
Abstract
Objective
Palliative care (PC) utilization in cancer care has been shown to alleviate symptoms, increase goals of care discussions, and reduce invasive end of life measures. This study examined the association of inpatient PC consultation with readmission and hospitalization costs among patients with ovarian cancer.
Methods
All records for women (≥18 years) hospitalized with a diagnosis of ovarian cancer were tabulated from the 2010-2020 Nationwide Readmissions Database. Multivariable logistic, Poisson, and linear regressions were used to evaluate the association of PC consultation during index hospitalization with length of stay, rates of 30-day non-elective readmission, time to readmission, as well as overall number of readmissions and hospitalization costs.
Results
Of an estimated 285,487 patients included, 25,957 (9.0%) received a PC consultation, with an increase from 5.1 to 11.7% (P < 0.001) across the period. Factors associated with use of PC included: increasing age (AOR 1.03/yr, 95% CI 1.03-1.03, P < 0.001) and Elixhauser comorbidity index (AOR 1.19/point, 95% CI 1.17-1.21). PC was associated with lower risk adjusted rates of 30 day (11.63%, 95% CI 11.0-12.3 vs 20.25%, 95% CI 20.0-20.6) non-elective readmission (P < 0.001). The adjusted incident rate ratio of readmission after PC consultation was 0.41 [0.38-0.43], P < 0.001. Patients receiving PC additionally had less cost associated with their index hospital stay; −$2,407 [−$2,669.86- −$2,144.43], P < 0.001).
Conclusions
Inpatient PC consults appear to be associated with reduced medical readmissions for patients with ovarian cancer, as well as decreased hospital resource use, however disparities exist. Continued increase in access and early PC referral should be considered.
Keywords
Introduction
In 2024, ovarian cancer accounted for about 1% of all new cancer cases and 2.1% of all cancer deaths in the United States, with an estimated 19,710 cases diagnosed and 13,270 deaths. 1 The majority of ovarian cancer cases are diagnosed at an advanced stage, with stage IV disease carrying a 5-year survival rate of ∼30.8%. 1 Patients with ovarian cancer often present with debilitating symptoms at the time of diagnosis, during initial treatment, and at progression. 2
Integration of palliative care services is recommended in patients with a new diagnosis of advanced malignancy by multiple organizations including the American Society of Clinical Oncology, the World Health Organization (WHO) and the Society of Gynecologic Oncology.3-6 Studies show that early palliative care referrals can result in better quality of life and less aggressive interventions in patients navigating end of life care. 7 Within the field of gynecologic oncology, palliative care has been associated with improved symptom management and fewer emergency department visits.8,9 Despite these findings, palliative care continues to be underutilized, with studies showing that only 70% of patients were referred to palliative care prior to death, and more than 80% of those patients referred within 30 days of death.10-12
While many studies have evaluated the utilization of palliative care and its effect on patient symptoms, few studies have examined the association of palliative care consultation on hospital systems, which has important implications. The objective of this study was to describe the association between inpatient palliative care consultations and readmission rates in patients with ovarian cancer.
Methods
This was a retrospective cohort study of all inpatient hospitalizations in the United States among patients with a diagnosis of ovarian cancer from 2010 to 2020 using the Nationwide Readmissions Database. 13 Maintained as part of the Healthcare Cost and Utilization Project, the Nationwide Readmissions Database is a federal, state, and industry partnership that contains 17 million discharges encompassing 57% of U.S. hospitalizations. The Nationwide Readmissions Database utilizes a 2-stage cluster design to post-stratify by hospital (census region, urban/rural location, teaching status, and bed size) and patient (sex and age) characteristics, weighting certain patients more than others to best represent the US population. The resulting individual discharge weights were utilized to generate national estimates for approximately 36 million hospital discharges annually.
All adult (≥18 years) records for women with ovarian cancer were queried from the 2010-2020 Nationwide Readmissions Database using International Classification of Disease, 9th and 10th Revision (ICD-9 and 10) codes. 14 Palliative medicine consultations were identified using ICD-9 and 10 codes for palliative care consultation which has a sensitivity of 49% and specificity of 99% as described in previous studies.15,16 Patients without data for age, in-hospital costs, or elective status were excluded. Additionally, women who underwent surgery during their index admission were excluded, to minimize confounding factors related to perioperative morbidity and costs. Patients who did not survive to discharge were also excluded as described in previous studies to reduce bias in readmission rates. 15 As the Nationwide Readmissions Database contains only longitudinal data for patients within each calendar year, only patients with index hospitalization within the first 9 months of each calendar year were included to allow for adequate 90 day follow-up.
Patient and hospital characteristics including age, insurance status, income level, and hospital type were defined using the Healthcare Cost and Utilization Project data dictionary. 13 Major adverse events were defined as a composite of cardiac complications, pneumonia, venous thromboembolism, wound dehiscence, and sepsis, identified by ICD-9 or 10 codes. The Elixhauser Comorbidity Index, a previously validated composite score of 30 common comorbidities, was utilized as an additional measure of patient medical complexity. 17 Hospital costs were calculated using the center specific cost to charge ratios to the total hospitalization cost and subsequently adjusted for inflation. 13 Non-elective readmissions were captured using a variable inherent to the database which defines each hospitalization as elective/planned or non-elective/unplanned. Elective admissions were considered planned or scheduled admissions for procedures, while non-elective admissions were for individuals admitted to the hospital under emergent conditions. 13 The primary outcomes of this study were the rate of palliative care consultation and rates of 30- and 90-day readmission.
Categorical variables were analyzed using Pearson’s Chi-square test. Continuous variables are reported as means with standard deviation and were compared using the Adjusted Wald test. Demographic, clinical, and operative factors were selected for inclusion in regression models through application of least absolute shrinkage and selection operator (LASSO) regularization. 18 Poisson, and linear regressions were used to evaluate the independent association of palliative care consultation on index hospitalization with length of stay, rates of 30-day non-elective readmission, frequency of readmission, and total hospitalization costs. Regression results are reported as adjusted incidence rate ratios, adjusted odds ratios, or beta coefficients with a 95% confidence interval. The Cochrane-Armitage test was used to evaluate for trend. In all comparisons, P < 0.05 was considered statistically significant. All statistical analyses were performed using STATA 14.2 (StataCorp LP, College Station, Texas). The study was deemed approved for exempt status by the Institutional Review Board at the University of California, Los Angeles (IRB #17-001112). STROBE reporting guidelines were followed for this cohort study. 19
Results
Characteristics of Patients Receiving Palliative Care Consultation.
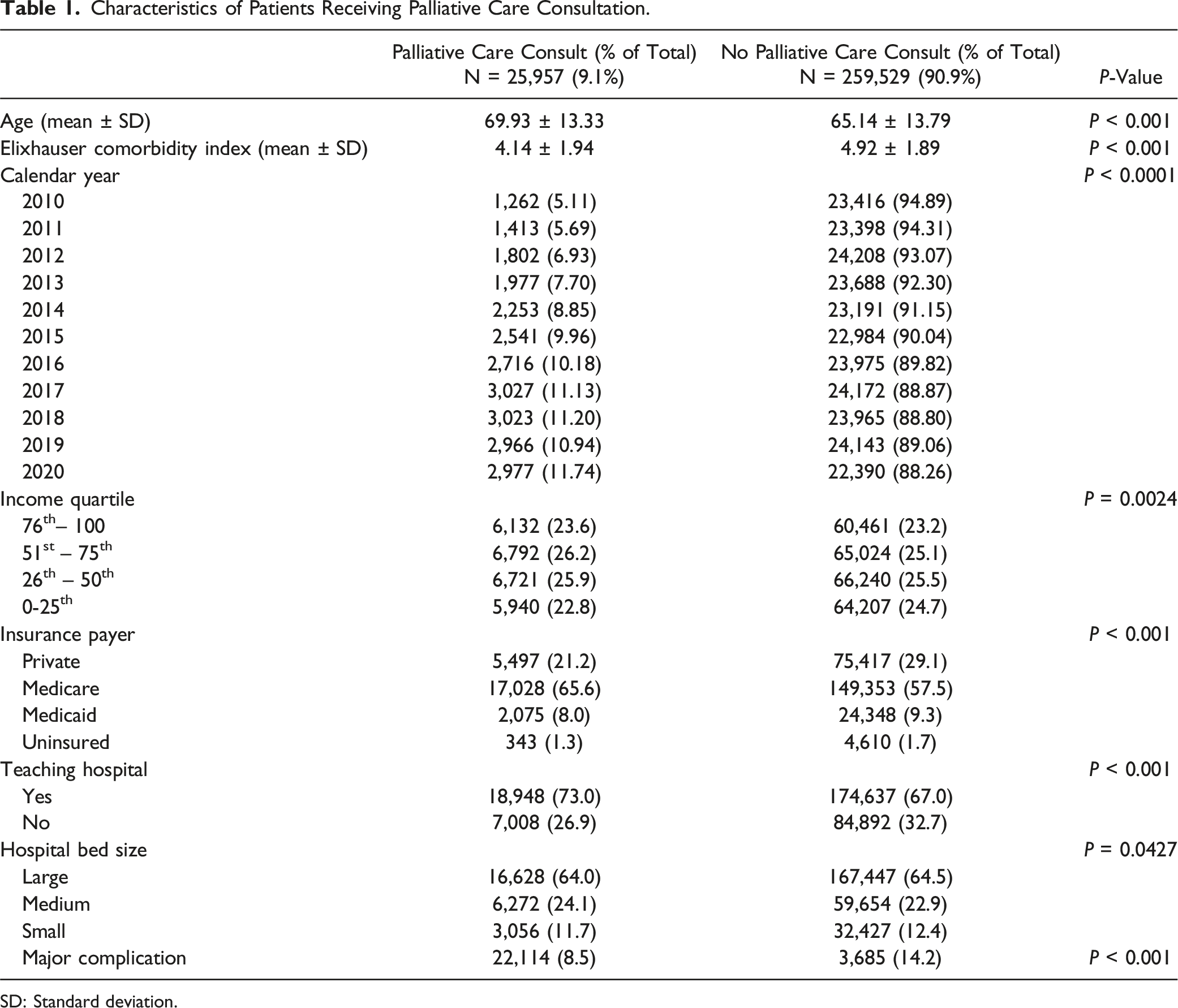
SD: Standard deviation.
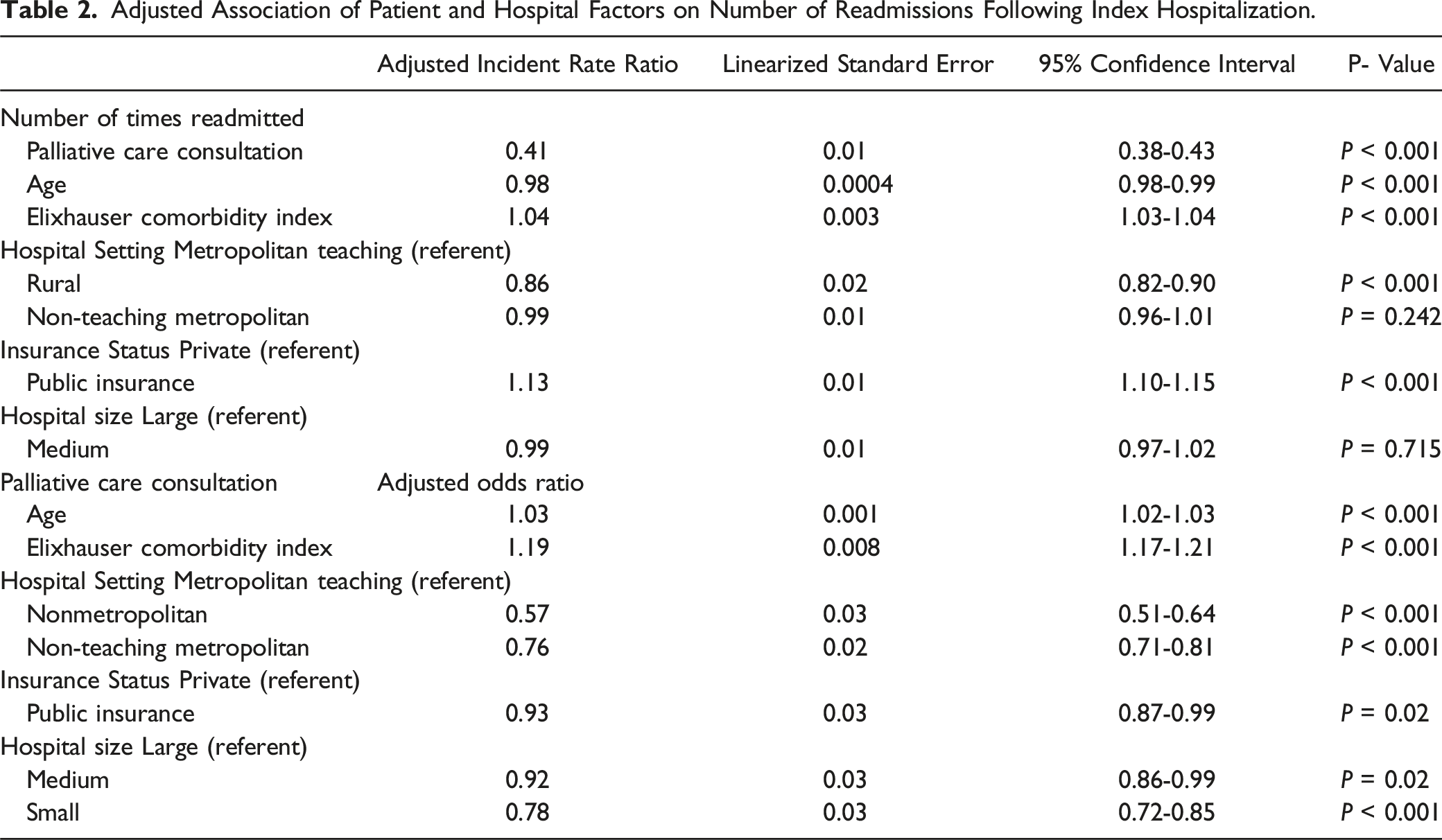
Adjusted Association of Patient and Hospital Factors on Number of Readmissions Following Index Hospitalization.
Adjusted Patient Outcomes and Hospital Resource Utilization, by Palliative Care Consult Status.

SD: Standard deviation; CI: confidence interval.
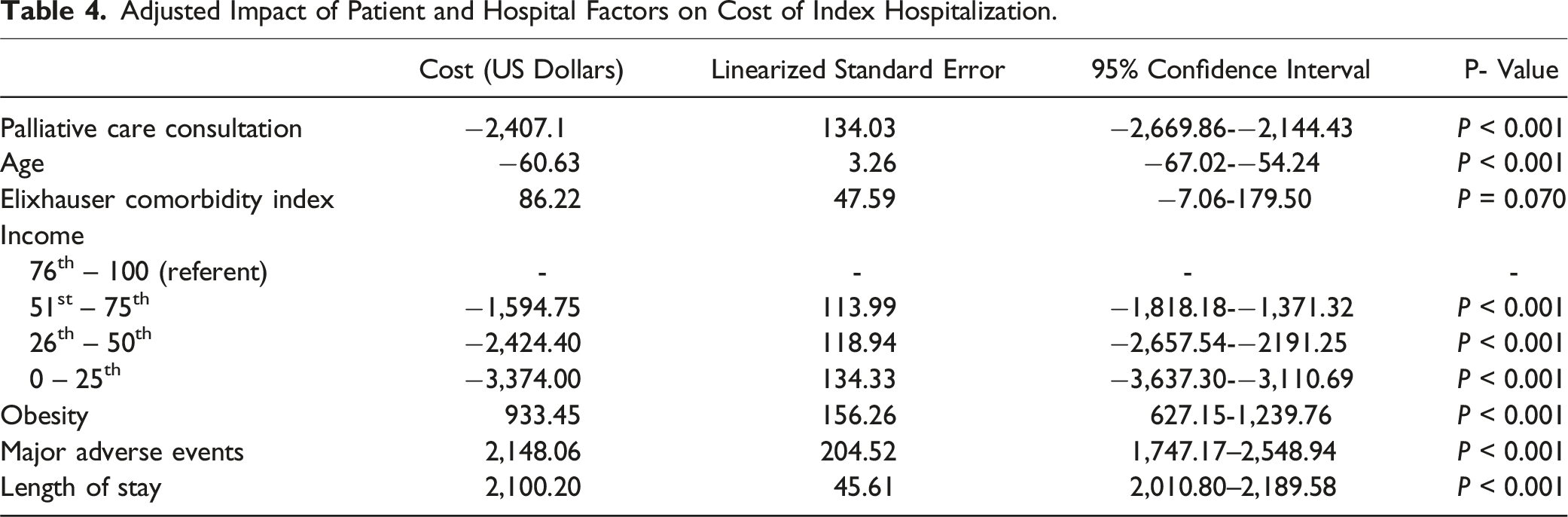
Upon multivariable regression adjusting for patient and hospital factors, palliative care consultation at index hospitalization was independently associated fewer number of readmissions in the 90-day follow-up period (adjusted incident rate ratio (aIRR) 0.41 [0.39-0.43, P < 0.001) (Figure 1). Older age was associated with a decreased rate of readmission, while increasing medical complexity was associated with an increased risk of readmission after adjustment (aIRR 0.98 [0.98-0.99], P < 0.0001 and aIRR 1.04 [1.03-1.04], P < 0.001. Patients with public insurance were more likely to have a subsequent readmission compared to private insurance (aIRR 1.13 [1.10-1.15], P < 0.001). Patients receiving care at more rural locations were less likely to be readmitted compared to patients at metropolitan hospitals. There was no difference on readmission rates based on the size of the hospital (Table 2). Patients with a palliative care consultation additionally had fewer costs associated with their index hospital stay; adjusted beta coefficient -$2,407 [−$2,669.86-−$2,144.43], P < 0.001). Increased cost of hospitalization was associated with the occurrence of major adverse events, increasing length of stay, and in patients with obesity (Table 4). Adjusted incident rate ratio of hospital readmission after palliative care consultation for women with an ovarian cancer diagnosis. Adjusted Impact of Patient and Hospital Factors on Cost of Index Hospitalization.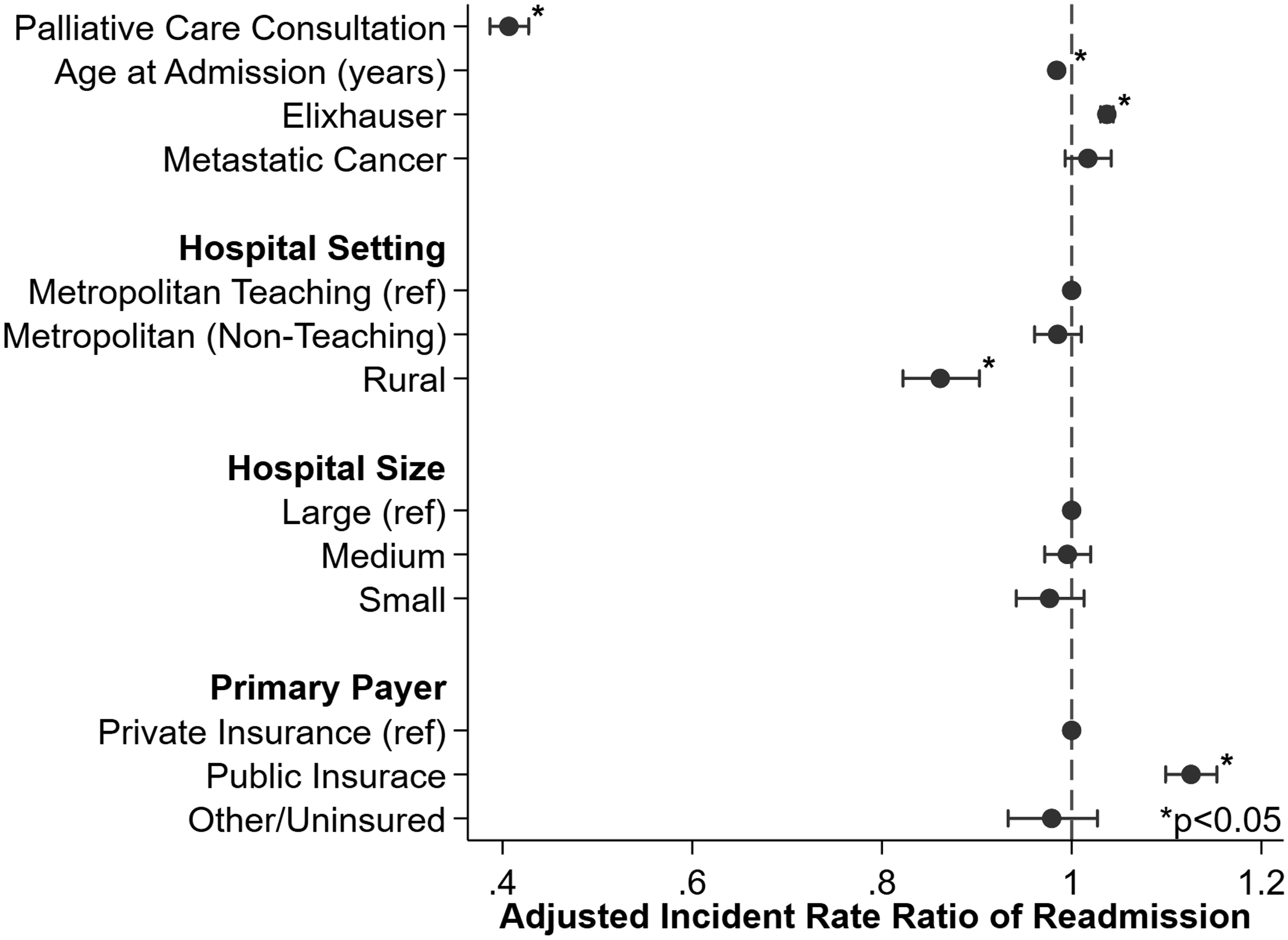
Discussion
Summary of Main Results
Cancer is the second most common cause of death in the United States after heart disease. 20 Palliative care services are important in providing symptom relief and comprehensive care to patients with cancer, with research demonstrating significant improvement in symptoms, quality of life, and initiation of conversations regarding goals of care. This study found that ovarian cancer patients who had an inpatient palliative care consultation had lower rates of unplanned 30- and 90-day readmission compared to patients who did not. Following adjustment for patient and hospital factors, palliative care was also associated with lower cost of index admission. Additionally, we identified disparities among patients who did and did not receive a consultation with palliative care. Few studies have looked at the association of palliative care utilization in gynecologic cancer patients with respect to hospital systems or cost.
Results in the Context of Published Literature
Palliative care utilization in patients with cancer has been studied from many perspectives. While palliative care has been shown to have a positive impact on end-of-life care in gynecologic cancer patients, many studies demonstrate that not enough patients are being appropriately referred to see palliative care specialists, or are getting referred late in their disease course, contrary to governing body recommendations.3-6,9,12,21 Our study is consistent with prior findings in this area; among our cohort of 285,456 women, only 9.1% had a palliative care referral. Other studies report anywhere from a 4% to 58% rate of referral to palliative care while in the inpatient setting.12,22 In general, most women admitted with a diagnosis of ovarian cancer excluding surgical hospitalization will have advanced disease. The majority of these women would likely benefit from palliative care consultation. Rates of consultation to palliative care increased from 5.11% in 2010 to 11.74% in 2020 in our study. Other studies have reported similar trends, likely due to increasing availability of palliative care services in United States hospitals.22,23 This demonstrates a promising trend of increasing incorporation of multimodal care in complex cancer patients, but more work is needed to further increase palliative care utilization and to decrease the disparities in its access. Our study identifies that patients with public or government-funded insurance, and those receiving care at non-metropolitan or metropolitan non-teaching hospitals, less frequently receive a palliative care consultation. This is likely multifactorial and could be due to lack of palliative care resources in these settings. These findings represent a potential area for improvement in creating equitable access to palliative care consultation on both a patient and hospital level. Further, patients with increased comorbidities and higher Elixhauser scores had higher rates of palliative care consultations, potentially identifying a group of patients with highest need for palliative medicine services. It is important to consider that older patients and patient with more comorbidities may have been referred to palliative care to discuss hospice enrollment which would impact the readmission rates seen in this population.
This study also focuses on the association between palliative care services and the burden on the health care system. 30-day readmission rates are a key quality metric at many hospitals and with many insurance payers. 24 There are few studies looking at the impact of palliative care specifically on readmission for ovarian or gynecologic cancer, but some have examined its relationship with other malignancies or chronic diseases. Results in other studies are conflicting, with some studies showing no change in readmission rates and others showing decreased readmission rate.25-30 These differences seen could be due to physiologic differences in disease processes as some studies looked at palliative care and readmissions in conditions such as congestive heart and liver failure. Our study found that patients who had an inpatient palliative care consultation had overall lower 30- and 90-day readmission rates despite older age and high comorbidity index in this population. While our finding is clearly limited by the inability in the Nationwide Readmissions Database to track patient outcomes and mortality that occur outside of the hospital setting, we posit that our finding of decreased readmission rates is potentially related to increased ability to manage symptoms related to the patient’s ovarian malignancy as an outpatient, preventing the need to come into the hospital. Additionally, as palliative care can often help with goals of care discussions, patients receiving palliative care consultation may opt for more conservative treatment options such as hospice, which would affect readmission rates. This is consistent with several studies demonstrating that incorporation of palliative care reduces the rate of interventions and invasive procedures, while increasing the rate of hospice initiation at the end of life.9,31 These findings demonstrate a need and benefit of increased early involvement of palliative care services in order to improve patient outcomes as well as hospital metrics.
Implications for Practice and Future Research
The rising cost of medical care is a large consideration for health care systems. Previous studies have shown palliative care consultation to be associated with lower cost in the setting of decreasing high resource care at the end of life and early initiation of hospice.32-34 A study examining cost associated with end-of-life care in patients with ovarian cancer found that hospital admissions accounted for more than 50% of the average $24,073 costs in the last 90 days of life. 35 Our study demonstrated palliative care was associated with decreased index cost and subsequent readmission rate, a significant driver of health care cost at the end of life. Cost data was limited as it was indirectly determined from the hospital system cost-to-charge ratio. Based on the above literature, palliative care consultations could have cost-saving impacts on the United States health care system, while simultaneously improving symptom management and end of life care delivery to patients. This needs further exploration in larger, prospective studies.
Strengths and Weaknesses
This study has several limitations. The Nationwide Readmissions Database is a large database that is subject to errors in coding that may affect results. The database can only track readmissions for a single patient over 1 calendar year which limits the timeline of our study. Additionally, the Nationwide Readmissions Database is limited in that it does not include outpatient data, thus out-of-hospital mortality, costs, and changes in trends of outpatient palliative care referrals are not included in the data set and may confound readmissions data. Since we are unable to follow patients in the outpatient setting or identify the timing of the referral in the patient’s disease course, we are unable to determine how many patients with inpatient palliative care consultations were referred to hospice, and as a result, avoided readmissions and incurred lower costs. The Nationwide Readmissions Database does not have comprehensive data on patient race and ethnicity although disparities in the receipt of palliative care consultations have been previously documented.36,37 Additionally, this study included the calendar year 2020, and the COVID-19 pandemic may have affected the results from this year. This study has several strengths. The Nationwide Readmissions Database is the largest nationwide database that tracks readmissions which provides strong power and generalizability for our study. Many studies looking at palliative care referrals or outcomes are retrospective, single institution studies which can be less widely applicable. Large sample size can help detect disparities or trends that may not be easily identified in smaller studies.
Conclusions
In addition to quality of life and symptom improvements, palliative care consultation for patients with ovarian cancer is associated with decreased readmission rates and reduced hospital cost. The rate of inpatient palliative care consultation increased over the study period, however disparities in its utilization continue to exist on the patient and hospital level. This study raises a cost effectiveness and systems-based argument for more widespread use of palliative care in the ovarian cancer population and identifies patient populations and hospitals in which its use could be further implemented. Additional studies are merited to examine whether the same findings persist in other cancer populations and to develop effective methods for increasing implementation of palliative care consultation to decrease the disparities that exist.
Supplemental Material
Supplemental Material - Association of Palliative Care With Readmission and Resource Utilization in Patients With Ovarian Cancer: A National Perspective
Supplemental Material for Association of Palliative Care With Readmission and Resource Utilization in Patients With Ovarian Cancer: A National Perspective by Alex A. Francoeur, Nikhil Chervu, Alexandra L. Mardock, Samantha Solaru, Sara Sakowitz, Peyman Benharash, and Tiffany S. Lai in American Journal of Hospice and Palliative Medicine
Footnotes
Author’s Note
This work was previously presented as a poster at the Society of Gynecologic Oncology Annual meeting in Tampa, Florida, 2023.
Author Contributions
Alex. A Francoeur: Conceptualization; methodology; writing original draft; visualization. Nikhil Chervu: Methodology; formal analysis; software. Alexandra L. Mardock: Conceptualization; methodology; writing review and editing. Samantha Solaru: Writing review and editing. Sara Sakowitz: Formal analysis; software. Peyman Benharash: Resources; data curation; supervision. Tiffany S. Lai: Conceptualization; methodology; supervision; writing review and editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.