
Abstract
Purpose
In the US, nearly one-third of skilled home health (HH) patients and nearly one-half of hospice patients live with Alzheimer’s disease and related dementias (ADRD). Hispanic older adults are more likely to live with ADRD than white non-Hispanic older adults. Persons with ADRD, compared to their counterparts without ADRD, have a prolonged trajectory of decline and experience multiple care transitions between health care settings, bringing risks for poor outcomes. Little is known about patients transitioning between skilled HH and hospice. We aimed to determine if there were demographic and/or diagnostic variables associated with the frequency of transitions between skilled HH and hospice.
Design
In a cross-sectional study, we used Medicare claims data from 2020 and descriptive statistics including Chi-Square to determine demographic and diagnostic differences in frequency of care transitions between skilled HH and hospice for older adults with ADRD.
Findings
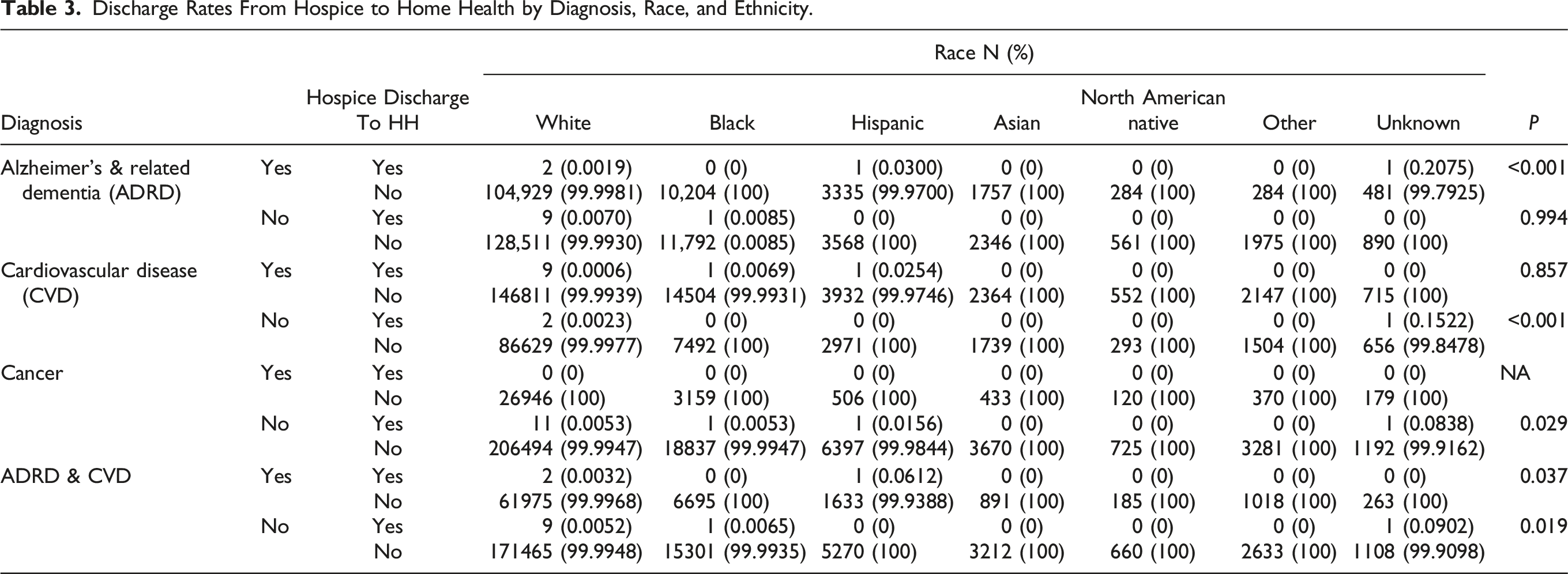
In N = 272,323 hospice episodes, Hispanic older adult beneficiaries with ADRD and co-occurring cardiovascular disease (CVD) had significantly higher rates of care transitions from hospice to skilled HH (P = 0.037) than other racial and ethnic groups with both diagnoses.
Conclusions
Our findings provide evidence of disparities in care transitions from hospice to skilled HH for Hispanic older adults living with ADRD and CVD. Multiple factors may impact this result: Hospice low quality scores, insufficient advance care planning and understanding of hospice philosophy, and policies affecting eligibility. Implications include policy change and greater coordination of care for older adults with co-occurring ADRD and CVD, with attention to health equity.
Keywords
Introduction
In the US, nearly one-third of skilled home health (HH) patients and nearly one-half of hospice patients live with Alzheimer’s disease and related dementias (ADRD). 1 Skilled HH is defined by Medicare as physician-ordered long-term care provided to homebound patients by nurses, nurse aides, physical therapists, occupational therapists, speech therapists, and/or social workers. 2 Medicare defines hospice as a service for people with a prognosis of 6 months or less who no longer opt to pursue curative treatments. 2 Hospice provides skilled nursing case management, aide services, chaplain care, and social work support as well as durable medical equipment, care supplies, and medications and treatments related to comfort. 2 Hospice care is provided in the patient’s residence or at an in-patient facility. 2 Most hospice beneficiaries receive hospice care until they die and are thereby discharged; however, some patients are discharged from hospice while still living. Live discharge may be patient-initiated or agency-initiated. For example, a patient-initiated live discharge happens when a patient chooses to disenroll for personal reasons; an agency-initiated live discharge happens when a clinician cannot document patient decline consistent with a 6-month prognosis. Post-acute care transitions between skilled HH and hospice warrant investigation because the decision to pursue hospice care involves a significant shift in focus from rehabilitation and cure to comfort and quality of life. Further, care transitions involving live discharge from hospice are associated with adverse outcomes. 3
In 2016, Wang found patients disenrolled from hospice were likely to experience multiple care transitions involving skilled HH, hospital, skilled nursing facilities, and hospice. 4 Wang’s historically significant study demonstrated that hospice enrollees discharged to skilled HH were likely to ultimately transition back to hospice. Such hospice care transitions may disrupt continuity of care, place patients at risk for adverse outcomes such as hospitalization and emergency department visits, cause distress, and reduce the quality of life for patients and families. Beyond Wang’s study, there is a dearth of literature about transitions between the particular settings of skilled HH and hospice.5,6
End-of Life Care for Persons Living with Alzheimer’s Disease and Related Dementias
Diagnoses of ADRD are significant to discussions about end-of-life care because they are characterized by a long trajectory of decline when compared to other diagnoses. For example, individuals with ADRD have high, sustained functional impairment during the last 4 years of life when compared to persons without ADRD in the last 6 months of life. 7 Despite such evidence of decline, persons with ADRD receive less skilled HH and hospice care than those without ADRD.8,9 Minoritized patients, specifically people identified as Black or Hispanic who are living with ADRD, are at higher risk for live discharge from hospice than their white non-Hispanic counterparts living with ADRD.9-15 Live discharge from hospice for persons living with ADRD and their care partners has been described as distressing and confusing; associated with numerous losses; and referred to disparagingly as being expelled from hospice.16,17 Live discharge from hospice affects caregiver decisions about re-enrollment in hospice because they are unsure of the appropriateness of the hospice service if their loved one cannot continuously receive it until death. 17
Persons Nearing End of Life with ADRD and Cardiovascular Disease
The link between cardiovascular disease (CVD) and ADRD has been well-established. CVD risk factors can contribute to blood-brain barrier dysfunction and reduced cerebral blood flow, and amyloid deposits may cause damage to both the heart and the brain. 18 Not all persons with ADRD have co-occurring CVD, but cardiovascular risk factors have been associated with worse cognitive function in multiple populations. 19 Additionally, in the US from 1999 to 2016, deaths from co-occurring heart failure and dementia constituted 4% of all heart failure deaths and 9.04% of all dementia deaths. 20 However, it is unknown whether co-occurring CVD and ADRD diagnoses are significant variables in home health-hospice care transitions.
Knowledge Gap
Hospice care transitions may disrupt continuity of care, place patients at risk for adverse outcomes such as hospitalization and emergency department visits, cause distress, and reduce the quality of life for patients and families. 3 While it is known that Hispanic and Black patients living with ADRD are at higher risk for live discharge from hospice than their non-Hispanic white counterparts with ADRD, little is known about their post-hospice destination. 11 A systematic review of the literature revealed a gap in knowledge regarding transitions between skilled HH and hospice for persons with ADRD. 5 Osakwe et al 6 recommended that future studies on transitions between skilled HH and hospice use claims data to capture diagnoses, a call to which the present study responds. Therefore, the purpose of our study was to describe diagnostic variables and demographic covariates associated with transitions between skilled HH and hospice for Medicare beneficiaries with ADRD.
Methods
Study Design
Ethics approval was obtained from East Tennessee State University. A data use agreement was completed. This correlational study used national Medicare claims data in the US from 2020. A care transition was defined as discharge disposition from hospice to skilled HH or from skilled HH to hospice. The datasets did not indicate whether the discharges were patient-initiated (ie, revocation of a benefit) or agency-initiated (eg, due to no longer fitting eligibility criteria or other reason).
Data Sources
Our study used Medicare claims data, a reliable and comprehensive source of a representative sample of older adult beneficiaries in the US and includes information such as type and dates of service, diagnoses, and procedures. Skilled HH patient diagnoses and discharge to hospice variables were identified in the Standard Analytic File Home Health (SAFHHP) Limited Data Set (5% extraction). Demographic covariates for both skilled HH and hospice beneficiaries were obtained from the Master Beneficiary Summary File (MBSF) (5% extraction). Hospice patient diagnoses and discharge to skilled HH were identified in the Standard Analytic File Hospice (SAFHSP) Limited Data Set (5% extraction), and the Home Health Claims OASIS Limited Data Set (100% extraction).
Sample
Our study focused on older adult (aged 65+) beneficiaries enrolled in skilled HH or hospice care. An episode refers to the time the beneficiary is admitted to the health service up to 60 days. 2 An episode was the primary unit of analysis in this study.
Procedures
We hypothesized that episodes with beneficiaries with ADRD involved more frequent care transitions between skilled HH and hospice than episodes with beneficiaries without ADRD. Further, we hypothesized that there are no demographic differences in the frequency of transfers between skilled HH and hospice for episodes with beneficiaries with ADRD.
Measures
We systematically investigated care transitions from hospice to skilled HH for three distinct groups of older adult Medicare beneficiaries: (1) those with ADRD; (2) those with co-occurring ADRD and CVD; and (3) those with cancer but without ADRD or CVD. We examined demographic covariates, including age, gender, race, and ethnicity, to identify potential differences in the frequency of these care transitions. For each group, we calculated discharge disposition rates and used Chi-Square tests to evaluate the statistical significance of any disparities. Our significance level was set at P = 0.05, meaning that differences between groups were considered statistically significant if the probability of occurrence was less than 5%. This analysis aimed to provide insights into potential disparities in care transitions and to contribute to the understanding of health care services for older adults facing the complex challenges of living with ADRD.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows (Version 28.0). 21 Descriptive statistics were reported for demographic covariates including age, gender, race or ethnicity, and for diagnoses of ADRD, CVD, cancer, and both ADRD and CVD for both skilled HH and hospice datasets. Chi-square tests were conducted to examine the association between the diagnoses of 4 types of conditions and the discharge status between skilled HH and hospice. A two-tailed P value of less than 0.05 was considered statistically significant for all analyses.
Results
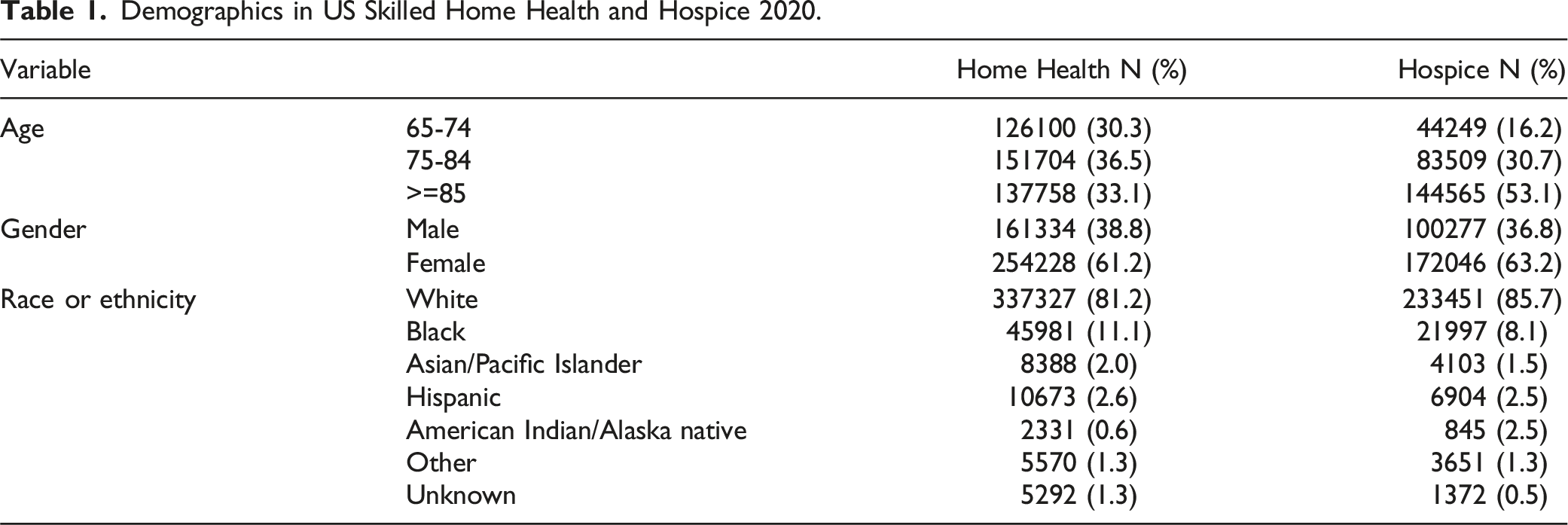
Demographics in US Skilled Home Health and Hospice 2020.
Diagnoses in Skilled Home Health and Hospice 2020.

Discharge Rates From Hospice to Home Health by Diagnosis, Race, and Ethnicity.
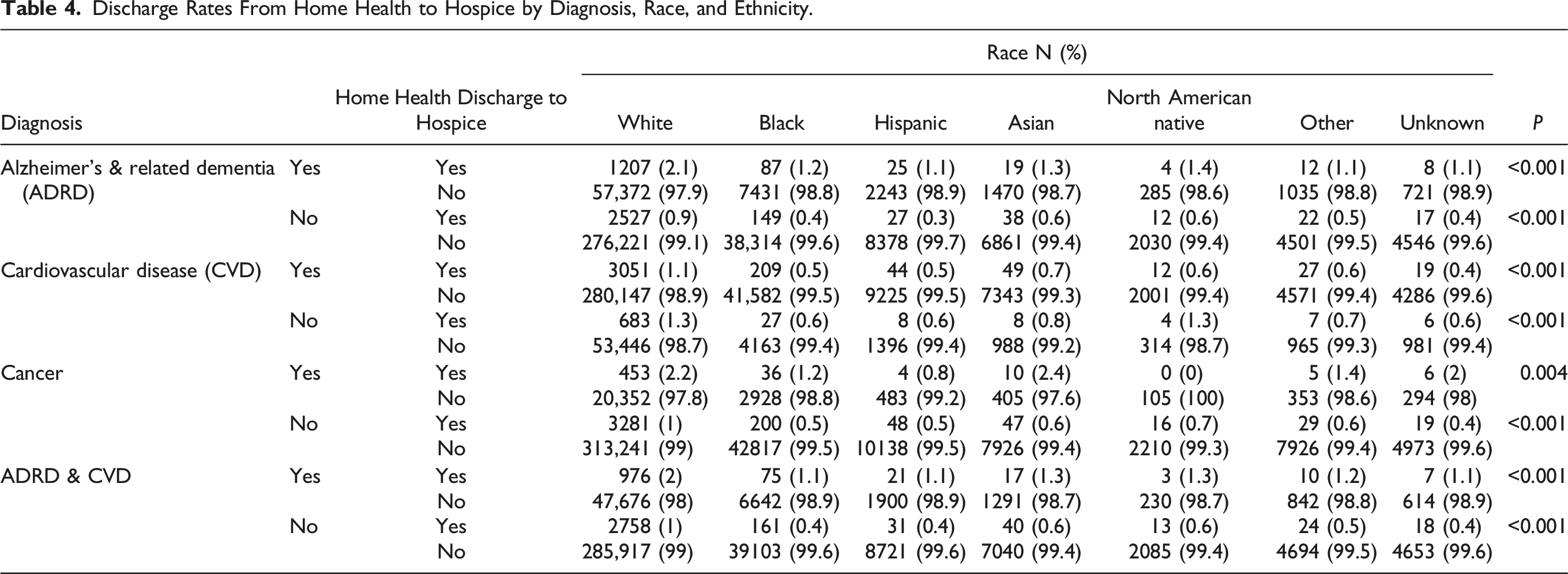
Discharge Rates From Home Health to Hospice by Diagnosis, Race, and Ethnicity.
Discussion
Our findings suggest that Hispanic beneficiaries with co-occurring CVD and ADRD were significantly more likely to be discharged alive and transition to skilled HH from hospice than other racial, ethnic, or diagnostic groups. Our findings are consistent with multiple studies showing that Hispanic persons living with ADRD are at higher risk for live discharge from hospice than their white non-Hispanic counterparts with ADRD.10-15 However, our findings add to the literature specific evidence about hospice transitions to skilled HH for Hispanic patients with co-occurring ADRD and CVD. Multiple factors may influence the result in this population, including the impact of low quality scores in the overall services rendered, insufficient advance care planning, a gap in understanding the philosophy of hospice care, lack of lay supporters of hospice and palliative care within Hispanic communities in the US, and the impact of Medicare audits on determinations of eligibility.11,14,22-29
Hispanic older adults are 1.5 times more likely to live with ADRD and to live an average of one year longer with the disease than non-Hispanic white older adults, prolonging the care period for family care partners. 30 Hispanic care partners experience more burden (45%) than non-Hispanic white care partners (33%). 31 Cultural factors and support systems affect Hispanic caregiving experiences via gender norms, role satisfaction, and resource delivery. 32 Additionally, Hispanic care partners often lack knowledge about ADRD and pursue professional services (eg, hospice or skilled HH) later than non-Hispanic caregivers. 33
Barriers to hospice enrollment among Hispanic persons have included limited knowledge, caregiver bias, language barriers, fear of deportation, economic restraints, family decision-making, religious beliefs, preference for paternalistic approach, mistrust in health care providers, and physician bias. 22 Disparities in hospice utilization may include financial stressors as well as cultural preferences including non-disclosure of primary diagnosis.23,26 Hispanic persons are underrepresented in hospice care, and little research has focused on Hispanic persons’ experiences with hospice.23,25,30 However, between 2004-2016, hospice use among Mexican-Americans in particular increased when compared to the national average, though they were more likely to have short stays (39%) compared to the national average (29%). 26
While Medicare beneficiaries have the right to choose the setting of their health care when nearing the end of life, skilled HH may not be the optimal setting for such care. For example, Jones et al 34 found among patients with heart failure discharged from the hospital to skilled HH that 15% died within 6 months, indicating they could have benefited from the specialized end-of-life care provided by hospice. Further, skilled HH may not be optimal for Black and Hispanic patients nearing end of life, since they have a 2.2-percentage point and a 2.5-percentage point lower adjusted probability of high quality HH agency use, respectively, compared to their white counterparts within the same neighborhoods. 35 Quality measures may be more accurate measures of equity than enrollment numbers; 36 therefore, future research should examine whether HH quality scores are correlated with goal-concordant care measures or hospice transition rates.
Patients and their caregivers who might benefit from new or continued hospice services may end up receiving skilled HH, where their goals of care may not be met since skilled HH is rehabilitation-focused rather than comfort-focused. However, while hospice care has the potential to provide optimal end-of-life care, hospice quality of care and disparities must also be examined. The likelihood of being discharged alive from hospice is higher among minoritized patients and in hospices in the lowest quartile of quality ratings. 29 Some examples of poor hospice quality ratings among Hispanic persons include receiving more religious and spiritual support than they wanted, being less likely to receive opioid analgesics than non-Hispanic patients, and being less likely to achieve a pain-free status at discharge than non-Hispanic patients.14,37 Among hospice enrollees, Hispanic persons experience mixed end-of-life outcomes compared to non-Hispanic persons, including length of stay, live discharge, hospitalization, site of death, hospice staff acting against patient wishes, and symptom-related outcomes. 27
While evidence shows the two settings of hospice and skilled HH are both in need of quality improvement, the provision of culturally adapted patient navigation programs including the use of validated Spanish language tools can improve advance care planning, adoption of do-not-resuscitate directives, and hospice enrollment among Hispanics in the US.22,38,39 Future studies should explore the effects of culturally-tailored palliative care interventions on hospice quality ratings and on health equity in care transitions.
Next, health policy may affect hospice care transitions. For example, in 2016, the Center for Medicare and Medicaid Services (CMS) implemented a 2-tier payment system under the Improving Medicare Post-Acute Care Transformation (IMPACT) Act, reducing reimbursement for hospice stays longer than 60 days, which been associated with reductions in the total number of hospice patients with ADRD.40,41 Future research should investigate such policies’ effects on health equity among diverse persons living with ADRD. The effect of fiscal penalties for hospice agencies billing for patients whom auditors may deem ineligible may impact the enrollment and discharge decisions that hospices reach regarding patients with potentially longer lengths of stay. Patients with ADRD fit the profile of patients at risk for live discharge from hospice care due to their long trajectory of decline.
Our findings merit discussion because post-acute care transitions from hospice to skilled HH involve a shift from comfort-focus to cure-focus, potentially compromising patient and family quality of life. It is unclear whether the patient and family goals are concordant with this shift; that is, just because the health care service changes does not necessarily mean that the patient- and family goals change. For example, Beltran 27 found that Hispanic patients made decisions about end-of-life care based on a limited understanding of care options. Hispanic patients and their care partners have described the impetus for choosing hospice as (a) the need for in-home care and (b) not having other options for accessing such services. Beltran recommended that health care providers engage with Hispanic patients and their care partners in ongoing needs assessment and education about available services, 27 since some studies have shown that when Hispanic patients are informed about end-of-life care options they are more likely to choose less invasive treatments.42,43
Limitations
The most recent datasets at the time of data collection were from 2020, when the COVID-19 pandemic may have impacted health care decisions. Additionally, although statistical significance was found, discrete numbers of episodes were small. Another limitation is that the dataset did not show whether the episodes of hospice discharge were agency-initiated (due to stabilization or extended prognosis) or patient/family-initiated (due to changes in goals of care or other reasons). Medicare datasets capture Medicare beneficiaries only; therefore, our data did not include patients classified as self-pay, indigent, or having private insurance. This limitation affects generalizability of our findings because access to Medicare benefits requires certain citizenship status, which not all patients may have. Other studies have used non-Medicare databases such as the National Inpatient Sample (NIS), though no such databases exist for post-acute settings. 23 Data on quality outcomes is independent of other Medicare sources of claims data that include diagnoses. Further, data resulting from clinician identification of patient ethnicity in administrative datasets may differ from data resulting from participant self-identification of ethnicity in other studies. Finally, our findings might be limited by the choice of statistical test for analysis; future studies employing multivariate analyses may provide more detail.
Conclusions
Skilled HH and hospice are critical services for older adults living with ADRD, yet transitions between the two services can be disruptive and confusing to patients and care partners when goal concordant care is paramount. Hispanics with co-occurring ADRD and CVD were significantly more likely to transition from hospice to skilled HH than other diagnostic and demographic groups, potentially increasing their risk for disjointed care coordination. Specific attention to health equity and improved care coordination across systems of care for Hispanic older adults with co-occurring ADRD and cardiovascular disease is needed to ensure high quality palliative and end-of-life care.
Footnotes
Acknowledgements
The authors would like to acknowledge the Epsilon Sigma Chapter of Sigma Theta Tau International and East Tennessee State University for funding the research. A portion of author SEB’s time was supported by the Dick and Timmy Burton Post-Doctoral Fellowship at the University of Utah College of Nursing, as well as the National Institute on Aging of the National Institutes of Health under award number R01AG069033. The content is solely the responsibility of the authors and does not necessarily represent the official views of the University of Utah or the National Institutes of Health.
Author Contributions
Sharon E. Bigger: Corresponding author, conception of idea, data collection, literature review, interpretation of results.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Epsilon Sigma At-Large Chapter of Sigma Theta Tau International, National Institute on Aging of the National Institutes of Health; R01AG069033, The Dick and Timmy Burton Post-Doctoral Fellowship at the University of Utah College of Nursing, 10.13039/100006514; East Tennessee State University.