
Abstract
Background
While advance care planning (ACP) can facilitate a “good death” for people living with cancer, there remain gaps in understanding how to optimize ACP for better patient outcomes. This formative research aimed to explore experiences with advance care planning among oncology and primary care practitioners in primary/tertiary care settings.
Methods
The research team conducted structured and semi-structured in-depth interviews with family medicine practitioners (n = 12) and medical oncologists (n = 12) to understand their approaches to ACP.
Results
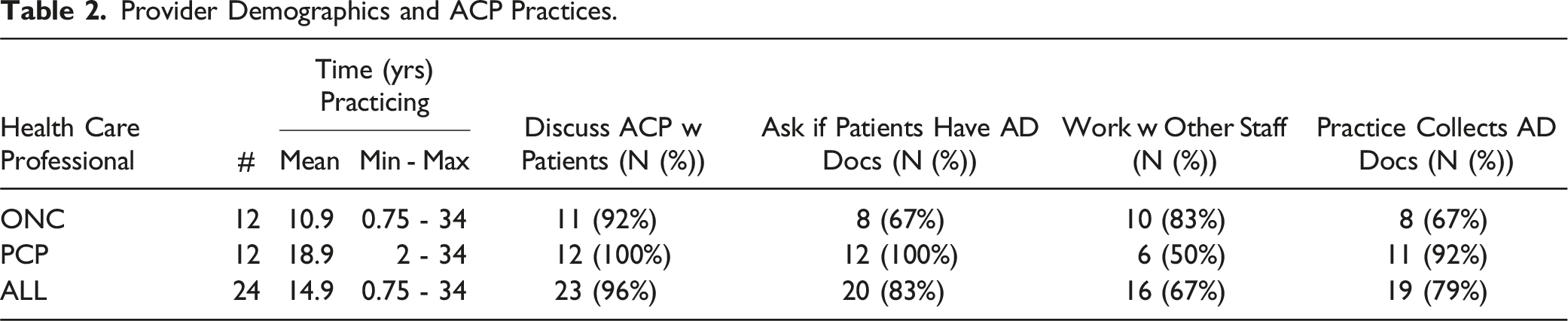
While oncologists and PCPs shared many of the same concerns about advance care planning, their unique contexts and specialties influenced their perspectives on the approach to ACP. Though oncologists and PCPs were both very likely to discuss ACP with their patients, oncologists more often discussed conducting ACP with other members of the health care team (e.g. social workers). Furthermore, disciplines differed in their emphasis on particular types of ACP documentation. Semi-structured interviews also revealed issues related to provider-patient communication as well as institutional challenges. Participants discussed their processes for timing the ACP conversation, addressing language-use challenges, assessing patient goals, and ensuring a good ACP workflow.
Conclusions
Participants recommended areas for institutional support and intervention to improve provider-patient ACP interactions.
Keywords
Background
While there are potential benefits of advance care planning (ACP) conversations for improving end-of-life care,1-3 health care providers, and particularly oncologists, may be disinclined to have them4,5 due to a concern that discussing patient prognosis will quash hope. 6 Because the goal of ACP is to prepare for medical emergencies or serious illness, it is often recommended that patients discuss ACP with their family and primary care practitioner (PCP) before the plan becomes necessary. 7 However, a U.S.-based Kaiser Family Foundation study found that only 10% of all adults with serious illness surveyed, and 25% of adults older than 65, have shared their wishes with their doctor. 8
Among older adults with cancer in the United States, ACP prevalence (end-of-life discussion, durable power of attorney, and/or advance directives) ranges from 59%–67%, based on an analysis of data from the National Health and Aging Trends Study, a nationally representative longitudinal cohort study. 9 In a separate study, cancer patients in a palliative care registry were less likely than others (53% vs 73%) to have advance directives. 10 Yet, there is evidence that PCPs may help facilitate the completion of ACP: An examination of deceased patient charts in a US academic medical center found that involvement of primary care physicians in ACP was associated with earlier ACP document completion (ACP completed more than 3 months before death). 11
Little is known about how primary care clinicians and medical oncologists understand the division of labor in ACP; how cancer patients’ end-of-life values and wishes are communicated to providers who share patient care; and how best to transition care for cancer patients who have varied life-expectancies. This formative research aimed to explore experiences with advance care planning among oncology and primary care practitioners and staff in primary/tertiary care settings. The data reported here will be used to develop an intervention to optimize cancer survivorship care by building capacity for coordinated ACP by both cancer specialists and primary care staff.
Methods
This paper focuses on part of a larger qualitative study in which we examined beliefs and practices regarding ACP among oncology and primary care providers and cancer survivors. This study used the National Cancer Institute’s definition of cancer survivor, which considers survivorship to span from the time of cancer diagnosis through the end-of-life. 12 In this manuscript, we use the COREQ tool (Appendix A) 13 to report the results of structured and semi-structured in-depth interviews with family physicians/other primary care practitioners (n = 12) and medical oncologists (n = 12). Sample sizes were chosen based on previous research regarding the optimal number of interviews within a similar group to achieve saturation. 14 Because the study team was interested in how health care providers communicated with their patients about ACP, as well as their understanding of how their patients’ wishes were communicated to other internal and external health care providers, we asked for participants’ experiences so that we might place them into micro, meso, and macro levels of potential intervention. 15 Participants were asked structured questions about their professional experience and ACP practices, while other open-ended questions allowed participants to explore topics in-depth. (See Appendix B for Interview Guide).
The University of Arizona Institutional Review Board approved this study as an exempt project on February 17, 2017 (Protocol #1702178642). Data collection took place in three sites: (1) an academic comprehensive cancer center and (2) two academic family medicine clinics. Interviews were conducted by two researchers (JA or RB), both females with qualitative research training. JA is research faculty in a department of family medicine and has an interest in cancer survivorship within primary care. RB was a graduate student at the time of the study. Physician co-investigators (MM, LA, LG) shared information about the study with colleagues through email and participants responded with their interest in being interviewed. Interviews were conducted with the goal of understanding provider practices related to ACP and the general ACP workflow (e.g., the collection of AD documents). Interviews were conducted one-on-one in private offices or in clinical settings. All interviews were audio recorded, with the permission of the participants, and field note summaries were stored with the recordings for context. Data from the structured questions regarding demographics and ACP practices were summarized with frequencies and percentages. Recordings were transcribed and coded in MaxQDA, a qualitative data management program. The research team did not return the transcripts to participants for review. All notes and transcripts were coded with a code tree composed of a priori and emergent codes, and interim findings guided additional data collection, using a deductive (ideas from prior literature) and inductive (ideas from the transcripts) approach to coding. To achieve intercoder agreement, two team members compared the codes applied to at least two transcripts and discussed disagreement until achieving concordance in code definition and application. Coded segments were reviewed by the team for both sub-themes and connections with other codes. Findings were not shared with participants, although three of the co-authors (MM, LA, and LG) are physicians and represent members of the population studied.
Results
Practitioner Subspecialties.
Provider Demographics and ACP Practices.
When asked how the ACP conversation is documented, most (81%) providers explained that they summarize the conversation in the notes section of the patient’s electronic health record (EHR). Less than half (45%) stated that this information was documented in another way, such as an AD being scanned into the EHR. Providers were often unclear about the policy for storing ADs in the EHR, often reporting that the documents are “scanned into” the EHR but unable to identify how, when, or by whom.
Most Important Advance Directive(s).
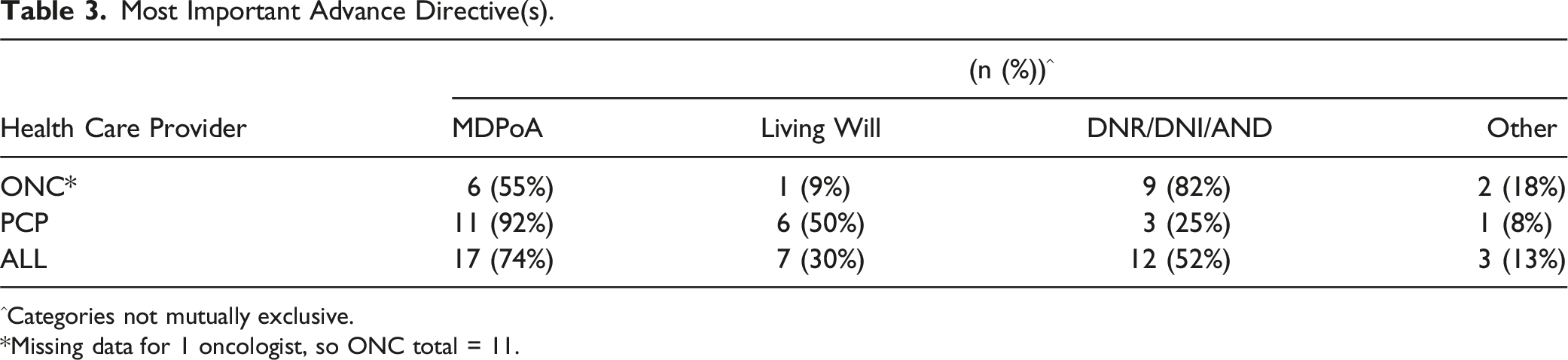
^Categories not mutually exclusive.
*Missing data for 1 oncologist, so ONC total = 11.
Semi-Structured In-Depth Interviews
Based on our framework, which is concerned with understanding the multiple levels of influences on ACP 15 , we organized the themes from the interviews into two broad categories: provider-patient interactions and provider-institution interactions. Provider-patient interaction themes include micro-level influences such as timing the ACP conversation, language-use challenges, and assessing patient goals. Provider-institution interaction themes touch on meso-level influences, including institutional support and workflow. Within these themes, however, there were nuances based on provider specialty.
Provider-Patient Interactions
Timing the Conversation
PCPs and oncologists shared that patient prognosis offers a significant cue for the timing of an ACP discussion. One oncologist [ONC 9] noted: “… patients who come for active chemotherapy after their cancer diagnosis, and we expect that they’re gonna get better and there might be long-term survival, I probably don’t think about [ACP]. But for patients who are in the hospital… and we know that their condition is unstable and they may go downhill at any moment, we definitely have this discussion and we make sure that everything is in the chart.”
Providers also noted that they may introduce the topic of ACP in response to patient/family cues along with prognosis. An oncologist [ONC 12] explained: “Oftentimes I sense that there’s a need from the patient’s perspective for it to be discussed, or honestly the family, caregiver perspective. If I feel the disease state is so advanced that there’s a serious threat to their life, it’s automatically discussed. So it’s a combination of those things.”
Another oncologist [ONC 1] noted that it is important to time these conversations to prepare the family for death, because “If the family’s not expecting it, then they become angry with you.” PCPs echoed the need to respect the provider’s relationship with the patient and family in deciding the timing of an ACP conversation.
Across the board, clinicians noted that a good ACP discussion takes time, so they might not want to do it during a standard clinic visit. PCPs noted that there are often too many other issues to address in a short clinic visit. Moreover, several oncologists emphasized the need for multiple conversations over time, especially for patients whose language they do not speak, to ensure everyone understands the goals of care.
Language-Use
Participants described the need to adjust their approaches to ACP based on patients’ preferred language. As noted, multiple conversations may be essential if the provider does not share a language with a patient and her family. One oncologist noted: “Trying to get everybody on the same page and have the correct information conveyed appropriately can be a bit of a challenge. But I also think that that’s where these ancillary services [telephone or video conferencing] can also really be helpful, and that the consistent message is addressed. It takes more than one conversation usually, in my experience, to really get the message across.” [ONC 2] “You have to dial in [to the phone translation service], the conversation cuts off. Sometimes we have the video monitors and it freezes. It just is a whole other set of barriers to try to get all those conversations in in one visit.” “Translation, especially if I’m tired, it’s just - it becomes a stressful thing…you have to pull out a different way of thinking and speaking and it takes longer, and …it’s more concentration and tense, and it can be very draining in a situation that is already draining, some of those [ACP] talks.”
A primary care physician [PCP 3] emphasized the importance of being sensitive to the family’s role in ACP when the patient speaks another language: “I think [the ACP conversation] just has to be carefully done…Of course with family involvement, but not using a translator [who is] one of the family... It’s pretty important because that frees up the family to have the discussion, number one, and number two, I think that the pressure would be a lot greater on the patient if they were just hearing things through the voice of their family.”
Assessing Patient Goals
Providers also discussed their consideration of patients’ priorities when planning for care, and how those priorities factor into measures to extend their patients’ lives. One oncologist [ONC 6] commented: “Some patients have a goal, they share with me their goal. ‘Doctor, I wanna make it to my first grandchild’s birth, it’s scheduled for this month, or in six months, do you think you can help me do that?’ And sometimes I’ll say, ‘We will aim for that as a priority.’ You know, and then risk/benefit then with the side effects goes more towards the let’s-keep-her-alive-to-see-that-day.”
A primary care provider [PCP 2] noted that the primary care perspective on ACP can contrast with an oncologist’s narrower focus on cancer treatment: “The decision to move into hospice and palliative care is not something I deal with every day, but I have with a few of my primary patients. And I find sometimes I bring it up before the oncologist does. Because, I don’t know, I guess I see the bigger picture. And maybe the patients are expressing to me that they’re kind of ready to, you know, not keep going with this treatment that’s causing them a lot more physical illness than they already have.”
Provider-Institution Interactions
Institutional Support and Workflow
PCPs and oncologists also described their approaches to discussing and documenting ACP discussions, which was not based in institutional policy, per se, but in their professional ethical comportment and decision-making. Oncologists in particular were confident that patients’ ADs were being scanned into the EHR, but they were unclear about the process for ensuring this happens. Commenting on the need to prioritize ACP and setting up a good workflow to ensure it happens, a primary care physician [PCP 1] pointed out the difficulty of establishing processes, both individually and institutionally. They noted: “If you look at the to-do list for all of us, it can vary from 10 things to a hundred things. [It comes down to] how you prioritize and where it falls. It probably just needs to be continually just…not reintroduced… but reminded. I think if you establish these patterns of how you’re gonna implement it and how you’re gonna do it, it’s pretty much second nature. But it takes time to get that into the culture of an organization, or the workflow processes that clinics go through.”
Physicians endorsed team-based approaches, noting that they often work with a social worker to arrange hospice or that a member of the office staff might scan an advance directive for the medical record. However, they also acknowledged that they are unclear about who actually requests ADs and puts them into the record, and they advocated for a systematic approach to team-based ACP instead of the ad hoc approach used currently.
Discussion
While oncologists and PCPs shared many of the same concerns about advance care planning, their unique contexts and specialties influence their approach to ACP with cancer survivors. The number of providers who have and document ACP conversations is high; however, there is a lack of standardization and institutional clarity on how ADs get into the medical record. While oncologists and PCPs were both likely to discuss ACP with their patients, oncologists more often discussed conducting ACP with other members of the health care team (e.g. social workers). Further, there were notable differences between PCPs and oncologists in their emphasis on particular types of ADs, with PCPs highlighting durable medical power-of-attorney documents and oncologists highlighting do-not-resuscitate orders. This difference may be due to differences in patient health, with PCPs seeing primarily healthy cancer survivors and oncologists seeing many patients with life-limiting illness.
In interviews, participants discussed micro-level factors that inform ACP, such as provider-patient communication. Interviews with oncologists highlighted the factors that influenced the timing of and approaches to ACP conversations in the oncology context. Discussions with oncologists revealed a prioritization of the ACP conversation over the receipt of an AD from the patient, with the participants describing careful notation of the conversation in the medical record. Both PCP and oncology participants noted that lack of time in the clinical visit can impact the timing of the discussion, particularly when there are many other medical issues of concern.
Moreover, oncologists and PCPs described listening for their patients’ goals to help guide their decisions about having ACP discussions, with oncologists highlighting patients’ goals of cancer care. PCP respondents emphasized their role in treating the whole person over long periods of time (PCP 8 called it advocating for “the big picture”) when identifying the time to discuss ACP. While the conversation about end-of-life in the oncology context was often precipitated by a change in a patient’s treatment status, PCPs described conversations about end-of-life planning as normalized in the primary care context. This difference may be due to having theoretical conversations in primary care vs existential conversations taking place in oncology care. Taking a process-oriented approach that integrates the different contexts within which patients are receiving care may support a person’s changing medical, emotional, and social circumstances and provide an opportunity for interdisciplinary collaboration in ACP management. 16
The micro-level factors influencing ACP often intersected with meso-level or institutional factors. For instance, providers discussed the challenges of having a conversation about ACP with a patient who speaks a language other than English (or a language that the provider speaks fluently). It might be necessary to schedule a longer visit to accommodate interpretation, and it may require multiple conversations with non-English speaking patients and families. Moreover, these discussions may be taxing, even for clinicians who routinely have these conversations, because they may be more careful about how they share information with an interpreter.
Furthermore, conversations with oncologists emphasized that having multiple conversations about ACP over time with all patients acknowledges patients’ changing medical and psychosocial circumstances. This perspective aligns with what some have called an “impractical challenge of finding an optimal time” for ACP discussions and have advocated for these conversations to be “an iterative process.” 16
Clinician Recommendations
The providers interviewed in this project offered two concrete recommendations to support them in ACP for patients with cancer: (1) develop system-based and team-based approaches to ACP; and (2) provide additional support or time for ACP conversations with patients whose language they do not speak. These recommendations require institutional commitment to patient-centered cancer survivorship care, involving collaborations among a variety of health care providers, including specialists and primary care clinicians. As others have noted, 17 there remain institutional and individual barriers to integrating PCPs into cancer survivorship care. However, ACP provides an opportunity to better integrate specialty and primary care.
Limitations and Next Steps
These qualitative research findings may have limited generalizability due to their focus on clinicians at an academic medical center vs those practicing in community contexts. However, these findings point to potential areas for intervention, similar to areas pointed out by other researchers, including the need to evaluate cancer outcomes based on a team-based approach to ACP and assess interventions that utilize the electronic health record for tracking ACP conversations and documentation. 18
Supplemental Material
Supplemental Material - Practices and Perspectives of Clinicians Regarding Advance Care Planning With People Living With Cancer
Supplemental Material for Practices and Perspectives of Clinicians Regarding Advance Care Planning With People Living With Cancer by Julie Armin, Rebecca Bedwell, Leila Ali-Akbarian, Linda Garland, Bailey Lockwood, and Myra Muramoto in American Journal of Hospice and Palliative Medicine®.
Supplemental Material
Supplemental Material - Practices and Perspectives of Clinicians Regarding Advance Care Planning With People Living With Cancer
Supplemental Material for Practices and Perspectives of Clinicians Regarding Advance Care Planning With People Living With Cancer by Julie Armin, Rebecca Bedwell, Leila Ali-Akbarian, Linda Garland, Bailey Lockwood, and Myra Muramoto in American Journal of Hospice and Palliative Medicine®.
Footnotes
Acknowledgments
The authors would like to thank Ellen Kennedy Estrada for her assistance in data analysis and interpretation, and Jacquanette Slowtalker MPH for her assistance in assembling the manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American Academy of Family Physicians Foundation (grant #G1606JG) and supported in part by institutional funds in support of the FUTURRE-Careers @ UArizona COM Program.
Ethical Statement
Data Availability Statement
Data from this study are not publicly available. Please contact the corresponding author for data requests.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.