
Abstract
Introduction
Patient attitude to death is associated with outcomes in hospice care settings. This Korean study investigated the association between terminal cancer patient death acceptance and symptom control and quality of care (QoC) as perceived by family caregivers (FCs).
Methods
A multicenter cross-sectional survey was conducted in nine inpatient hospice care units, and the data of 108 dyads (terminal cancer patients who responded to the revised Death Attitude Profile and their primary FCs) were analyzed. Dyads were dichotomized into high and low groups by death-acceptance level. Multivariate regression models were used to examine the association between death acceptance and symptom severity/QoC as perceived by FCs.
Results
Patients in the high acceptance group were younger, educated to a higher level, more religious, and had better-functioning families. Patients with severe shortness of breath were less likely to accept the inevitability of death. FCs of patients with high acceptance of death were more satisfied with QoC, particularly in domains of individualized care and family relationships. In addition, the positive association between patient acceptance and FC satisfaction with care was significant in dyads of young or female patients, patients with a low education level, and patients not cared for by a spouse.
Conclusion
Terminal cancer patient death acceptance is associated with symptom control and FC perceived QoC.
Introduction
Patients with terminal cancer and their families may suffer physically, emotionally, mentally, socially, and spiritually, and hospice care requires a clinical context of care that addresses these patient needs. 1 When end-of-life care is compassionate and family-centered, it can increase patient and family satisfaction and reduce the likelihood of depression among bereaved relatives. 2 A recent Cochrane review indicated that compared to usual care, hospice care offers clinically relevant benefits that influence different outcomes, such as patient health-related quality of life, symptom burden, and patient satisfaction with care. 3
Health professionals perceive a good death as one in which physical pain is controlled and patients and families are psychologically prepared.
4
A psychological inclination towards death is usually characterized as death anxiety,
5
although death acceptance is considered a favorable psychological state. Nonetheless, addressing a patient’s perception of mortality is considered an essential component of advanced cancer care. Previous studies have focused on relationships between acceptance of death and psychological aspects, such as demoralization or emotional distress
6
or the identification of vulnerable groups,
7
and as a result, data on death acceptance and outcomes, such as symptom control and quality of care (QoC), in hospice settings is lacking. In this study, we primarily examined the relationship between acceptance of death by terminal cancer patient and symptom control/QoC as perceived by family caregivers (FCs) in inpatient hospice care settings. Our secondary aim was to identify patient subpopulations exhibiting a robust association between death acceptance and QoC as perceived by FCs (Figure 1). Conceptual framework.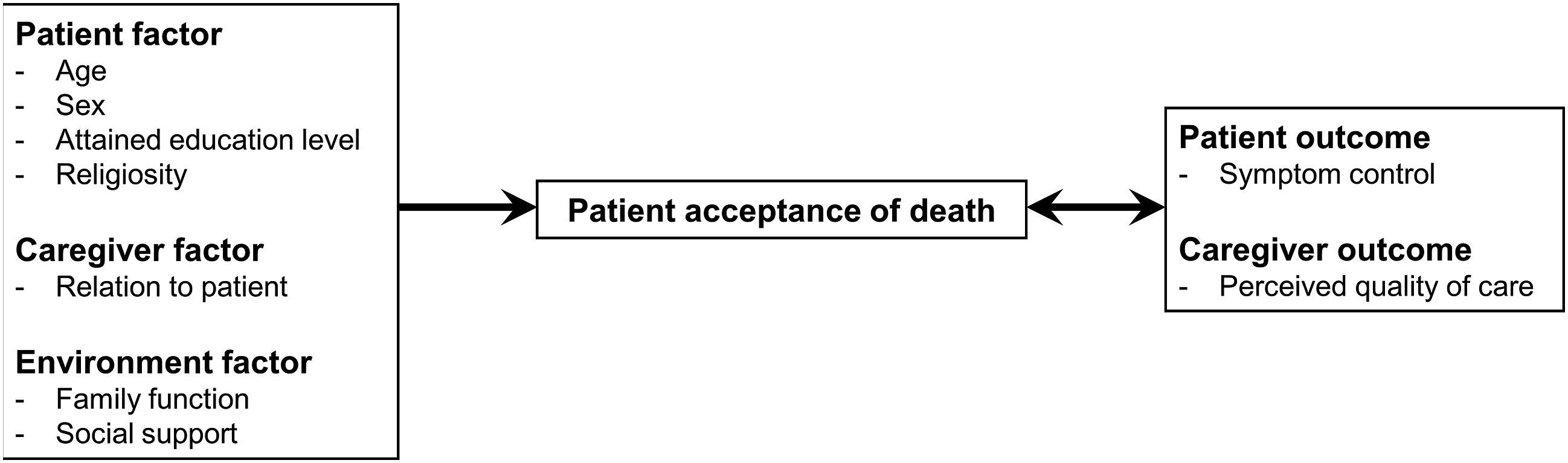
Methods
Study Design and Subjects
In this multicenter cross-sectional study, we collected data on patient-FC dyads from 9 hospice care units in Korea from September 2021 to May 2023. All units were enrolled in the National Hospice and Palliative Care registry, and the quality of service provided was regularly monitored and verified by the National Hospice Center. 8 Only terminal cancer patients who provided informed consent were admitted to these units for inpatient hospice care, which included the suspension or discontinuation of life-sustaining treatment, in accordance with the ‘Hospice and Palliative Care and Decisions on Life-Sustaining Treatment for Patients at the End of Life’ act. Admitted patients were consecutively screened to assess eligibility. Patient eligibility criteria were an age ≥20 years, an alert mentality, the ability to communicate during interviews and complete questionnaires with minimal assistance, and the provision of informed consent. Patients were also required to identify their primary FC, that is, the relative who provided most informal care. FCs were excluded if they were under 20, could not complete questionnaires satisfactorily, were unable to communicate with an interviewer, or did not agree to study participation. The most common reason for non-participation was discomfort for patients and FCs. A priori sample size estimation could not be performed due to the lack of a similar study.
The researchers and trained assistants explained the aim and scope of the survey to the participants and administered self-reported questionnaires after obtaining informed consent. Researchers checked responses immediately after receiving completed surveys and promptly followed up for missing data to minimize missing values. A total of 108 dyads were included in the analysis. All patients and FCs provided written informed consent, and the institutional review boards of each medical center approved the study.
Measures
The Korean version of the Death Attitude Profile-Revised (DAP-R) was employed to quantify patient acceptance of death. 9 The DAP-R encompasses five subthemes, namely fear of death, death avoidance, escape avoidance, approach acceptance, and neutral acceptance; the latter was used to assess death acceptance. Patients were requested to rate their level of acceptance on a 7-point Likert scale, ranging from 1 (not at all) to 7 (very much). Based on the observed distribution (median, 5.8 pts), patients with mean scores of ≥6 pts were arbitrarily allocated to the high death-acceptance group, and the remainder were allocated to the low death-acceptance group.
The M. D. Anderson Symptom Inventory was used to assess symptoms. 10 Patients were requested to rate the severity of each symptom they had experienced during the preceding 24-hour period using an 11-point scale ranging from 0 (absent) to 10 (most severe imaginable). Symptoms were divided into three groups based on severity: none or mild (≤3), moderate (4-6), or severe (≥7). The “Family Caregiver Quality of Care Questionnaire - End of Life” was used to assess the quality of end-of-life care. 11 This instrument contains 16 items rated using a 4-point Likert scale ranging from 1 (not at all) to 4 (very much), and four domains, viz, dignity-conserving care, care by healthcare professionals, individualized care, and family relationships.
Patient information, including age, sex, attained educational level, and religiosity, and caregiver-provided information, such as the nature of the patient/FC relationship and information on environmental factors, such as family function and social support, were collected. FC rated family function was assessed using the Korean version of the family Adaptation, Partnership, Growth, Affection, and Resolve instrument. 12 Each of these five items was evaluated using a 3-point Likert scale based on the frequency of each experience: 2 = almost always, 1 = sometimes, and 0 = hardly ever, which resulted in a total possible score of 10. To evaluate the structure of the social support system, we used the Medical Outcome Study Social Support Survey, which encompasses four distinct subcategories: emotional/information support, tangible support, positive social interaction, and affectionate support. 13 The survey consists of 19 items, which were rated by FCs using a five-point Likert scale (from 1 (not at all) to 5 (always)). Raw scores of each item were subsequently transformed into a unified 0 to 100 scale.
Statistical Analysis
The chi-square test or an independent t test was used to compare the characteristics of the high and low death-acceptance groups. Multivariate regression analysis adjusted for covariates, such as age, sex, educational level, religiosity, spousal relationship, social support level, and family functionality, was used to determine the proportions of patients with high death-acceptance with respect to symptom severity and QoC scores as perceived by FCs. The odds ratios (ORs) and corresponding 95% confidence intervals (CIs) for the perception of a high QoC were calculated using multivariate logistic models, and this analysis was repeated for subgroups. The analysis was performed using STATA/MP version 17.0 (Stata Corp., College Station, TX, USA), and statistical significance was accepted for P values <.05.
Results
Characteristics by Death Acceptance Level.
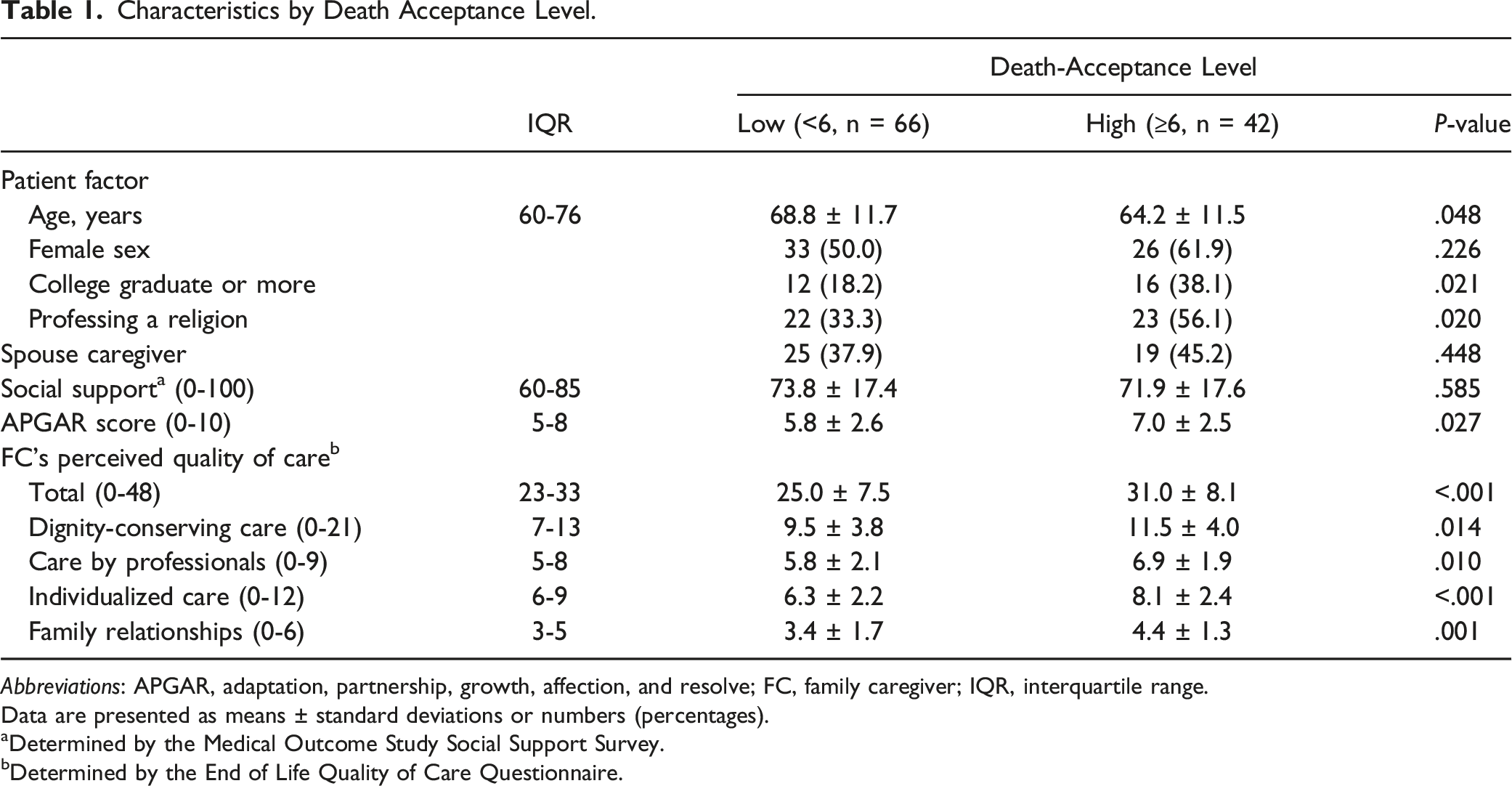
Abbreviations: APGAR, adaptation, partnership, growth, affection, and resolve; FC, family caregiver; IQR, interquartile range.
Data are presented as means ± standard deviations or numbers (percentages).
aDetermined by the Medical Outcome Study Social Support Survey.
bDetermined by the End of Life Quality of Care Questionnaire.
Regarding the correlation between death acceptance and symptom severity, patients in the mildly symptomatic group seemed to be more accepting of death. Notably, patients who experienced shortness of breath were significantly and dose-dependently less likely to exhibit high death acceptance (Figure 2). Estimateda proportion of patients with high death acceptance by symptom severity. aAdjusted for patient factors (age, sex, educational level, and religiosity), spousal relation, social support level, and family functionality. *P < .05 by multivariate logistic regression.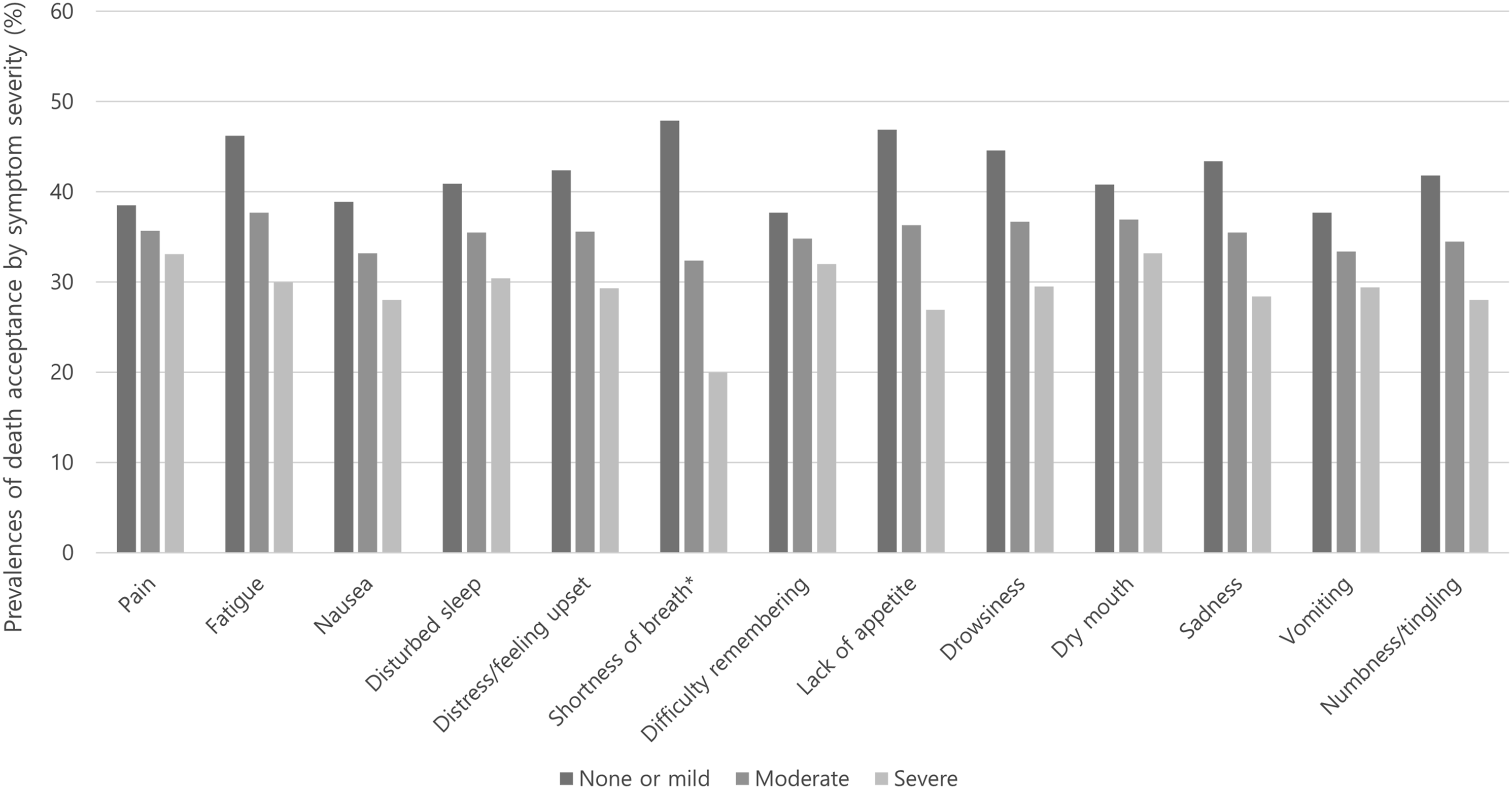
Figure 3 shows the relationship between FC perceived QoC scores and patient death-acceptance. The FCs of patients with high death acceptance were significantly more satisfied with QoC, particularly in the domains of individualized care and family relationships than the FCs of patients with low death-acceptance. Estimateda QoC scores perceived by family caregivers according to patient acceptance of death. aAdjusted for patient factors (age, sex, educational level, and religiosity), spousal relation, social support level, and family functionality. *P < .05 and **P < .01 by multivariate regression.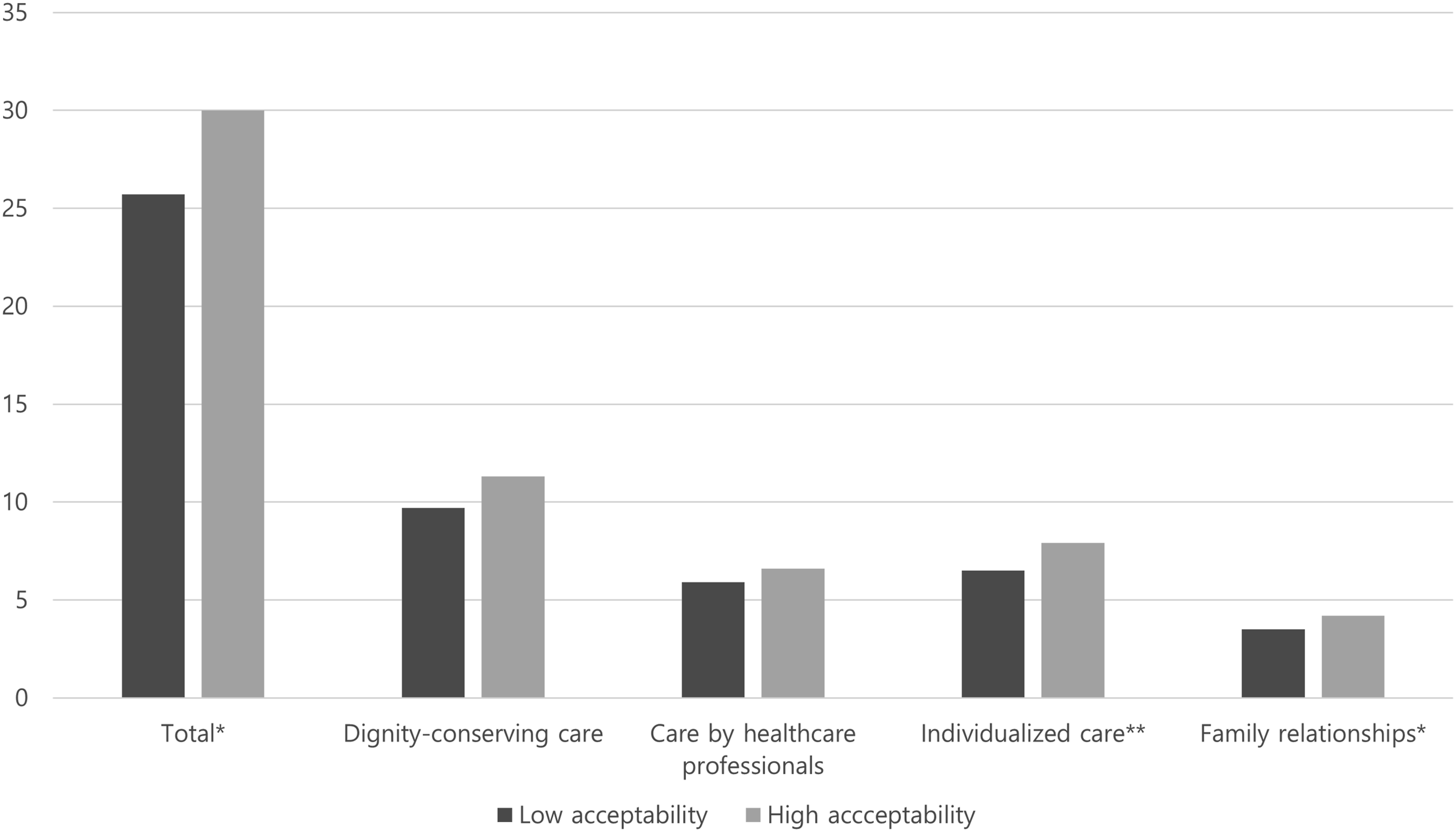
Associations Between Patient Death-Acceptance and FC Perceived QoC for All Patients and Patient Subgroups.
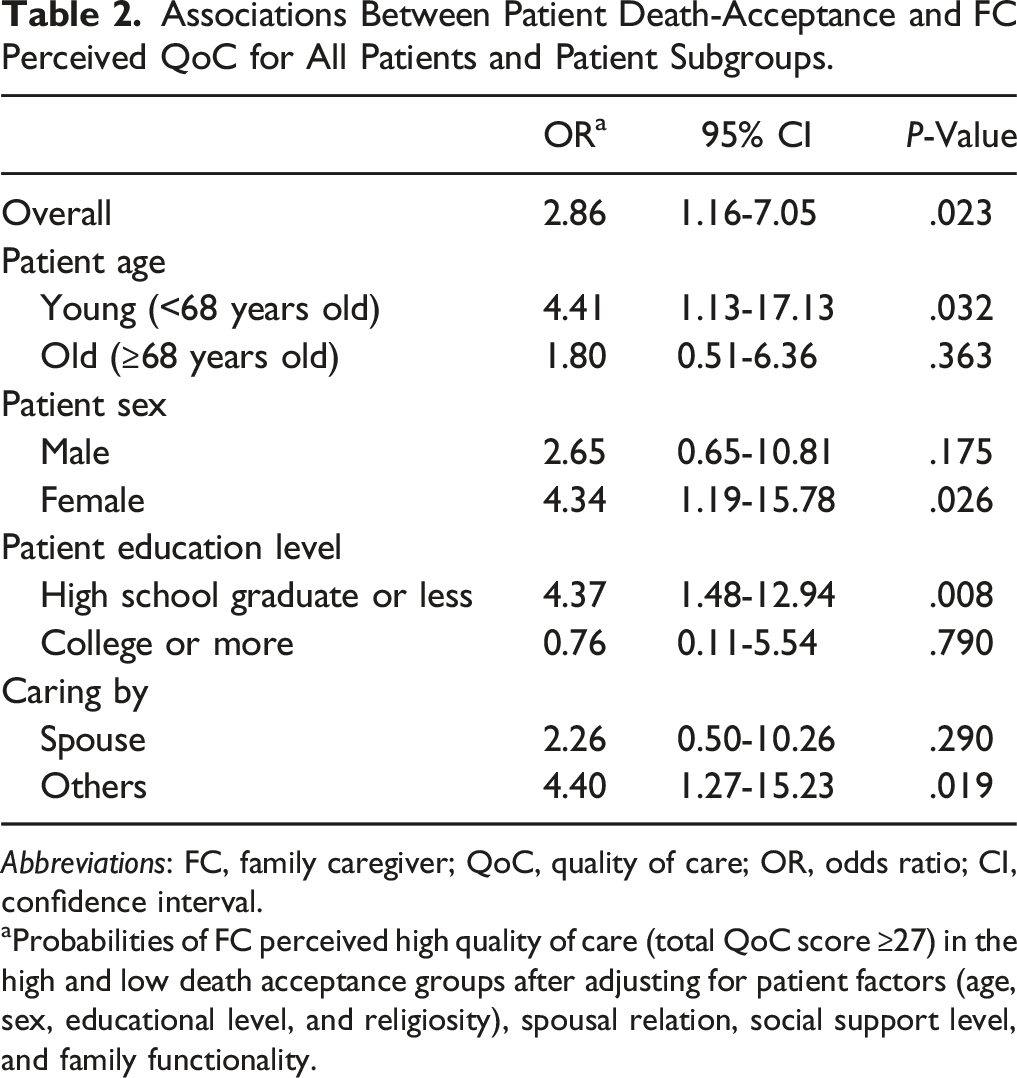
Abbreviations: FC, family caregiver; QoC, quality of care; OR, odds ratio; CI, confidence interval.
aProbabilities of FC perceived high quality of care (total QoC score ≥27) in the high and low death acceptance groups after adjusting for patient factors (age, sex, educational level, and religiosity), spousal relation, social support level, and family functionality.
Discussion
Death acceptance is an overall predictor of psychological adaptation during the process of dealing with advanced cancer. 14 Few dyadic studies have been conducted on death acceptance in a palliative care setting. A recent Italian study described how early palliative care might influence the acceptance of death in patients with advanced cancer and their FCs. 15 This multicenter study indicates that high acceptability is positively associated with several outcomes, even in hospice care settings. In particular, it shows that high death acceptance is inversely associated with shortness of breath and positively associated with FC-perceived QoC, especially concerning individualized care and family relationships. A better understanding of acceptance of death may be necessary to help terminal cancer patients manage their symptoms and improve QoC. In addition, the study highlights the potential significance of death acceptance even in cultural contexts where discussing death is challenging. In Korea, death is still considered a taboo subject. 16 Discussing death is often seen as disrespectful or unfilial, and family-centered decision-making prioritizes harmony over individual autonomy, further discouraging open conversations. 17 These cultural norms underscore the importance of culturally sensitive hospice care approaches that create supportive environments for end-of-life discussions.
In this study, milder symptoms tended to be associated with better acceptance of death, which aligns with the notion that effective symptom management is the foremost requirement of a good death. 18 Interestingly, shortness of breath was significantly associated with low death-acceptance. Patients commonly use this term to describe dyspnea, which often worsens near the end-of-life, 19 and may be the symptom most closely associated with death. 20 Intractable breathlessness is interactively associated with anxiety in patients with terminal cancer 21 and may prevent death acceptance. More comprehensive control of dyspnea is needed to enable terminal cancer patients to face death, reduce emotional distress, and thus, increase the quality of hospice care.
Notably, a positive correlation was found between patient acceptance of death and FC-perceived QoC. Cancer patients and their FCs often experience a heightened level of interconnectedness, especially during the terminal phase, which lead to the World Health Organization recommending that the quality of life and burden imposed on FCs should be considered during palliative care. 22 However, little research on hospice outcomes has been undertaken in a dyadic manner. A prospective German study showed that patient quality of life influenced FC perceived burden, 23 which is consistent with our results. This finding shows that providing appropriate care to terminal cancer patients and their FCs would facilitate greater positive acceptance of death by patients.
Our study suggests a domain-specific significant association between death acceptance and QoC. Patients of FCs satisfied with individualized care and family relationships are more likely to accept death, which underscores the importance of person-centered and family-focused care in hospice settings. 1 Individualized care facilitates effective communication 24 and helps patients accept death by effectively identifying the unmet needs of terminally ill cancer patients and addressing physical, psychological, and emotional deficiencies. A positive relationship among family members, which constitute the primary support unit by providing comfort and communication, 25 can also cultivate a sense of security for terminal cancer patients, which in turn contributes to holistic stability and aids the acceptance of death.
Subgroup analysis identified characteristics of dyads exhibiting significant positive associations between patient death acceptance and FC perceived QoC for younger and female patients, patients with a lower educational status, and those cared for by other than a spouse. These associations have not been previously studied but might be partially explained by the anticipation of accepting death. It would appear that patient subpopulations identified in the present study found it difficult to talk about death directly. Overall, women facing death are more likely to exhibit death anxiety than men because they worry more about how their deaths will affect loved ones. 26 It is no surprise that discussing death is troubling to young patients, those educated to a low level, and those cared for by a non-spouse. We hypothesized that if these individuals accept death despite a low acceptance of death, their FCs would strive to increase QoC. Although this hypothesis requires further investigation, this finding suggests that efforts to enhance death acceptance (e.g., Acceptance and Commitment Therapy and Death Education)27,28 would raise FC perceptions of QoC. Furthermore, FC satisfaction with care is closely associated with FC quality of life in the bereaved 29 and pre-loss stage. 30
This study has several limitations. First, although its cross-sectional design enabled us to identify associations, it prevented our establishing causative relationships. In addition, the study design did not address the likelihood that death acceptance can vary with time. Longitudinal studies and repeated measures analysis are required to confirm our results. Second, the validity of the Korean version of the DAP-R was not formally tested. However, we performed a brief translating process; two bilingual doctors first translated the questionnaire and reached consensus, and then a pilot test was conducted on two doctors, five nurses, one social worker, two patients, and three FCs. Third, we exclusively recruited inpatient-FC dyads from hospitals, and thus, our findings might not be applicable to all terminal cancer patient-FC dyads, such as those receiving home care or those being cared for in an independent hospice care unit. In addition, the use of convenience sampling limited generalizability. Finally, we did not differentiate between religiosity and spirituality, which could have impacted our results.
In conclusion, death acceptance by terminal cancer patients was found to be associated with symptom control and FC perceived QoC. To improve FC satisfaction with hospice services, greater efforts should be made to address death acceptance and assess symptoms. Finally, we recommend that intervention studies be conducted to examine the effect of communication regarding prognosis or death on FC-perceived QoC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: In Cheol Hwang have received the funding from the Gachon University Gil Medical Center (No. FRD2021-14), which had no role in study design, data collection, analysis, decision to publish, or manuscript preparation.