
Abstract
Objectives: To investigate the current state of primary palliative care practice in Japanese critical care settings, identify care perceived as equivalent to primary palliative care, and explore the barriers. Methods: We employed a quantitative descriptive questionnaire survey with a nationwide cross-sectional design involving 740 critical care specialist nurses. Results: Questionnaires were received from 384 nurses, yielding a response rate of 51.9%. Nurses recognized typical palliative care provided to cancer patients, such as “relieving suffering at end-of-life” (95.3%), “pain management” (88.8%), and “caring for patients’ psychological suffering” (88.3%), as primary palliative care in the critical care setting. They also recognized “monitoring and management of delirium” (68.5%), “caring for patients’ social suffering” (63.5%), and “preventing post-intensive care syndromes” (61.7%) less frequently as aspects of primary palliative care in critical care settings. Additionally, the recognition was lower among emergency department nurses than intensive care unit nurses. The nurses recognized inadequate overall palliative care practices, especially regarding patients’ social (72.1%) and spiritual (76.8%) suffering. They recognized “insufficient knowledge and skills among critical care medical staff” (70.6%) and “unable to confirm the patients’ preferences to treatment goals” (54.4%) as barriers to providing primary palliative care. The barriers that nurses recognized less often were “uncertainty about palliative care in critical care settings” (6.8%) and “disagreements among nursing teams regarding providing palliative care” (8.3%). Conclusion: Specialist nurses understood palliative care but felt unprepared in primary palliative care due to limited knowledge. Improved education in primary palliative care and patient-family communication is needed in Japan’s critical care settings.
Introduction
Palliative care has traditionally been provided primarily to patients with cancer, especially those in the terminal stage, 1 but its scope has expanded to include a wider range of diseases and disease stages. 2 In 2022, the World Health Organization (WHO) has indicated that palliative care should be provided to patients in critical care settings, such as intensive care units (ICUs) and emergency departments (EDs), 3 including those with coronary artery disease, major organ failure, severe burns, acute trauma, and other representative diseases. Even patients and families receiving aggressive treatment in critical care settings require appropriate palliative care if they experience suffering. 4
Palliative care is broadly divided into primary palliative care and specialized palliative care. Primary palliative care generally focuses on managing symptoms such as pain, depression, and anxiety, as well as discussing prognosis, treatment goals, suffering, and code status. 5 This type of care is more commonly provided by bedside nurses than specialized palliative care. 6 Several nurse-targeted surveys regarding palliative care in critical care have been conducted in Japan. For example, Kinoshita et al 7 reported that many nurses believed that the ICU was not a suitable place for death. Additionally, Tatsuno et al 8 reported that nurses in the critical care field found it difficult to provide palliative care at the end of life, feeling that “the patient’s suffering is difficult to grasp,” and “there are differences in recognition and values between physicians and nurses.” However, these surveys were limited to the end-of-life period and did not address the overall status of palliative care. They indicated various difficulties, barriers, and a lack of knowledge that critical care nurses face when practicing end-of-life care. These data suggest the possibility that high-quality end-of-life care, and consequently, palliative care, may not be provided in Japan.
In response to this situation, Japan launched the End-of-Life Nursing Education Consortium-Japan Critical Care, led by certified and specialized nurses, in 2014. By 2021, the program had attracted 1550 nurse participants and 420 instructors. 9 Additionally, in 2019, the Japan Critical Care Nursing Society and the Emergency Nursing Society, composed of certified and specialized nurses, created and disseminated the “End-of-Life Nursing Practice Guide in Emergency and Intensive Care” to promote awareness and education. In Japan, certified and specialized nurses respond to consultations regarding the care of critically ill patients through multidisciplinary team activities such as the Respiratory Support Team, and contribute to the advancement of critical care nursing in general.10,11
Given the significant differences in patient populations and operational systems between the ED and the ICU in Japan, it is necessary to determine whether there are differences in the practice, recognition, and barriers to primary palliative care between these two settings. Furthermore, targeting certified and specialized nurses would be appropriate. We examine the current state of primary palliative care practice in critical care settings, identify care perceived as equivalent to primary palliative care, and explore the barriers associated with its practice in Japan.
Methods
Ethical Consideration
This study was approved by the institutional review boards of Tohoku University (No. 2020-1-550) and Shinshu University (4798) and was conducted according to the tenets of the Declaration of Helsinki. Participation in the study was considered as consent when the completed questionnaire was returned, with a mark indicating agreement to participate.
Study Design
This was a quantitative descriptive study utilizing a nationwide, cross-sectional, anonymous, self-administered questionnaire survey conducted from October 2020 to December 2020. To enhance response rates, questionnaires were sent twice to all selected nurses, with the second distribution including a ballpoint pen as an incentive and sent one month after the initial distribution. The study design is shown in Figure 1. Study flowchart.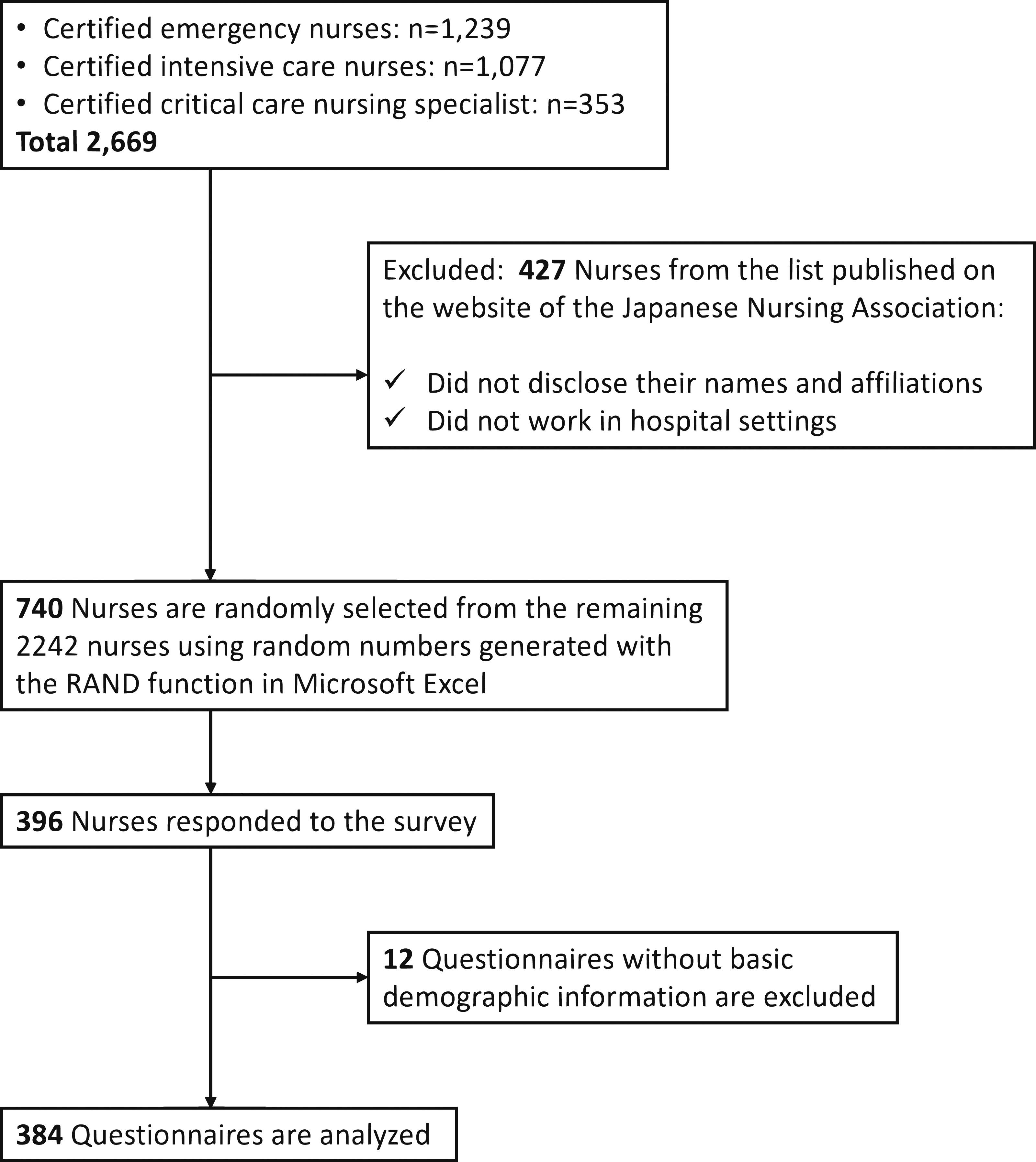
Participants
Critical care specialist nurses were surveyed. In Japan, critical care specialist nurses are classified into three certification types: Certified Emergency Nurse (CEN), Certified Intensive Care Nurse (CIN), and Certified Critical Care Nursing Specialist (CCNS). CENs and CINs receive training in specific areas of critical care, acquiring advanced nursing skills and knowledge through 6 months of education at accredited facilities. In contrast, CCNSs pursue advanced education, typically at the master’s level, to deepen critical care nursing, and this enables them to provide high-level care to individuals, families, and groups with complex and challenging nursing issues. 12 Nurses whose names and institutions could not be identified on the Japanese Nursing Association website were excluded from the survey, as it was conducted via mailed questionnaires. Additionally, specialist nurses not currently employed in hospital facilities were also excluded to clearly elucidate the current status of primary palliative care.
The target sample size was calculated using G*Power Ver 3.1 with the following parameters: a population of 2669 nurses (certified emergency nurses: 1239; certified intensive care nurses: 1077; and certified critical care nursing specialists: 353), an α error probability of 0.05, a power of 0.95 (Z score 1.96), and P = 0.5. A total of 336 specialist nurses were needed. A previous study 13 suggested estimating a response ratio of 0.45. Therefore, from the 2669 nurses listed on the website (accessed on June 1, 2020), 427 nurses without a name or institution and those not working in hospital settings were excluded, resulting in a final population of 2242 nurses. Overall, 740 specialist nurses were randomly selected from the remaining population.
Measurements
The questionnaire was developed based on previous studies14-16 and underwent discussion and pilot testing with five specialists, including a palliative care physician, an intensivist, an emergency physician, a certified critical care nursing specialist, and a researcher, recruited using snowball sampling. In the pilot test, specialists provided feedback on the questionnaire items using clinical sensitivity ratings (1 = invalid, 2 = somewhat invalid, 3 = somewhat valid, and 4 = valid). Items rated 1 or 2 were modified by the researchers. Finally, these specialists were offered the opportunity to recheck clinical sensitivity, and all items were rated 3 or 4, resulting in the final version of the questionnaire.
Nurses’ Recognition of Palliative Care in Critical Care Settings
Participants were asked to indicate their degree of agreement with 13 aspects of care related to palliative care in critical care settings, using a scale score ranging from 1 to 6: 1 = strongly disagree, 2 = disagree, 3 = somewhat disagree, 4 = somewhat agree, 5 = agree, 6 = strongly agree. The 13 aspects were as follows: “relieving suffering at the end of life,” “pain management,” “caring for patients’ psychological suffering,” “providing psychological support for the family,” “supporting patient and family decision-making,” “caring for patients’ spiritual suffering,” “reconciling ethical issues,” “treatment and care for physical symptoms other than pain,” “withholding/withdrawing intensive treatment when the patient is suffering,” “sedation management,” “monitoring and management of delirium,” “caring for patients’ social suffering,” and “preventing post-intensive care syndromes (PICS).”
Current Status of Primary Palliative Care in Critical Care Settings
Participants were asked to indicate their degree of agreement with the statement “Is the suffering of patients adequately addressed in the intensive care unit (ICU)/Emergency Department (ED)?” for physical, psychological, social, and spiritual suffering on a scale ranging from 1 to 6: 1 = strongly disagree, 2 = disagree, 3 = somewhat disagree, 4 = somewhat agree, 5 = agree, and 6 = strongly agree.
Barriers to Primary Palliative Care in Critical Care Settings
Participants indicated their recognition of barriers to primary palliative care in critical care settings using the following 10 multiple-answer items: “insufficient knowledge and skills among ICU/ED medical staff regarding palliative care,” “often unable to confirm the patient’s preferences when determining treatment goals,” “difficulty in breaking ‘bad news’ to patients and families,” “insufficient time to interact with patients and families to provide palliative care,” “disagreement between physicians and nurses about palliative care,” “disagreement among physician team about palliative care,” “difficulty in predicting and assessing end-of-life prognosis,” “legal concerns regarding the discontinuation of life-sustaining treatment even when it is deemed to cause the patient suffering,” “disagreement among nursing teams regarding providing palliative care,” and “uncertainty about definition of palliative care in the critical care settings.”
Participant Background
The participants’ sociodemographic background, including sex, age, years of experience in nursing and critical care nursing, position title, type of critical care setting (ED or ICU), and number of hospital beds were included. Additionally, the experience of consultation with the palliative care team, experience of education and/or training regarding palliative care, and the degree of knowledge of the WHO’s palliative care definition; Palliative care is an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial, and spiritual, 17 were assessed according to four levels: known, somewhat known, somewhat unknown, and unknown.
Statistical Analysis
Categorical variables (sex, position title, number of hospital beds, consultation experience for palliative care team, experience with palliative care education, knowledge of the WHO palliative care definition, and barriers to primary palliative care) were presented as frequencies and percentages and compared between ED nurses and ICU nurses using the chi-squared test. Meanwhile, continuous variables (nurses’ age, years of nursing experience, years of emergency nursing experience, nurses’ recognition of primary palliative care, and current status of primary palliative care) were summarized as means and standard deviations (SD). The normality of their distribution was assessed using the Shapiro-Wilk test and graphical methods. Subsequently, continuous variables were compared between ED and ICU nurses using the t-test or Welch’s test. Furthermore, the effect size (ES) of categorical variables were evaluated by calculating Cramer’s V, with values <0.3, 0.3-0.5, and >0.5 indicating small, moderate, and large ES. All statistical analyses were conducted using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan) with a two-tailed approach. Statistical significance was defined as P < .05.
Results
Demographic and Institutional Characteristics
Participant Characteristics (n = 384).
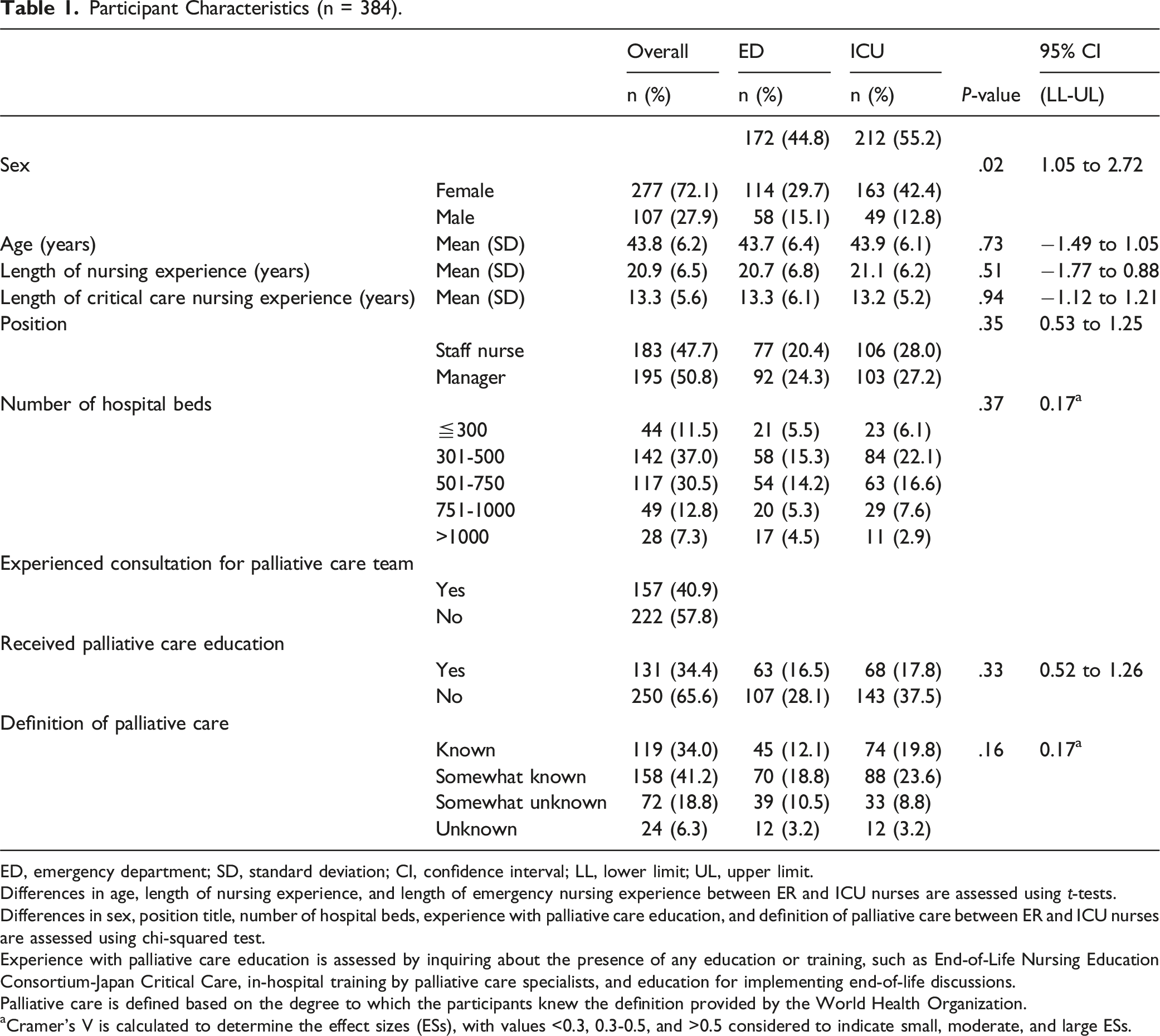
ED, emergency department; SD, standard deviation; CI, confidence interval; LL, lower limit; UL, upper limit.
Differences in age, length of nursing experience, and length of emergency nursing experience between ER and ICU nurses are assessed using t-tests.
Differences in sex, position title, number of hospital beds, experience with palliative care education, and definition of palliative care between ER and ICU nurses are assessed using chi-squared test.
Experience with palliative care education is assessed by inquiring about the presence of any education or training, such as End-of-Life Nursing Education Consortium-Japan Critical Care, in-hospital training by palliative care specialists, and education for implementing end-of-life discussions.
Palliative care is defined based on the degree to which the participants knew the definition provided by the World Health Organization.
aCramer’s V is calculated to determine the effect sizes (ESs), with values <0.3, 0.3-0.5, and >0.5 considered to indicate small, moderate, and large ESs.
Nurses’ Recognition of Palliative Care in Critical Care Settings
Figure 2 presents the symptoms and situations that nurses recognized as pertaining to palliative care in the critical care setting. More than eight-tenths of the nurses responded with “strongly agree” or “agree” to the following symptoms and situations: “relieving suffering at end-of-life” (95.3%), “pain management” (88.8%), “caring for patients’ psychological suffering” (88.3%), “psychological support for family” (83.1%), “caring for patients’ spiritual suffering” (81.6%), “reconciling ethical problems” (80.7%), and “treatment and care for physical symptoms other than pain” (80.5%). Meanwhile, approximately 60% of the nurses responded with “strongly agree” or “agree” to the following items: “monitoring and management of delirium” (68.8%), “sedation management” (68.5%), “caring for patients’ social suffering” (63.5%), and “preventing PICS” (61.7%). There were significant differences between ED nurses and ICU nurses regarding the recognition for “pain management” (P = 0.01, 95% CI: −0.42–-0.05), “caring for patients’ psychological suffering” (P = 0.02, 95% CI: −0.43–-0.05), and “caring for patients’ spiritual suffering” (P < 0.01, 95% CI: −0.43–-0.08). The ICU nurses’ scores on these five items were higher than those of ED nurses. Nurses’ perception of palliative care in critical care settings (n = 384). Notes: Each item is rated on a 6-point scale: 1 = strongly disagree, 2 = disagree, 3 = somewhat disagree, 4 = somewhat agree, 5 = agree, and 6 = strongly agree.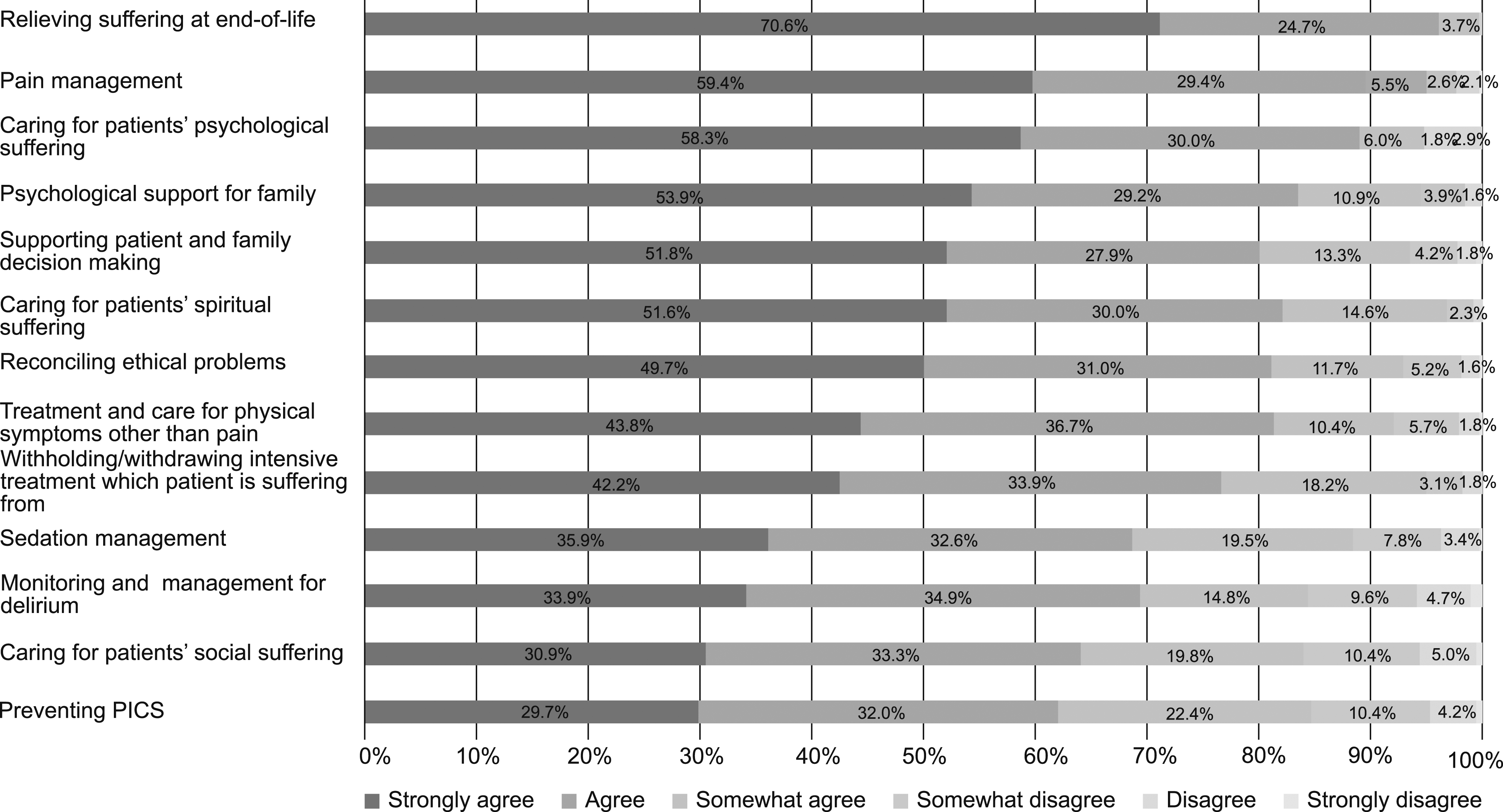
Current Status of Primary Palliative Care in Critical Care Settings
The nurses’ evaluations of the status of palliative care in critical care settings are shown in Figure 3. Nurses who strongly agreed or agreed that patients’ physical suffering is being appropriately provided for accounted for 1.8% and 15.6%, respectively. Regarding patients’ social and spiritual suffering, <10% of the nurses strongly agreed or agreed that it was adequately addressed (6.0% and 4.2%, respectively). Furthermore, there were no significant differences in the status of the four aspects of primary palliative care between ED and ICU nurses. Nurses’ evaluation of current provision of palliative care in the ICU/ER (n = 384). Note. Each item is rated on a 6-point scale: 1 = strongly disagree, 2 = disagree, 3 = somewhat disagree, 4 = somewhat agree, 5 = agree, and 6 = strongly agree.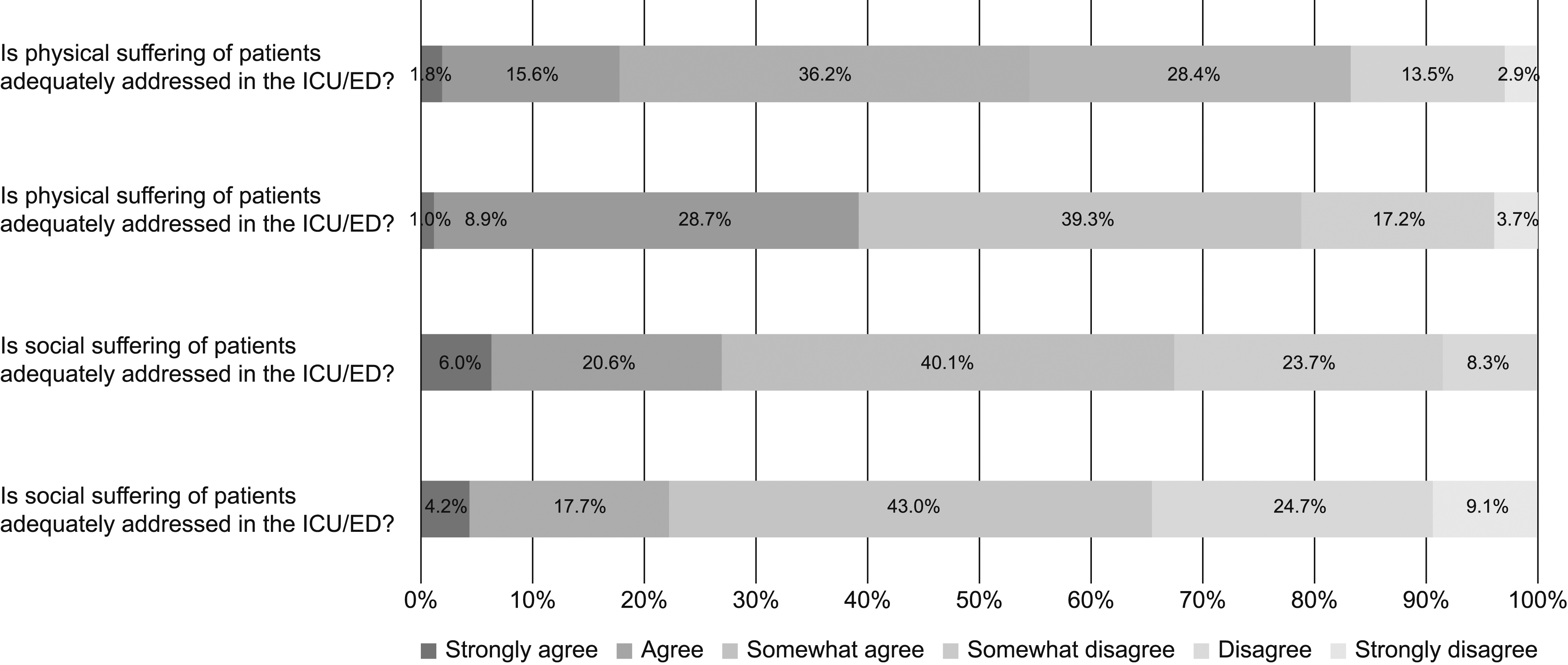
Barriers to Primary Palliative Care in Critical Care Settings
Figure 4 illustrates the barriers that nurses perceived in providing palliative care in critical care settings. More than half of the nurses’ recognized “insufficient knowledge and skills among ICU/ED staff regarding palliative care” (70.6%) and “often unable to confirm the patient’s preferences when determining treatment goals” (54.8%) as barriers to primary palliative care in critical care settings. In contrast, <10% of nurses identified “disagreement among nursing teams regarding providing palliative care” (8.3%), and “uncertainty about the definition of palliative care in the critical care settings” (6.8%) as barriers. There were no significant differences between ED and ICU nurses in their recognition of these barriers to primary palliative care. Barriers to recognition of primary palliative care among nurses (n = 384). Note. Multiple responses are obtained. The percentage indicates the proportion of nurses who respond, agree, and are asked to answer all items with which they agreed.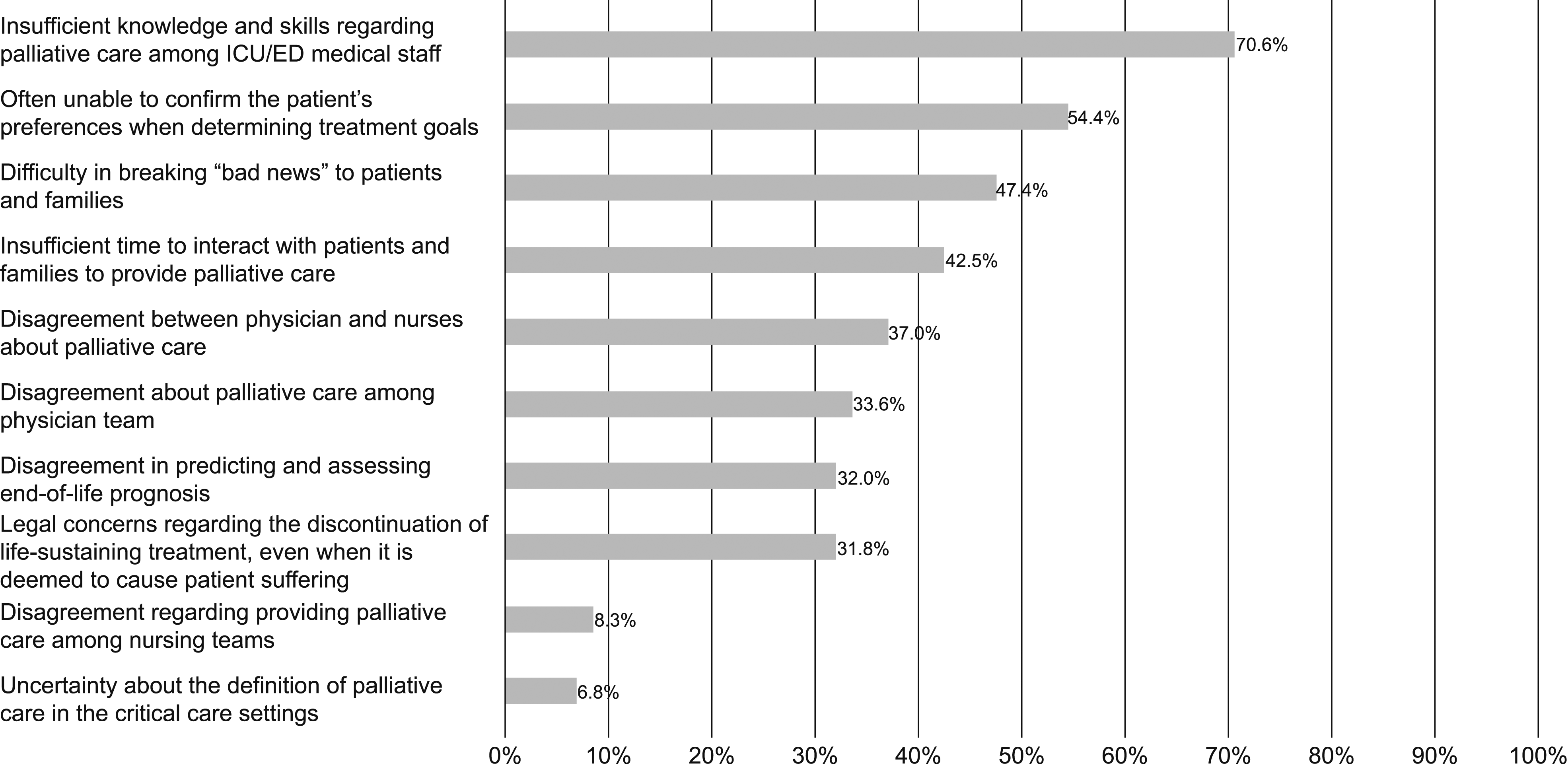
Discussion
Three main findings were observed in the current study. First, critical care specialist nurses recognized that the typical palliative care provided to cancer patients or patients with chronic illnesses was also considered palliative care. However, recognition level of ED nurses was lower than that of ICU nurses. Second, ED and ICU nurses recognized, with no significant differences, the insufficient practice of primary palliative care in critical care settings in Japan, particularly noting the lack of care for patients’ social and spiritual suffering. Third, specialist nurses perceived various barriers to practicing primary palliative care, and these were particularly related to healthcare providers’ insufficient knowledge and skills in palliative care, as well as uncertainty regarding patients’ preferences for treatment plans, with no significant difference in perception between the ED and ICU nurses. To our knowledge, this study is the first to describe the recognition, practices, and barriers to current primary palliative care among critical care specialist nurses in Japan. The findings can be used to develop suitable educational programs and/or implementation systems appropriate for providing palliative care in the EDs and ICUs in Japan.
Most specialist nurses recognize primary palliative care in the critical care setting is generally acknowledged as required in patients with cancer or chronic illness. In Japan, comprehensive efforts under the National Cancer Control Act have been underway since 2007, leading to the dissemination of the concept of palliative care for cancer and the development of undergraduate education. 18 Many nurses acquired basic knowledge of palliative care during their undergraduate education. However, in this study, only approximately 30% of these nurses had received education in palliative care after their undergraduate programs, suggesting that education in palliative care in critical care is insufficient and that nurses may respond to the suffering of patients receiving critical care based on their knowledge of basic palliative care.
Particularly, approximately 60% of respondents answered “strongly agree” or “agree” regarding symptoms specific to critical care, such as “preventing PICS” and “monitoring and management for delirium.” This indicated that specialist nurses had insufficient awareness regarding the necessity of primary palliative care in the critical care setting. PICS prevention and delirium monitoring are essential as part of the ICU Liberation approach aimed at “improving the quality of life of ICU patients” worldwide. 19 This monitoring not only promotes recovery, but also provides palliative relief. Additionally, several patient and family characteristics underline the need for palliative care in critical care settings, including decreased communication ability,20,21 short time from admission to death,22,23 and uncertain prognosis or high incidence of unexpected deaths.24,25
Therefore, specialist nurses may need to make greater use of palliative care learning programs focused on critical care settings, such as the End-of-Life Nursing Education Consortium-Japan Critical Care, than they currently do. Furthermore, because ED visits are common among patients with cancer or chronic illness suffering pain in end-of-life,26,27 ED nurses routinely provide care to these patients. Hence, it may be more difficult for ED nurses to clarify whether practicing care is primary palliative or general critical care. Educational efforts should promote the understanding among ED nurses that daily care incorporates aspects of palliative care.
More than 30% of specialist nurses reported insufficient palliative care practices of critical care medical staff. Previous studies have reported that ICU nurses find it difficult to provide care for social and spiritual aspects.28,29 In this study, specialist nurses found care for these aspects difficult and reported that care for physical and psychological aspects was insufficient. Over half of them acknowledged the overall inadequacy of palliative care practices. In the report by Igarashi et al, 30 75% of supervising ICU physicians reported not holding interdisciplinary conferences on palliative care, even monthly, suggesting that nurses and medical professionals in the critical care field may not be able to provide adequate palliative care. Primary palliative care is a team effort involving various professionals including nurses 31 Therefore, although education for nurses is important, opportunities for palliative care education for medical professionals involved in critical care are also necessary.
More than 50% of specialist nurses identified knowledge and skill deficits among medical professionals in primary palliative care practice, as well as uncertainty in patient preferences when deciding on treatment goals, as barriers to providing palliative care. Regarding the former, expanding education is a starting point. The latter has also been observed in critical care settings abroad,32-34 indicating a global challenge regarding palliative care in critical care. To overcome this barrier, communication training focusing on eliciting patients’ life trajectories and values, such as VITAL TALK® and the Serious Illness Conversation Program, may be effective.35,36 Communication training has only recently been introduced in Japan. Therefore, it is important to determine how to increase it in the future.
The issues and barriers described thus far are not limited to specialist nurses. Reports indicate that intensive care and emergency physicians in Japan also recognize them. 37 Therefore, to advance palliative care in the critical care field, it is necessary to include nurses, physicians, and other professionals in education and system development efforts.
This study has some limitations. First, the response rate was only 51.9%; thus, the data is not fully reflective of the opinions of specialist nurses in Japan. Additionally, the study focused only on specialized nurses and excluded staff nurses’ perspectives. Future studies should expand the scope of palliative care nursing in the critical care field from various nurses’ perspectives. Second, the survey method was subjective, and it was possible that the actual practice situation was not accurately evaluated. Tanaka et al 38 developed quality indicators of palliative care for ICU patients, facilitating the objective identification of current palliative care practices and areas of inadequacy by analyzing electronic medical record data using these indicators. Therefore, the subsequent phase of our study will involve collection of medical records from nationwide critical care settings.
In conclusion, although there is a general recognition of palliative care principles, including symptom management and end-of-life care, there are significant gaps in the provision of primary palliative care in Japan, particularly in addressing patients’ social and spiritual suffering. Specialist nurses also perceived barriers such as insufficient knowledge and skills among medical staff and challenges in determining patient preferences for treatment goals. Targeted educational programs should focus on enhancing nurses’ skills in pain and symptom management, communication strategies for addressing social and spiritual needs, and methods for facilitating discussions about end-of-life care with patients and their families. Additionally, system improvements are necessary, including the development of protocols for identifying and addressing patients’ palliative care needs, establishing interdisciplinary teams to support primary palliative care delivery, and implementing tools to assess patient preferences for treatment goals and end-of-life care.
Footnotes
Acknowledgments
This survey was conducted when the ICUs and EDs nationwide in Japan were overwhelmed by the COVID-19 pandemic. We would like to express our heartfelt gratitude to all specialist nurses who participated in this study despite their busy schedules.
Author Contributions
Conceptualization: AK, YT, YK, and MM. Data curation: AK and YT. Formal Analysis: AK and MM. Funding Acquisition: AK and YK. Methodology: YK, YY, AT, JT, and MM. Project administration: AK. Visualization: AK. Writing the original draft: AK, TY, and MM. Writing, review, and editing: AK, YT, YK, HY, AT, JT, and MM.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: YK received honoraria for educational lectures from Chugai Pharma Co., Ltd. And Daiichi-Sankyo Co., Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI Grant Number 24K13775.