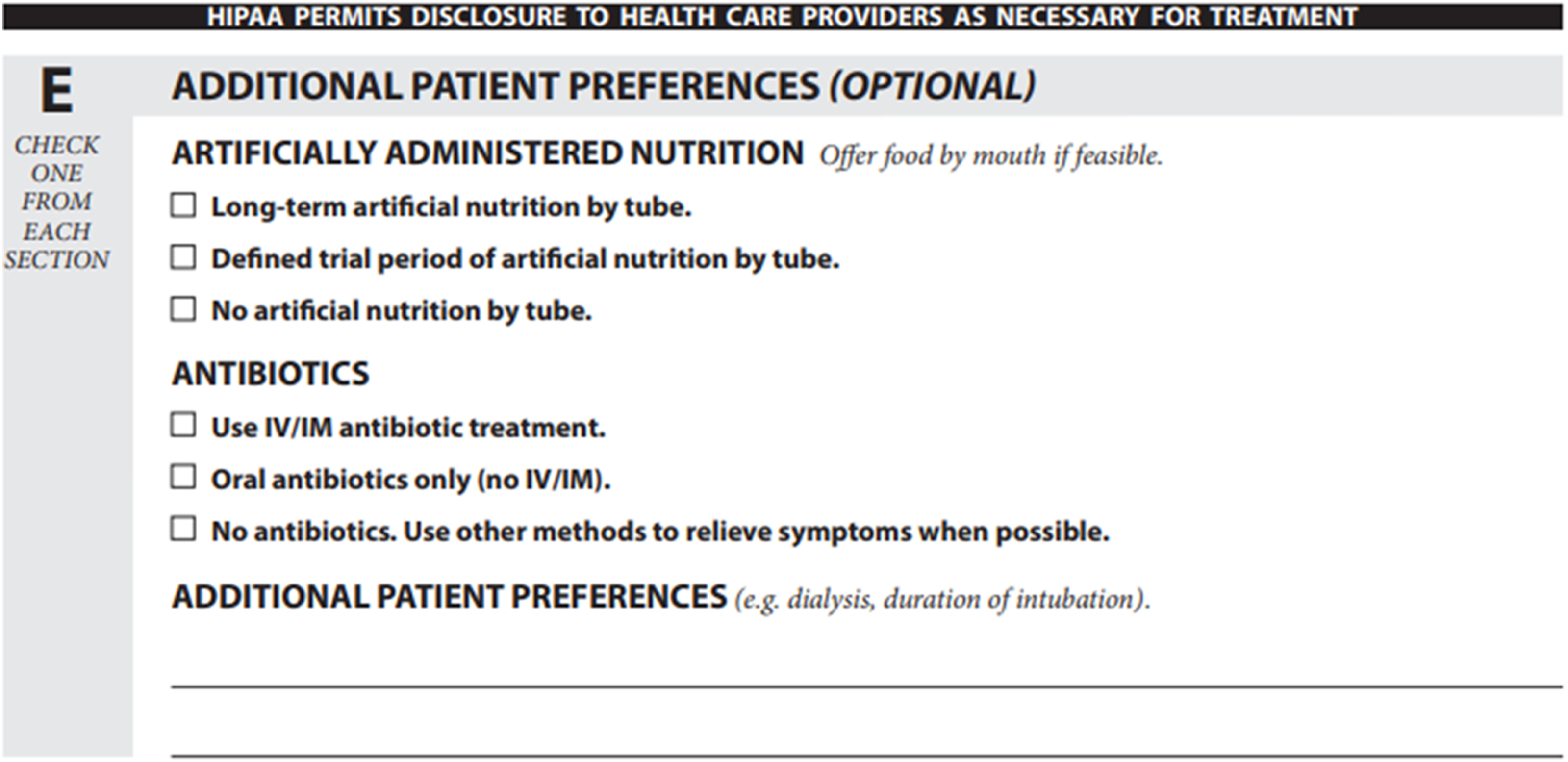
Stewardship represents an underutilized tool that can help improve care at the end of life, while also reducing the risk of propagating resistant organisms and superinfections, such as C diff. Beyond antibiotic stewardship programs, it may be important for health care systems and public administrators to better engage infectious disease specialists in educational strategies and research to better address the usage and limitation that antimicrobials may have at the end of life.
Conclusion
Antibiotics are prescribed often at the end of life for many conditions, though most often urinary or pulmonary infections. Rates and selection of antibiotics vary based on setting. Physician and family perspectives are broad. While physicians may defer to family wishes, initial discussions may omit antibiotics, likely leading to more aggressive care. The impacts of antibiotics are mixed. While they may prolong life and alleviating symptoms at the cost of prolonging hospitalization and placing the patient at risk of adverse drug reaction. While not typically considered a target for antimicrobial stewardship, studies have demonstrated potential value in inpatient palliative and hospice settings. Antibiotics that have less toxicity and risk of causing resistance should be considered, if possible, and IV medications should be avoided, particularly if discharge is a primary goal of the patient or family.
While it has recently been proposed that antimicrobial discussions at the end of life should be guided by Infectious Diseases providers, we recommend empowering all those clinicians treating patients at the end of life to discuss the benefits and hazards of antibiotics. 5 These discussions should be a part of goals of care discussions, including the benefits of stopping therapy if no benefit is seen or side effects develop. It is reasonable to propose a time-limited-trial (TLT) when the benefit of antibiotics are tenuous. 45 As proposed by Quill and Holloway, clinicians and patients or their families (1) jointly define prognosis and clinical concern, (2) clarify patient’s priorities, (3) identify markers for improvement, (4) decide a time frame for re-evaluation, and (5) plan next steps at the end of the TLT. This improves patient-clinician relationship and understanding and helps side-step treatment inertia that can dog treatment at the end of life.
Larger studies of impact of antibiotics on survival would be of benefit in counseling patients and their families. Additionally, study of antibiotic selection and subsequent effect in the over a million yearly patients enrolled in outpatient hospice are needed. Lastly, antiviral and antifungal therapies have not been described.
Antibiotics at the end of life have a potentially large impact on comfort, palliation, complications, and discharge from hospital at the end of life. As knowledge of this impact continues to grow, patients and clinicians will be better informed in their use, improving care at this crucial time for patients and their families. We look forward to the growth of this field in the coming years.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.