
Abstract
Background
Serious illness experiences, i.e. experiencing critical illness personally or through close ones, often influence end-of-life goals of care. Little is known about how older adults with cognitive impairment respond to serious illness experience questions during advance care planning (ACP).
Objectives
Our aim was to demonstrate the utility of serious illness experience questions as a strategy for eliciting goals of care during ACP among older adults with cognitive impairment and care partners.
Methods
Thematic analysis of 92 transcribed ACP conversations involving older adults ≥80 years old who screened positive for cognitive impairment and their care partner. Trained facilitators used a structured ACP conversation guide that probed serious illness experiences.
Results
Participants often described multiple serious illness experiences influencing goals of care, which fell on a spectrum between longevity and comfort. Experiences involving negative clinician interactions provided opportunities for participants to emphasize longevity in their goals of care. Experiences involving severe disability or iatrogenic harm provided opportunities to emphasize comfort in their goals of care.
Conclusions
Older adults with cognitive impairment and their care partners were able to respond to serious illness experience questions, with responses eliciting a spectrum of goals of care. Integrating such questions into ACP for older adults with cognitive impairment may clarify goals of care and improve decision-making for patients and families.
Introduction
People with dementia are less likely to engage in advance care planning (ACP) than people with cancer or organ failure.2,3 As dementia progresses, decisions are often made by family. Best practice recommendations highlight the need to elicit goals of care when cognitive impairment is first recognized and engage family early in ACP conversations. 4 However, the benefit of ACP and how best to encourage participation as cognitive impairment worsens is a point of debate.2,4-7
ACP in dementia is defined as “a process of communication about future care and treatment preferences, values and goals with the person with dementia, family, and the health care team. Continued when the person with dementia becomes unable to make their own decisions.” 8 Typical ACP conversations document end-of-life (EOL) goals of care, a collection of often context-specific preferences falling along a spectrum from maximizing life expectancy (i.e., longevity) to minimizing distress and burden (i.e., comfort). Longevity-focused care includes cardiopulmonary resuscitation (CPR) or interventions whose purpose is to prolong life. Comfort-focused care involves avoidance of interventions which cause discomfort, eg, CPR or surgery.
Serious illness experiences, e.g. personally experiencing serious illness, surrogate decision-making, or witnessing EOL care in loved ones, are important factors shaping goals of care. However, a systematic review found only 20% of ACP conversation guides prompted facilitators to ask questions about serious illness experiences. 5 These questions can evoke memories as a point of shared reference for older adults and families when discussing the nature of decisions and useful limits to decisions. For example, reflecting on a relative with anoxic brain injury after surviving cardiac arrest might assist older adults in clarifying a time limit for cardiopulmonary resuscitation efforts. However, people with dementia are often excluded from studies on ACP readiness and communication strategies.1,9-14
To demonstrate the utility of serious illness experience questions for eliciting goals of care from older adults with cognitive impairment and their families, we thematically analyzed goals of care-related responses to serious illness experience questions during ACP.
Methods
Parent Study, Setting, and Participants
Our study analyzes transcribed audio-recordings of facilitated ACP conversations collected from November 2020 to March 2023 as part of SHARE: Sharing Healthcare Wishes in Primary Care, a single-blind, two-group randomized controlled trial (NCT04593472). SHARE’s primary aim was to test the efficacy of an ACP intervention for improving communication quality between older adults with cognitive impairment and their care partners. The intervention included: (1) an introductory letter from their primary care practice, (2) access to a trained ACP facilitator, (3) person-family agenda setting to align perspectives regarding the family’s role in ACP conversations, and (4) assistance with patient portal registration for the patient and family. 15 Older adults were recruited from eight primary care practices in the Baltimore-Washington area and included English-speaking patients aged 80+ years who screened positive for cognitive impairment, provided written informed consent personally or through a proxy, and regularly attended primary care visits with a family care partner. Cognitive impairment was categorized as mild (32-50), moderate (28-31), or consistent with dementia (i.e., severe, 0-27) based on the Modified Telephone Interview for Cognitive Status (TICS-m). 16 Some older adults could not respond, however their care partner verified their severe impairment. Consent was obtained before data collection. Institutional Review Board approval was obtained from Johns Hopkins University (IRB00242431).
Respecting Choices, an evidence-based ACP conversation guide, formed the basis of facilitator training, supplemented with communication strategies for maximizing participation of older adults with cognitive impairment and family (e.g., providing information in small chunks, soliciting questions and input from both). 17 Facilitators (including a social worker, nurse, and community health workers) were trained to guide ACP discussions virtually or via telephone with approximately 17 questions. All ACP conversations included a standardized serious illness experiences question: “Tell me about any experiences you have had with family, friends, or yourself becoming seriously ill or injured.”
Data Collection and Thematic Analysis
Data included 92 recorded and transcribed ACP conversations with 88 older adults (80+ years), their care partners, and trained facilitators from the intervention arm. First, we deductively coded transcripts into a priori codes aligned with the Respecting Choices conversation guide, e.g. serious illness experience question responses and goals of care-related discussion.17-19 Codes were refined through weekly consensus meetings, added as patterns emerged (inductive coding), and removed if not reflecting the data. Using the final codebook, two independent coders (M.A.S., V.H., G.T., C.G., or P.Z.) coded remaining transcripts, with coding discrepancies (including when no code was assigned by the other coder) resolved in team consensus meetings for all transcripts. Coding was performed using NVivo v.12, and reporting adhered to COREQ guidelines.1,13 Thematic analysis was performed on data coded for both serious illness experience question responses and goals of care-related discussion, with iterative generation and refinement of themes and subthemes and frequent referencing of exemplar quotes based on methods described by Braun and Clarke. 18 To consider the effect of disease severity on conversation dynamics, quotes were labeled by theme and subsequently redivided into two groups based on TICS-m score in the mild/moderate vs severe range (i.e., consistent with dementia).
Results
Characteristics of Older Adults, Care Partners and Advance Care Planning Conversations
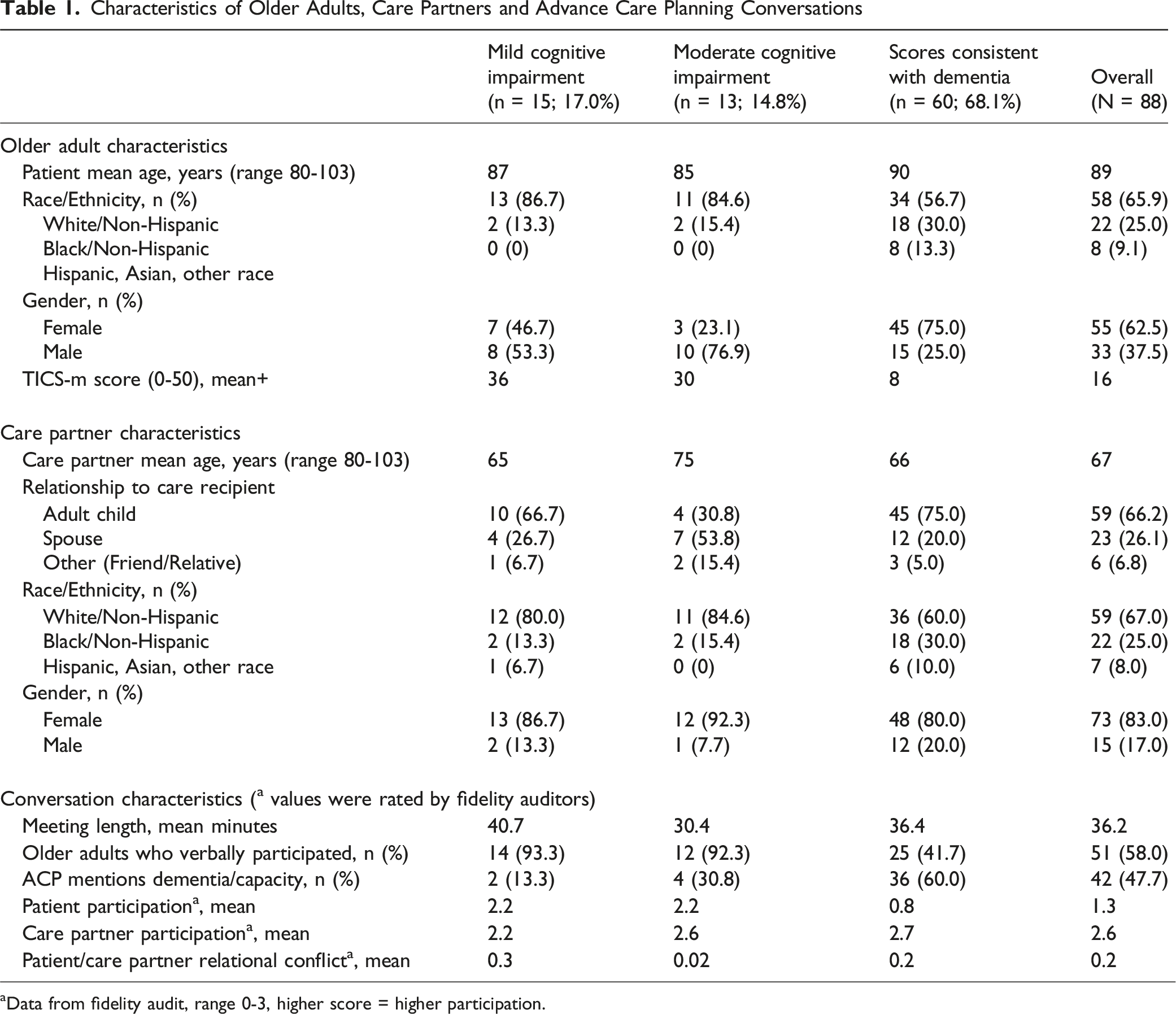
aData from fidelity audit, range 0-3, higher score = higher participation.
Themes, Subthemes, and Selected Quotes by Effect on End-of-Life Goals of Care
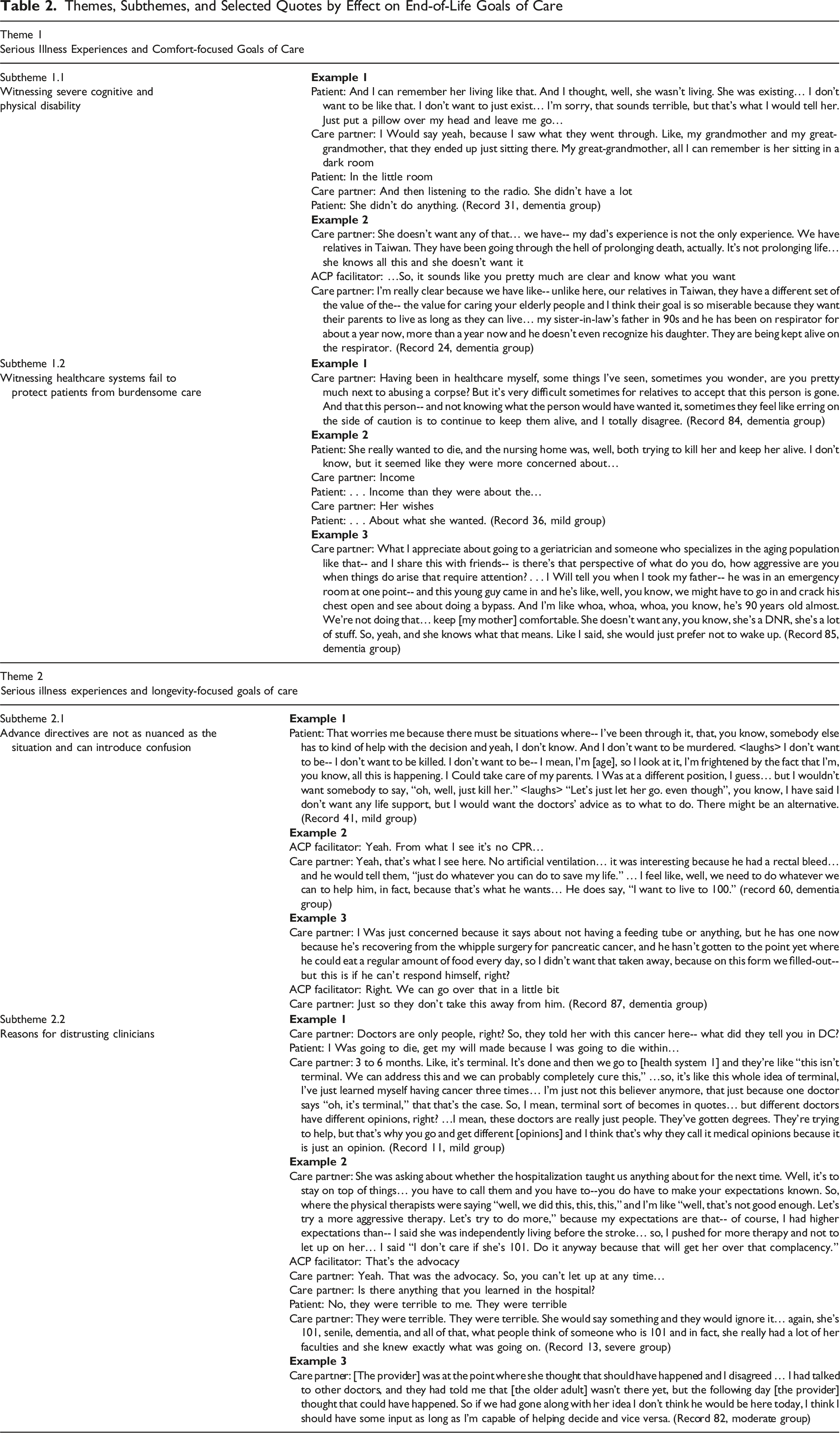
Theme 1: Serious Illness Experiences and Comfort-Focused Goals of Care
Subtheme 1.1 Witnessing Severe Cognitive and Physical Disability
Given the rarity of participation by older adults in the dementia group, their care partners provided most accounts witnessing severe disability (e.g., akinetic mutism or ventilator dependence). However, two older adults in the dementia group engaged deeply with the serious illness experience question, with one stating “She wasn’t living. She was existing… I don’t want to just exist” (Subtheme 1.1, Example 1).
Subtheme 1.2 Witnessing Healthcare Systems Fail to Protect Patients from Burdensome Care
Some participants described longevity-focused care as ‘prolonging death,’ expressing a strong value for quality over quantity of life. Several care partners indicated in remarks that patients needed advocacy to protect them from this care. One care partner expressed moral distress for enabling medically futile care as a healthcare worker (Subtheme 1.2, Example 1). Another patient and their care partner remarked that a relative “really wanted to die, and the nursing home was, well, both trying to kill her and keep her alive,” going on to state that financial interests rather than honoring the relative’s wishes were driving decisions (Subtheme 1.2, Example 2).
Theme 2: Serious Illness Experiences and Longevity-Focused Goals of Care
Serious illness experiences which introduced longevity-focused nuance in participants’ goals of care were more heterogeneous and more often reported by care partners or older adults with less impaired cognition.
Subtheme 2.1 Advance Directives are Not as Nuanced as the Situation and can Introduce Confusion
Some care partners described conflicting statements of preferences made by the older adult, so without clarity, they defaulted to longevity-focused care (Subtheme 2.1, Example 2). One older adult reflected on surrogate decision-making experiences as a source of anxiety, fearing that expressing comfort-focused preferences could bias surrogates to prematurely withdraw care (Subtheme 2.1, Example 1). Experiences of successful intensive treatments made older adults and care partners hesitant to limit future treatments, which they perceived advance directives to do. Care partners pointed to ongoing interventions (e.g., feeding tube) as reasons to continue maximizing treatment options (Subtheme 2.1, Example 3).
Subtheme 2.2 Reasons for Distrusting Clinicians
Serious illness experiences involving negative clinician interactions included receiving an inaccurate cancer prognosis and age-related discrimination. Care partners expressed concerns that clinicians had been dismissive or overly pessimistic about the life expectancy of themselves or a relative, complicating their ability to trust medical counsel (Subtheme 2.2, Examples 1-3) (Figure 1).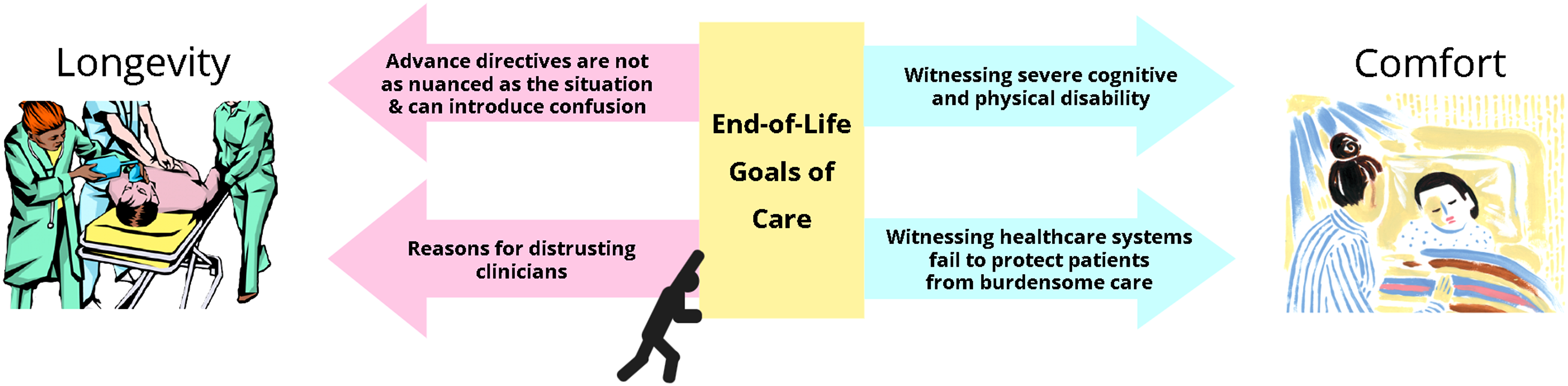
Discussion
This is the first study to explore serious illness experience questions as a strategy for eliciting goals of care during ACP conversations for older adults with cognitive impairment and their care partners. Many people have an unrealistic or distorted understanding of EOL care options, often based on cinema where immediate survival rates after CPR are almost twice that of actual rates.20,21 Personal experiences with serious illness allow people to observe the realities and limitations of medical care. Inviting discussion of these experiences in ACP provides an opportunity to discuss risks and benefits of real-world medical care using examples from people’s lives.
Both positive and negative experiences of EOL care are known to increase readiness to engage with ACP.22,23 Several patients with more severe cognitive impairment conveyed goals of care by describing relatives with severe disability, suggesting that serious illness experience questions may, in select cases, help older adults with dementia during ACP. However, dementia can impair ability to conceptualize one’s future self, a vital skill in ACP. 24 Care partners in mild/moderate and dementia groups emphasized caution when interpreting ACP conversations, particularly when older adults voiced contradicting preferences over time. More investigation is needed into strategies for navigating conflicting statements of preference from patients with cognitive impairment, e.g. utilization of Medical Ethics consultation services.
Previous literature notes that surrogate decision-making experience can heighten awareness of medicine’s limits and facilitate transition to comfort-focused care. 1 Interestingly, surrogate decision-making experiences made transitions more difficult for some participants. Fear that putting preferences in writing can lead to premature withdrawal of care is a known barrier to ACP completion. 11 Clinicians can support those hesitant about documentation by facilitating high quality conversations between patients and family.25,26
Distrust towards clinicians has been documented among older adults with cognitive impairment and their family. 2 Having received an inaccurate prognosis caused care partners to hang on to hope and struggle with accepting medical counsel that EOL decision-making may soon be necessary. Though this impact has been shown in those affected by lung cancer, it has not previously been documented among those affected by dementia. 27 Serious illness experiences involving negative healthcare interactions are important for clinicians to broach in a non-defensive, non-judgmental manner. By listening to patients’ formative medical traumas, clinicians can offer talk therapy, gain insights into microaggressions, and potentially heal rifts between patients and the healthcare system.
Strengths/Limitations
Being a qualitative analysis, the purpose of this study is to generate hypotheses. Therefore, associations between goals of care and disease severity cannot be made. In addition, due to low levels of engagement by older adults with severe cognitive impairment, themes likely overrepresent the perspective of care partners and older adults with mild/moderate cognitive impairment. Many responses prioritizing comfort-focused goals of care (Theme 1) included descriptions of relatives rather than reflections on one’s own illness, most likely because most quotes in this analysis come from the dementia group, of which care partner voices predominate. Also, all participants were English-speaking and 65.9% were Non-Hispanic White, limiting generalizability to the diverse U.S. population. Despite this, our study had notable strengths, using rigorous qualitative methods on a large dataset of ACP conversations. Such empirically derived findings have increased applicability to clinical settings.
Conclusion
ACP provides opportunities to communicate goals of care, but such conversations may be difficult for older adults with cognitive impairment. We demonstrate that serious illness experience questions during ACP can elicit goals of care from older adults with cognitive impairment and family (Supplemental Table 1).
Supplemental Material
Supplemental material - Asking Older Adults With Impaired Cognition and Care Partners About Serious Illness Experiences Can Elicit Goals of Care During Advance Care Planning
Supplemental material for Asking Older Adults With Impaired Cognition and Care Partners About Serious Illness Experiences Can Elicit Goals of Care During Advance Care Planning by Glory H. Thai, BS, Valecia Hanna, MS, Peiyuan Zhang, MSW, Chase Mulholland Green, MPH , John Cagle, PhD, MSW, Jennifer L. Wolff, PhD , Martha Abshire Saylor, in American Journal of Hospice and Palliative Medicine®
Footnotes
Ethical Considerations
Institutional Review Board approval was obtained from Johns Hopkins University (IRB00242431).
Consent to Participate
Written informed consent was obtained prior to data collection from older adults personally or from their healthcare proxy.
Author Contributions
Funding
The author received financial support for the research, authorship, and/or publication of this article; GHT was supported by the NIA #2T35AG026758 Medical Student Training in Aging Research (MSTAR) Summer Program. The SHARE Trial was funded by NIA (R01AG058671).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
De-identified data is available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.