
Abstract
Objectives
Identify the costs of an oncology patient at the end of life.
Methods
A systematic literature review was conducted by screening Embase, PubMed and Lilacs databases, including all studies evaluating end-of-life care costs for cancer patients up to March 2024. The review writing followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The quality of the included studies was assessed using the Drummond checklist. The protocol is available at PROSPERO CRD42023403186.
Results
A total of 733 studies were retrieved, and 43 were considered eligible. Among the studies analyzed, 41,86% included all types of neoplasms, 18.60% of lung neoplasm, All articles performed direct cost analysis, and 9.30% also performed indirect cost analysis. No study evaluated intangible costs, and most presented the macrocosting methodology from the payer’s perspective. The articles included in this review presented significant heterogeneity related to populations, diagnoses, periods considered for evaluation of end-of-life care, and cost analyses. Most of the studies were from a payer perspective (74,41%) and based on macrocosting methodologies (81,39%), which limit the use of the information to evaluate variabilities in the consumption of resources.
Conclusions
Considering the complexity of end-of-life care and the need for consistent data on costs in this period, new studies, mainly in low- and middle-income countries with approaches to indirect and intangible costs, with a societal perspective, are important for public policies of health in accordance with the trend of transforming value-based care, allowing the health care system to create more value for patients and their families.
Keywords
Introduction
Health costs in cancer have shown significant growth in recent decades and are an issue of great importance worldwide. 1 A recent study conducted by All Together Against Cancer movement and the Oncology Observatory, in partnership with the Center for Strategic Studies of Fundação Oswaldo Cruz (Fiocruz), showed that spending on oncology treatment in the Unified Health System in Brazil is approximately 800 million US dollars in 2023, with expenses in the outpatient and hospital areas included. 2 Another relevant aspect is that cancer-related expenses represent a significant proportion of health expenses, and aging and population growth are expected to increase the costs of cancer care from $183 billion US dollars in 2015 to about $246 billion US dollars in 2030 in the United States. 3 The estimate of the global economic cost of cancer between 2020 and 2050 is 25.2 trillion US dollars (in international dollars) and considering constant 2017 prices, that is, a value equivalent to an annual tax of 0.55% on global gross domestic product. 1
According to previous research, it has been observed that the initial year following the diagnosis of cancer and the final year of cancer patients are the periods that are associated with the greatest expenditures and resources in the treatment process.4,5 Despite the development of palliative care in recent decades and studies indicate that assistance from a team specialized in palliative care promotes better control of symptoms and quality of life, reducing aggressive or obstinate measures, enabling better allocation of resources and lower costs for health systems,6-8 the appropriate end-of-life care is still difficult to access in low- and middle-income countries 9 and is often not offered to patients with advanced cancer without curative possibilities. In this context, assessing costs in end-of-life care is important to identify which resources and expenses have the greatest economic impact on health systems in this period.
The objective of the systematic review was to identify the tangible and intangible costs of an oncology patient at the end of life.
Method
This study was developed according to the structure of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 10 The protocol for this review was registered on the PROSPERO platform with the number CRD42023403186. The research comprised steps in accordance with the guidelines provided in the Cochrane Collaboration Manual on Systematic Reviews of Interventions. 11
Eligibility Criteria
This review selected articles with cohort study design of patients diagnosed with advanced cancer, regardless of race, age, or gender, with an assessment of direct, indirect, and/or intangible costs involved in providing end-of-life care. The analysis did not include reviews, comments, case reports, and conference abstracts.
Data Source and Search Strategy
A systematic search of academic literature was carried out from March 2023 to March 2024 using three electronic databases, Embase, PubMed and Lilacs without publication date restrictions. The search strategy was structured using the key concepts of costs, end-of-life care and cancer, developing the appropriate search strategy for each research base. Supplementary Material 1 presents the search strategies and results found in each base. Endnote reference management software (Endnote 21.1) stores the extracted studies.
Study Selection
The study selection process involved three steps, with two independent reviewers (SCIS and CEAM). In the first stage, all the studies were exported to Endnote and the duplicates were removed. In the second stage, through the analysis of the titles and abstracts of the remaining articles, it was possible to define the articles regarding their eligibility for full-text search. Studies considered ineligible were excluded. In the third stage, articles considered eligible were independently analyzed in full for inclusion. Any point of divergence was discussed between the reviewers, and in situations of any discrepancy between the reviewers, it was discussed and resolved by two other team members (CGB and RJVAH) to establish the articles included in the systematic review.
Data Extraction
Characteristics of the Studies.

Methodological Quality of Studies
The quality of the included studies was assessed using the Drummond 13 checklist, which was designed to guide the critical analysis of economic evaluations and considers 10 points: 1. Was a well-defined question posed in answerable form?, 2. Was a comprehensive description of the competing alternatives given? 3. Was the effectiveness of the programme or services established? 4. Were all the important and relevant costs and consequences for each alternative identified? 5. Were costs and consequences measured accurately in appropriate physical units? 6. Were the cost and consequences valued credibly? 7. Were costs and consequences adjusted for differential timing? 8. Was an incremental analysis of costs and consequences of alternatives performed? 9. Was allowance made for uncertainty in the estimates of costs and consequences? 10. Did the presentation and discussion of study results include all issues of concern to users?.
A proposed assessment scale, developed by Doran, 14 was used to assign a potential score from zero to 1 for each of the checklist items. The aggregated results provide an assessment of economic quality according to the total score: poor (1-3 points), average (4-7 points), and good (8-10 points). The authors, SCIS and CEAM performed an independent assessment of the quality of the included economic evaluations. The detailed quality assessment of the Drummond checklist is presented in Table 3.
Analyzes
The data extracted from the selected studies were evaluated according to the methodology used to evaluate heterogeneity, considering the way of selecting patients, oncological diagnoses, design, comparison of patients’ clinical characteristics and analyzed costs. According to the results of the analysis of the heterogeneity of the studies, the meta-analysis stage can be carried out. 11
Results
Bibliographic Search Process
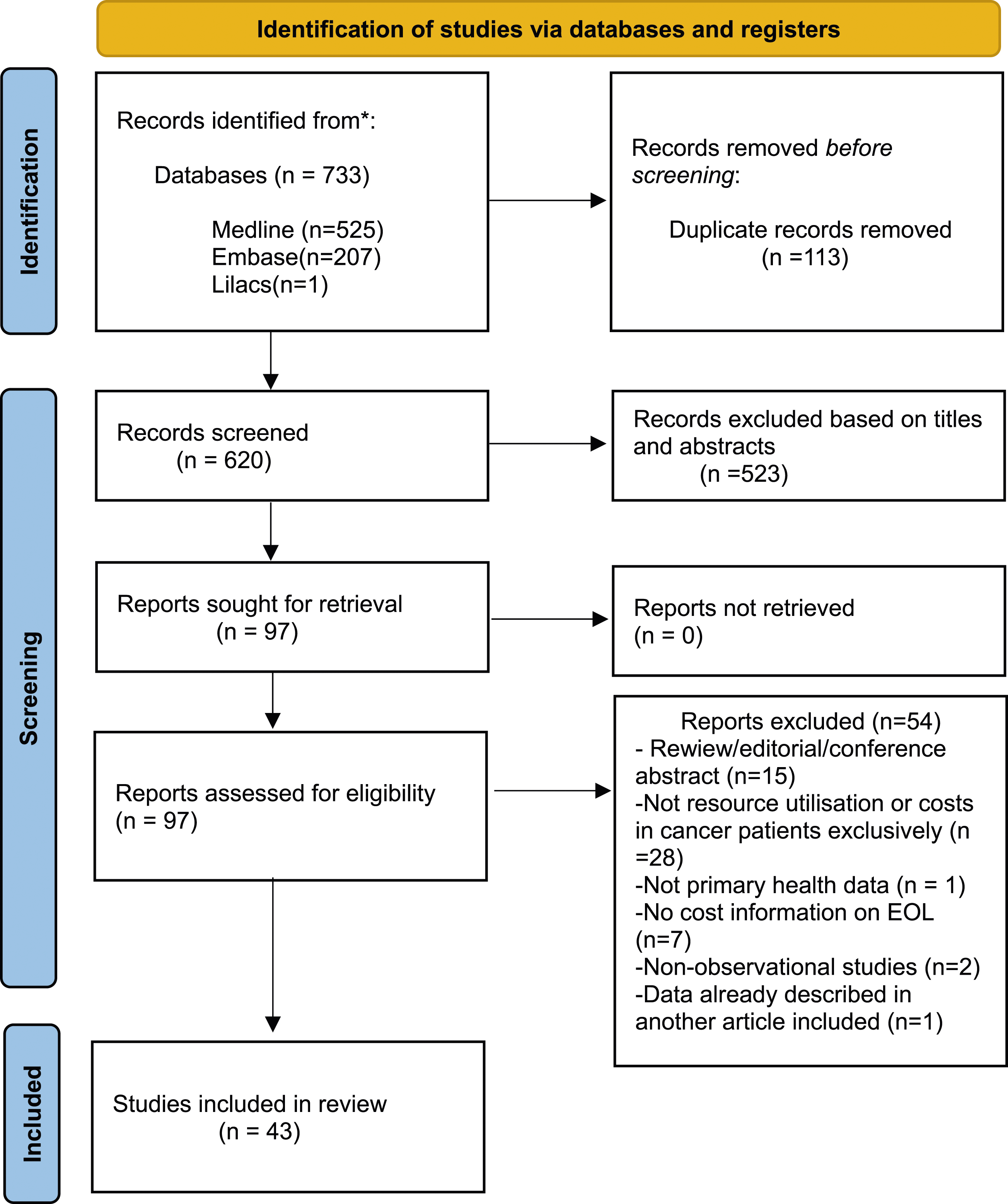
The search strategy proposed by the research identified 733 articles in all the selected databases. After a preliminary screening of titles and abstracts, 113 duplicate articles were removed, and 523 studies did not meet the inclusion criteria. A total of 97 studies remained for full-text analysis, and 43 studies were considered eligible for inclusion in the review, as described in Figure 1. Process of study inclusion in the systematic rewiew. *Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers). **If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools. From:
10
.
Characteristics of the Studies
Characteristics of Studies by Periods.
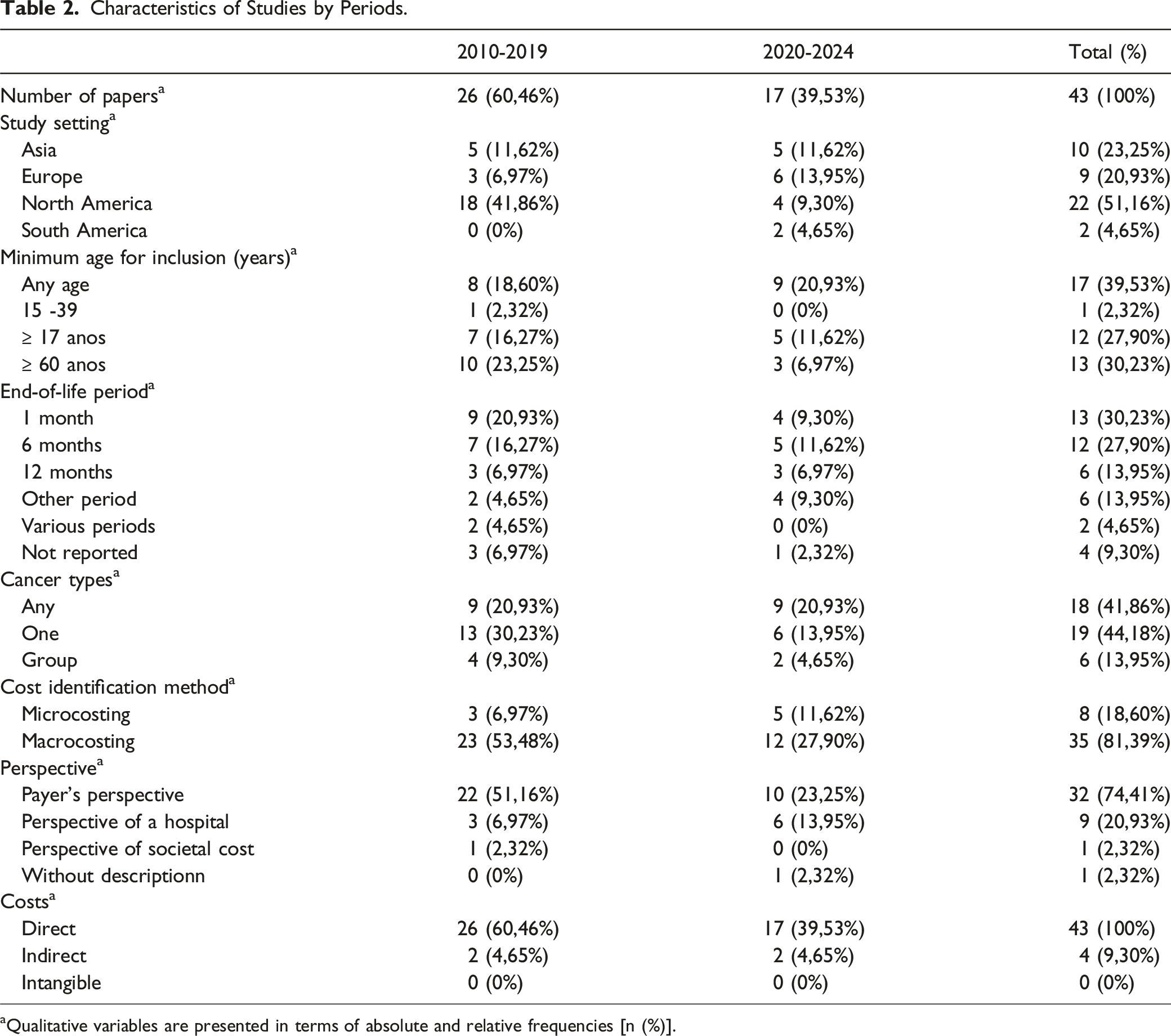
aQualitative variables are presented in terms of absolute and relative frequencies [n (%)].
The oncological diagnoses of the studies analyzed resulted in 18 studies (41,86%) including all types of neoplasms,15-32 and studies of a specific type of cancer, with eight studies (18.60%) of lung neoplasm,33-40 three studies (6.97%) of pancreatic neoplasm,8,41,42 two (4.65%) of breast cancer, 43,44 two (4.65%) of hepatocellular carcinoma,45,46 one (2.32%) of hematological neoplasms, 47 one (2.32%) of multiple myeloma, 48 one (2.32%) of brain neoplasm, 49 and one (2.32%) studies of gynecological neoplasms. 50 Joint evaluation of a group of solid neoplasms is present in seven studies (16.27%).51-56
Most of articles (83.72%) describe the concept of aggressive measures or active treatments in end-of-life care.8,16,18-28,30-35,37-42,44-50,52,54-56 The main measures described were chemotherapy and emergency room visits associated with hospitalizations. All articles performed direct cost analysis, and four (9.30%) also performed indirect cost analysis.15,17,29,54 No study evaluated intangible costs. The methodology for identifying health costs was macro-costing in 35 articles (81,39%).8,15,16,18,19,22,24-30,32,34-40,42-49,51-56 And micro-costing is mentioned in 8 articles (18.60%)17,20,21,23,31,33,41,50 among these, 1 article mentions top-down micro-costing 17 and 1 presents bottom-up micro-costing. 20
The perspective of the payer was observed in 32 articles (74,41%) of this review, with four studies presenting coverage of National Health Systems involving Ministries of Health.8,27,30,47 And in the most of US studies (30,23%) the Medicare perspective was used.16,28,36,37,40,42-44,48,49,53,55,56 The perspective of hospitals providing health care is present in 9 articles (20,93%) involving public or philanthropic hospitals associated with universities, most of them.17,20,21,23,31,33,34,41,50 Only one study highlights the perspective of the society, carried out in Canada. 29 This information is described in Tables 1 and 2.
The period considered for end-of-life care in the economic evaluation of 13 studies (30.23%) was the last 30 days of life,20,27,34,36,38,41,42,44,47-50,56 followed by 12 studies (27.90%) analyzing the last 6 months,16,18,22,30,31,35,37,39,40,45,52,53 and 6 studies (13.95%) considered the last year of patients’ lives.15,24,25,51,55 Six studies considered other periods,19,23,28,33,43,54 four studies (9.30%) did not establish a specific period,8,17,21,46 and two studies (4.65%) evaluated different periods of cohort follow-up to compare costs in end-of-life care.26,29
The studies selected samples ranging in size from 70 to 339,546 patients. Regarding the age range of patients, 17 studies (39.53%) did not define an age-specific,8,16-18,22,23,25,28,29,33,35,38,41,43,50,52,53 13 studies (30.23%) involved only elderly patients,15,26,36,37,39,40,42,44,46,48,49,51,55 and 13 studies (30.23%) involved adolescent and adult patients.19-21,24,27,30-32,34,45,47,54,56
Most of the studies in this review were developed by countries in the Northern Hemisphere, involving 41 studies, representing 95,34% of the total. Twenty-two studies (51.16%) were carried out in North America, seventeen (39.53%) in the United States, 16,19,24,26,28,36,37,40,42-44,48-50,53,55,56 and five (11.62%) in Canada.23,27,29,39,45 Ten (23.25%) in East Asia,8,22,25,31-33,46,51,52 nine (20.93%) in Europe 15,17,18,30,34,35,38,41,54 and two studies (4,65%) in South America.20,21
Quality of Studies
Drummond's Check-List for Assessing Economic Evaluations.
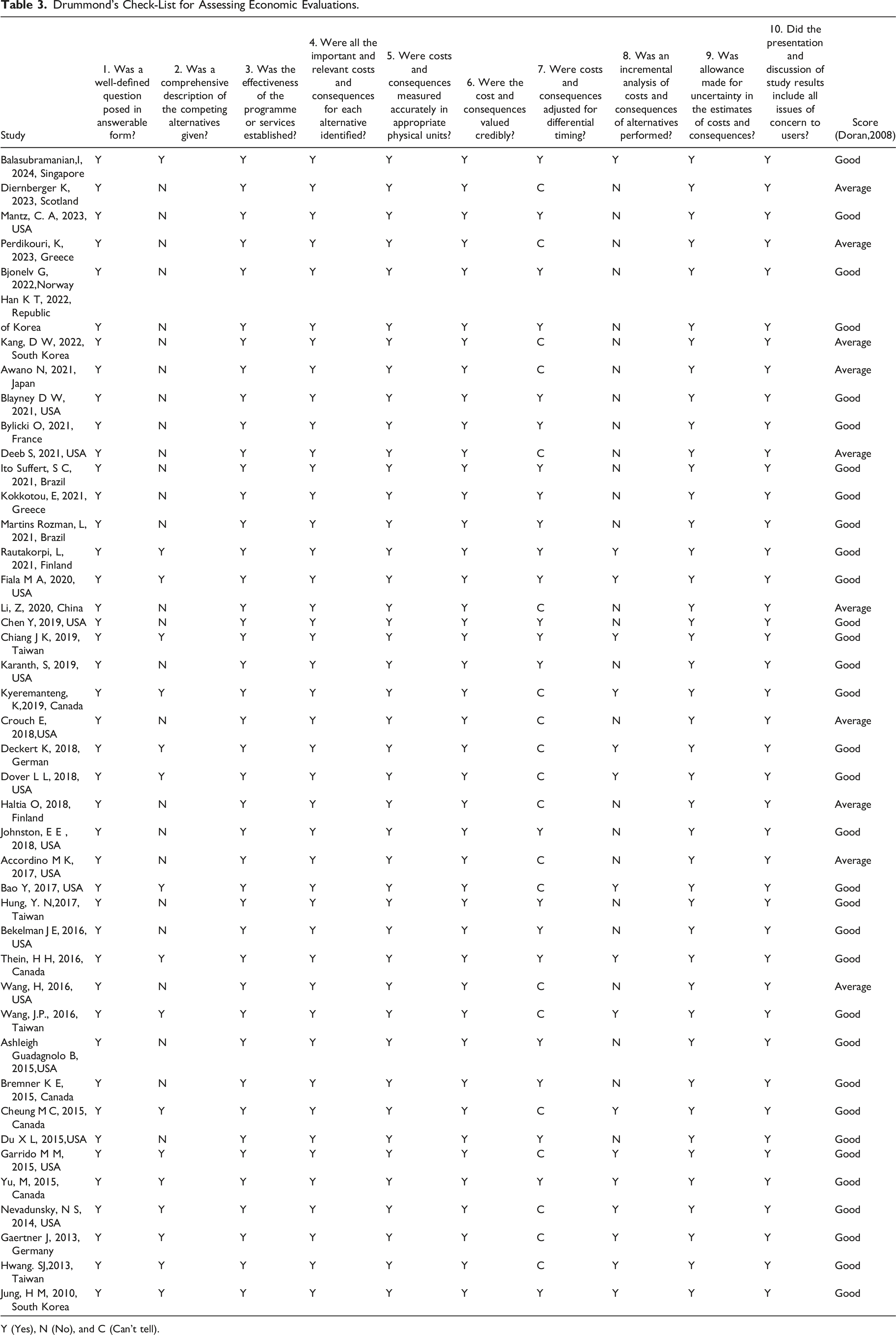
Y (Yes), N (No), and C (Can't tell).
Meta-Analysis
The articles included in this review presented significant heterogeneity related to populations, diagnoses, periods considered for evaluation of end-of-life care, and cost analyses. Therefore, it was not possible to perform a traditional meta-analysis to combine results from individual studies.
Discussion
Our study presents a systematic review with the objective of evaluating observational articles presenting the costs of end-of-life care for oncology patients. A relevant aspect identified is the predominance of studies evaluating costs in end-of-life care in the Northern Hemisphere (95.34%), with more than half of the studies (51.16%) being developed in North America. The scarcity of data in the literature on the costs of end-of-life care in low- and middle-income countries demonstrates a gap in information on the expenses involved in end-of-life cancer care in these countries. Data from the World Health Organization (WHO) highlights that in low- and middle-income countries, the most of people die without access to palliative care and with poorer quality of care. 9
In recent decades, the number of articles published on the topic of end-of-life care has increased in the main databases, our results suggest how the theme has been more explored recently, evidence that allows us to structure more consistent public policies aimed at developing end-of-life care. Although our search did not consider the entire year 2024, 17 articles (39.53%) included were published after 2020. Albeit the increase in the volume of studies is extremely positive, the heterogeneity in cost methods and on the definition of the period of end-of-life care highlights the lack of consensus and the gap in the literature. Most of the studies were from a payer perspective (74,41%) and based on macrocosting methodologies (81,39%), which limit the use of the information to evaluate variabilities in the consumption of resources. 57 The societal perspective was developed in just one study in Canada, published by Yu et al. in 2015. We did not identify this perspective in more recent studies. 29 An important piece of data presented from society’s perspective was that the average total cost of end-of-life care for all patients (death at home or in hospital) was US$34,197.73 throughout the entire palliative trajectory, which on average presented a duration of 4 months. Public health system costs represented 46.72% of total costs, and private costs represented 53.28%. 29 And the period defined as end-of-life varied across 1 month and years. It eliminates the opportunity to compare studies and cost information for similar clinical conditions.
All studies selected for analysis in this systematic review highlighted direct costs and only 9.3% analyzed indirect costs in an associated manner. The availability of consolidated data and the possibility of analyzing large databases available from Health Systems favor the performance of studies with the perspective of the payer, with analysis of direct costs. However, we know that oncological diseases have a great impact on the lives of patients and their families, 29 causing a reduction in work capacity associated with higher costs of travel for care and medication, absences from work, which are indirect costs, associated with intangible costs related to pain and suffering due to the clinical condition. Direct impacts on quality of life, with reflections and consequences for the perspective of society, and the scarcity of studies in this area identified in this Review indicate a knowledge gap.
Another aspect identified in our study is that heterogeneity was also present in the oncological diagnoses considered in the studies. Oncological diagnosis was explored in 39.53% of the studies included all types of cancer,15-31 enabling a comprehensive assessment of the costs of the different types of cancer in the population evaluated, 44.18% studies focused on one type of câncer8,33-50 that allowed the evaluation of specific interventions, Additionally, many studies had small population sizes and were limited to a single institution, 17,20,21,23,31,33,41,50 and the biggest samples were identified on the studies based on Medicare administrative data.16,28,36,37,40,42-44,48,49,53,55,56
The studies selected in this systematic review did not present uniformity in the end-of-life periods considering the time horizon, but it is possible to observe that almost 31% of the studies evaluated the last month of life, a fact that can be justified by the evidence that the greatest expenses would be involved in this period. The study by Hung et al., 25 in 2017, evaluating the last year of life, highlighted that a third of the expenses occurred in the last month of patients’ lives. Similar findings observed in the area of cancer treatment indicate a significant increase in expenses during the last weeks.15,32,33,51,54
Considering that health services use a service model focused on maximizing volume measured through productivity, the costs of end-of-life care are significant. 58 A change in approach by Palliative Care, focused on a proposal that ‘less is more’58,59 with emphasis on patient preferences and quality of life, generally promotes greater patient satisfaction, cost avoidance 60 and better care quality metrics for the patient and their family58,59,61-63 A systematic review, conducted by May et al., in 2018, demonstrated in stratified analyses that there was a reduction in costs for cancer (−$4251; 95% CI, −$4664 to −$3837; P < 0.001), these results suggest that palliative care is more effective in changing patterns of care for patients with life-threatening illnesses and that it may be possible for hospitals to reduce costs by implementing palliative care. 60
The majority of studies, 76.74%, in the review are of good quality,16,18,20,21,23-32,34-43,45-51,55,56 and 23.25% are of average quality.15,17,19,22,33,44,52-55 It is important to highlight two points in relation to the assessment of the methodological quality of the studies: criterion 7 was not possible to identify in the analysis of some articles, as the description or reference of costs in relation to the currency of the year of the study, as well as the equivalence with the dollar at the time of the research, was not identified in 20 studies (46.51%) of this review.8,15,17,19,22,23,27,28,30,33,38,42,44,46,49,50,52-55 Another significant aspect is that the design of the selected studies did not include a comparator or alternative technology, as described in criteria 2 and 8 of the checklist. As a result, only 16 studies (37.20%) carried out comparisons between conventional hospital care and palliative care, hospital care vs home care or palliative care, or the use of chemotherapy in end-of-life care vs its suspension, thus scoring these criteria.8,23,27-31,38,41,42,45-50
Limitations
New studies on the costs of end-of-life care, presenting a standardization of criteria for economic evaluations, involving a societal perspective, analyzing direct, indirect and intangible costs and also including the pediatric age group, are necessary to understand the resources and costs involved in end-of-life care for cancer patients, for structuring sustainable health policies, with better quality of life and support for patients and their families, through a care process that involves value-based health.
Conclusion
Considering the complexity of the end-of-life care period and the need for consistent data in relation to the care costs involved in this stage of life, the development of more studies, mainly in middle and low-income countries and approaches to indirect and intangible costs, with the perspective of society are of great importance for the development of public health policies and planning of health managers, in accordance with the trend of transforming value-based care, allowing the health care system to create more value for patients and their families.
We believe that future research in this area will be fundamental for the better utilization of healthcare resources. However, we believe that there is a lack of standardization in conducting these studies, such as study design, assessed costs, interval between death and the start of observation, and study perspective. This standardization would be crucial for using the data to develop international guidelines for more efficient end-of-life care.
Supplemental Material
Supplemental Material - End-of-Life Costs in Cancer Patients: A Systematic Review
Supplemental Material for End-of-Life Costs in Cancer Patients: A Systematic Review by Soraya Camargo Ito Süffert, MD, MSc, Carlos Eduardo Aliatti Mantese, MD, PhD, Felipe Rodrigo de Castro Meira, Katia Flavia Rosso de Oliveira Trindade, Ana Paula Beck da Silva Etges, Rafael José Vargas Alves MD, PhD, and Claudia Giuliano Bica, PhD in American Journal of Hospice and Palliative Medicine.
Supplemental Material
Supplemental Material - End-of-Life Costs in Cancer Patients: A Systematic Review
Supplemental Material for End-of-Life Costs in Cancer Patients: A Systematic Review by Soraya Camargo Ito Süffert, MD, MSc, Carlos Eduardo Aliatti Mantese, MD, PhD, Felipe Rodrigo de Castro Meira, Katia Flavia Rosso de Oliveira Trindade, Ana Paula Beck da Silva Etges, Rafael José Vargas Alves MD, PhD, and Claudia Giuliano Bica, PhD in American Journal of Hospice and Palliative Medicine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.